Article Text

Abstract
Introduction Perthes disease (PD) is an idiopathic disorder presenting with avascular necrosis to the femoral head, which frequently results in flattening. Long-term function is directly related to the subsequent femoral head sphericity. Current treatment includes mechanical modalities and surgical procedures, which are therapeutic but are not uniformly able to prevent collapse. The use of the nitrogen-containing bisphosphonate zoledronic acid (ZA) to inhibit osteoclastic bone resorption is aimed at preserving femoral head strength, reducing collapse and thus maintaining shape. The proposed multicentre, prospective, randomised controlled trial intends to evaluate the efficacy of ZA treatment in PD.
Methods and analysis An open-label randomised control trial recruiting 100 children (50 each treatment arm) 5 to 16 years old with unilateral PD. Subjects are randomly assigned to either (a) ZA and standard care or (b) Standard care. The primary outcome measure is deformity index (DI), a radiographic parameter of femoral head roundness assessed at 24 months, following 12 months of ZA treatment (3-monthly doses of ZA 0.025 mg/kg at baseline, 3, 6, 9 and 12 months) plus 12 months observation (group A) or 24 months of observation (group B). Secondary outcome measures are femoral head subluxation, Faces Pain scale, Harris hip score and quality of life. Assessments are made at baseline, 3 monthly during the first year of follow-up and then 6 monthly, until the 24th month.
Ethics and dissemination The study commenced following the written approval from the Human Research Ethics Committee. Safety considerations regarding the effects of ZA are monitored which include the subject’s symptomatology, mineral status, bone mass and turnover activity, and metaphyseal modelling. Data handling plan requires that all documents, clinical information, biological samples and investigation results will be held in strict confidence by study investigators to preserve its safety and confidentiality.
Trial registration number Australian and New Zealand Clinical Trials ACTRN12610000407099, pre-results.
- bone metabolism
- orthopaedics
- endocrinology
- bone disease
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known in this topic?
Perthes disease is a self-limiting disorder but the final hip shape and congruency will determine the long-term outcome.
Age of onset and Lateral Pillar classification play important role for guidance in management. However, outcome of current treatment in large trials is moderate.
Current research is focused on femoral head perfusion and biologics studies.
What this study hopes to add?
To explore the possibility of using bisphosphonate as an effective treatment for Perthes disease.
Introduction
Perthes disease (PD) is an idiopathic childhood osteonecrosis of the femoral head which can affect children from 2 years of age through to skeletal maturity, with peak age of onset of 5 years.1 The annual incidence is unclear with reports ranging from 0.2 to 19.1 per 100 000 of population.2 It is more common in boys than girls, with a ratio of 5:1. In Australia, it is estimated that around 200 patients present with PD each year and >50% are managed at tertiary centres. While it is a self-limiting disease, many children suffer femoral head collapse which leads to painful arthritis requiring hip replacement surgery in adult life.3 The prognosis of children who develop PD varies with age and gender, with those aged over 8 years and women having the worst outcome.4 Children less than 5 years of age have a better long-term outcome.
There are four distinctive pathological stages in the disease process. At first, the femoral head sustains an avascular insult leading to a necrotic phase and growth arrest.5 During the next stage the femoral head starts to collapse. This stage is known as the fragmentation or resorption stage, when the osteoclasts are removing dead bone.6 The usual mechanism of bone remodelling, however, is delayed resulting in lack of bone formation. Therefore, at this moment the femoral head will be mostly cartilaginous, soft and susceptible to any deforming forces placed on it.7 Finally, during the reossification stage, revascularisation by new blood vessels and action of osteoblasts will form new bone. It is here, approximately 2 years after the avascular insult, that the final shape of the hip can be estimated and prognosis can be predicted.8
Current treatment of PD is based on the principle of containing the soft femoral head in its socket during its most vulnerable stage. Mechanical treatment includes bracing or casting, physiotherapy, traction and bed rest. Many of these treatments are mainly symptomatic and do not alter the outcome of PD.4 9 Most surgical interventions involve procedures to place the femoral head in the optimal position within the joint, but not designed to prevent collapse.4 There have been numerous studies assessing the different treatment options but level I studies are lacking.10 Meta-analysis of the literature evaluated 14 level II and III studies and conclude that surgical treatment was associated with superior femoral head sphericity than non-operative treatment in children 6 years of age and older (OR 2.05; 95% CI 1.28 to 3.26).11 Two large multicentre trials represent the landmark studies so far, and the overall results of current treatment at best are modest.4 12 From both trials, number needed to treat analysis affirmed that to have one spherical hip as a result from surgery, at least seven patients needed to be operated on.13
Due to the lack of reliable surgical and non-surgical treatment, research into medical therapy with bisphosphonates has intensified in recent years. Ischaemic necrosis of an immature femoral head leads to an unbalanced repair response, in which there is predominant bone resorption resulting in excessive bone loss compared with new bone formation.7 Antiresorptive properties of bisphosphonate may be able to reduce the osteoclastic resorption in PD, and thus preserve femoral head strength and shape.6 14 15 The preserved femoral head bone could then act as a scaffold on which new bone is formed. Clinical studies in osteonecrotic conditions and preclinical animal models of PD support this hypothesis with preservation of femoral head shape following revascularisation.16–20 We designed the first randomised controlled trial of bisphosphonate therapy in PD, to compare the two treatment arms (a) standard care plus zoledronic acid (ZA) and (b) standard care.
Study aim
The primary aim of this study is to determine the efficacy of intravenous ZA at preserving femoral head shape in children with unilateral PD. Secondary aim is to determine the effect of ZA on hip function, hip pain, quality of life and safety at 24 months.
We hypothesise that five, 3-monthly doses of ZA 0.025 mg/kg (12-month treatment) will inhibit osteoclastic resorption of avascular bone in the femoral head, thus preserving structural integrity and preventing collapse. New bone will then form over the preserved avascular bone, with improved healing at 24 months.
Design and methods
Ethics approval
The study has been reviewed and approved by The Children’s Hospital at Westmead (CHW) Human Research Ethics Committee (09/CHW/153), The Royal Children’s Hospital (RCH) Melbourne (3003A), Lady Cilento Children’s Hospital Brisbane (11/QRCH/10), Women’s and Children’s Hospital Adelaide (REC2259/03/2013) and Princess Margaret Hospital Perth (1807/EP). Written informed consent is obtained from parents and assent from the young people prior to enrolment.
Design
An open-label, multicentre trial of 12 months ZA in children with unilateral PD is designed. The overall design flow chart is shown in figure 1. The CHW is the coordinating centre for the study. Each of the five study sites has an investigator team consisting of a paediatric endocrinologist, paediatric orthopaedic surgeon and a clinical trial coordinator.
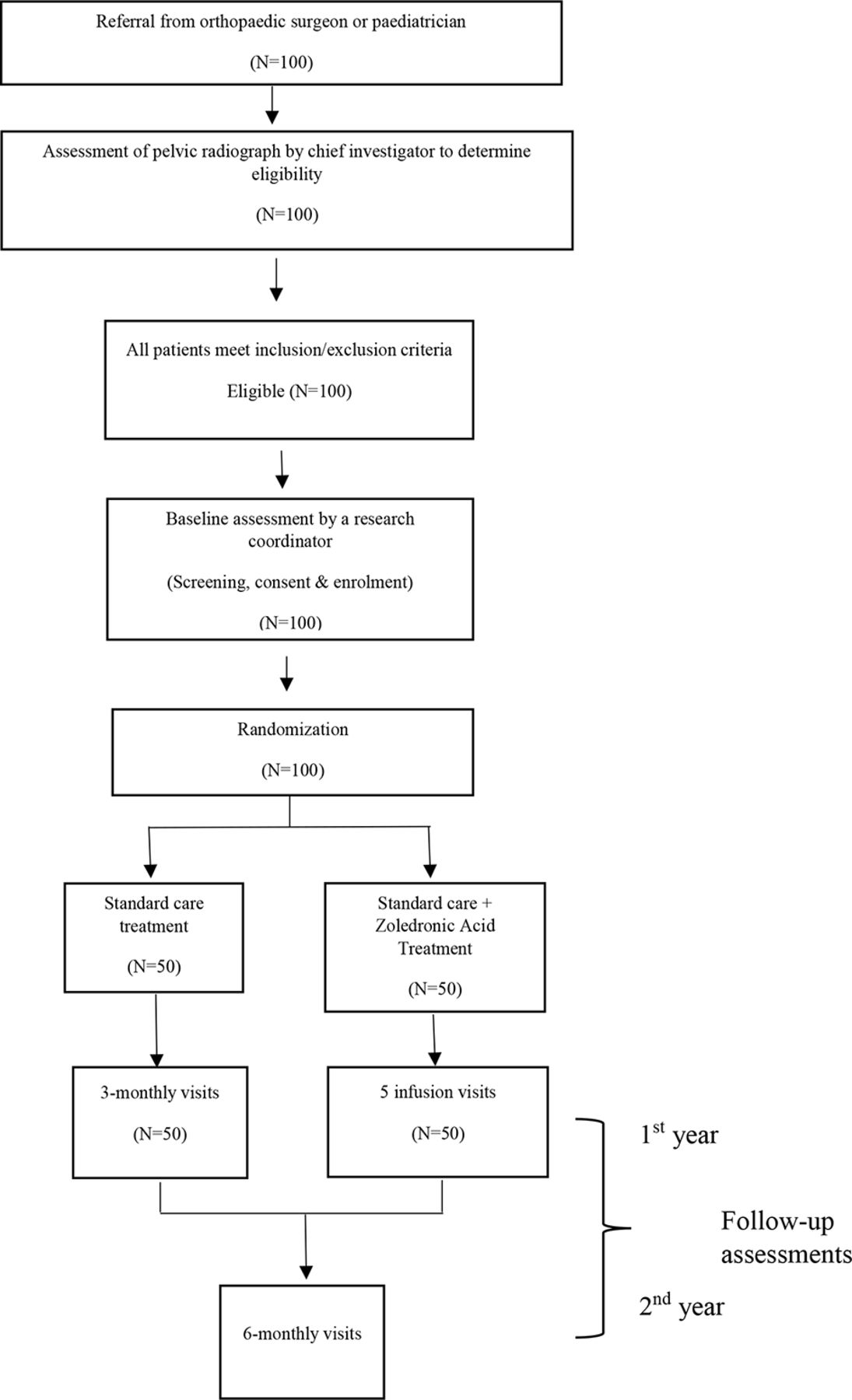
Study design flow diagram.
As the intervention attempts to prevent collapse of the femoral head, children who already have collapsed are not eligible for enrolment. The lateral pillar classification (table 1) is used to define the population such that femoral heads with a lateral pillar >50% of the height of the unaffected side are included (lateral pillar A or B).21 This classification is based on the observation of fragmentation in the lateral third of the femoral head width, as seen on an anteroposterior radiograph.
Lateral pillar classification21
Outcome measures
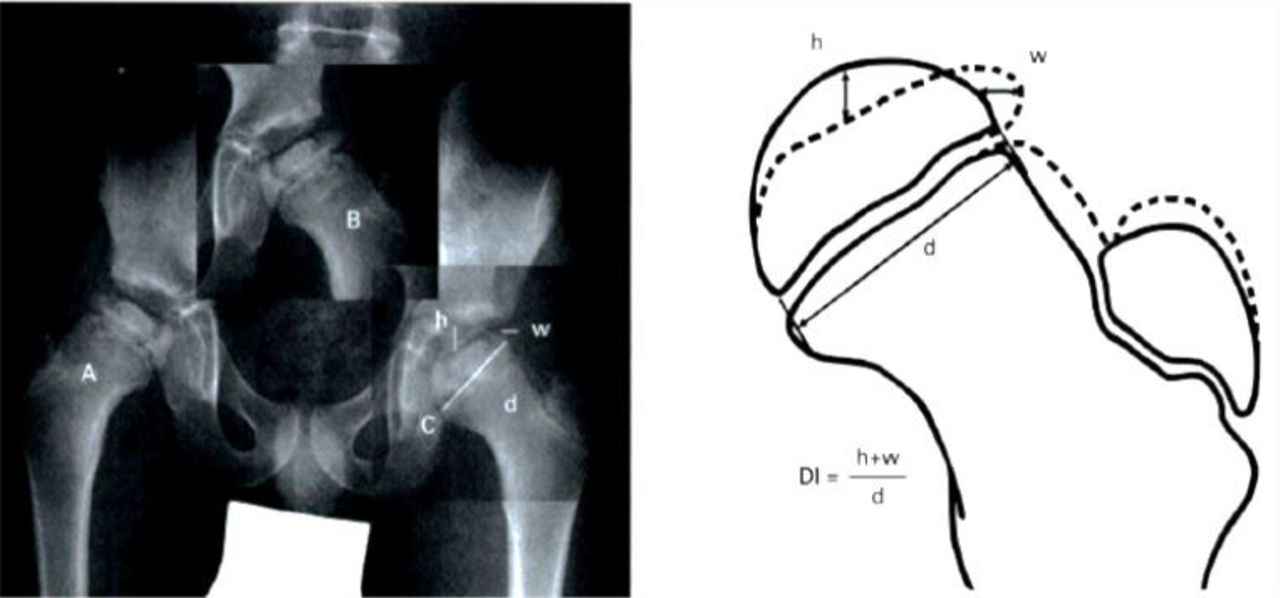
Table 2 summarises the primary and secondary outcome measures. Deformity index (DI) at 24 months is the primary outcome measure. DI (figure 2) is a validated and robust tool developed specifically for the assessment of femoral head roundness in unilateral PD.8 Using an AP radiograph of the pelvis, the DI compares the affected hip to the unaffected side, providing a continuous variable that correlates well with long-term outcome using the Stulberg classification,22 the standard measure of femoral head shape at skeletal maturity. Approximately 60%–75% patients with an aspherical femoral head (Stulberg III–V) have radiographic evidence of arthritis in adulthood.22 In the study by Nelson et al, a DI value above 0.3 was associated with an aspherical femoral head.8 Intra- and inter observer intra class correlation coefficient for DI is approximately 0.98.8 Observer error is reduced by having all measurements performed blinded at 24 months by a single observer. At this time point, the DI has been shown to correspond with the hip outcome at maturity8 and the majority of healing of the femoral head would have occurred.
Outcome measures
{kind=link}
{kind=link}
Deformity index (DI) (reproduced with permission. Nelson D, Zenios M, Ward K, et al. The deformity index as a predictor of final radiological outcome in Perthes' disease. Journal of Bone & Joint Surgery 2007;89:1369-74). The abnormal hip radiograph (A) is flipped horizontally (B) and overlaid on the normal hip image. DI is calculated using the maximum difference in epiphysial height (h) and width (w). The normal hip’s physical diameter (d) is also calculated.8
There are several secondary outcome measures that include the patient’s radiographic parameters, clinical symptoms and examinations and quality of life. These include extrusion index (femoral head coverage),23 Wong-Baker Faces Pain Scale,24 Modified Harris hip score25 and Global Paediatric Outcomes Data Collection Instrument (PODCI) questionnaires.26 As an exploratory variable, bilateral gadolinium contrast hip MRI scans are done at the Screening, 12th month and 24th month visits. Bone age hand X-ray is relevant as there is a known delay in bone age in PD.27 The magnitude of this delay at initial infusion and effect of therapy on this delay is recorded.
Subject enrolment
One hundred (50 in each arm) children 5–16 years of age with unilateral PD and lateral pillar classification A or B will be recruited for the study. Enrolment started in October 2010 and will continue until sufficient numbers are reached. Approximately 200–250 children present with PD each year in Australia, with the majority managed at the study centres and presenting with early disease. To obtain pilot data for the study, the primary study centre offered bisphosphonate treatment using a similar study protocol for a 5-year period to all children with early PD. Over this time, no parent or child refused treatment. Further, children with PD are routinely assessed 3 monthly by orthopaedic surgeons. Study visits will, where possible, be coordinated with clinic visits so as to minimise impact on families.
Patient referrals are being obtained from public or private orthopaedic or general paediatric clinics. Once a potential patient has been referred to the study, de-identified AP pelvis X-ray is sent to the coordinating centre and a single orthopaedic surgeon (DL) determines the lateral pillar classification. If classification A or B, the patients and carer are informed about the study by the patient’s orthopaedic surgeon. The family is then sent the patient/parent information sheet and are contacted by the site study coordinator. The study design, interventions, possible benefits, required commitment, associated risks and harms are explained. Once written consent is obtained, detailed assessment of inclusion and exclusion criteria is undertaken (box 1).
Inclusion and exclusion criteria
Inclusion criteria
Male or female aged 5–16 years inclusive.
Diagnosis of unilateral Perthes disease within the preceding 6 months and with lateral pillar >50% of the contralateral side at the time of enrolment.
Serum 25 (hydroxyvitamin D) >50 nmol/L.
Exclusion criteria
Femoral head avascular necrosis not due to Perthes disease.
Previous treatment with bisphosphonates.
Current pregnancy or sexually active and not using a medically acceptable form of birth control for both male and female participants.
Untreated rickets within 1 year of enrolment.
History of clinically significant organic or psychiatric disease or findings on physical examination, which in the opinion of the Investigator would prevent the patient from completing the study.
At screening: aspartate aminotransferase or alanine aminotransferase>2 x upper limit of normal, thyroid-stimulating hormone outside the normal reference range, GFR <60 mL/min as per the Schwartz formula.
Persistent vitamin D deficiency (<50 nmol/L) or hypocalcaemia (<2.0 mmol/L) despite treatment within 6 weeks from screening.
Randomisation
If the child is eligible for study, randomisation is achieved using minimisation, with strata being gender, treating centre and age (young: 5–8 years and old: 9 and older). Even balance of treatment allocation is crucial as age at diagnosis influences prognosis in PD.4 This is achieved via a web-based system from the NHMRC Clinical Trials Centre, University of Sydney. These methods ensured allocation concealment for the study. Blinding in this study only applies to allocation concealment. A physician independent to the study and blinded to the treatment arm will evaluate the hip radiological outcome.
Sample size
Sample size estimation: from our unpublished pilot data in PD, the mean difference in DI at 24 months between control and ZA cohorts was approximately 25% (from 0.4 to 0.3) with a SD of 0.2. Data were derived from 20 children with PD treated with 12 months intravenous ZA (0.025 mg/kg 3 monthly for five doses; same as in current study), showed preservation of hip sphericity at 24 months as measured by DI compared with age-matched untreated historical controls (ZA=0.28±0.11; Control=0.39±0.19 p=0.03 on two-tailed t-test). For this primary outcome to detect a difference of at least this magnitude at 24 months, a sample size of 100 (50 in the control and ZA arms) is sufficient to have 80% power with 95% CI. This power will accommodate a 20% dropout rate. The sample size calculation was based on an independent, two-sample t-test. The calculated sample size is also sufficient to cover paired t-test analysis within each group (differences between baseline and 24 months). Use of appropriate regression methods will take advantage of data collected over time or multivariate models to adjust for covariates.28 The magnitude of these effects on the secondary outcome variables of hip subluxation, pain and range of hip motion are unknown and no power analysis has been performed.
Current status of trial
The Study is ongoing. To date 70 children have been randomised.
Interventions
Standard care treatment
To lessen compressive forces on the femoral head, all children are advised to non-weight bear using a wheel chair for the first 6–12 months. The implementation is however at the discretion of the treating orthopaedic surgeon. The decision to undertake supplemental orthopaedic management such as traction, casting, bracing or surgery is made by the child’s orthopaedic surgeon at the local treating centre. Such procedures are not a contraindication to enrolment into or continuation within the study. A detailed history of such procedures is collated.
ZA treatment
ZA (for intravenous administration, 5.0 mg/100 mL) solution is supplied by Novartis Pharmaceuticals in vials containing 5.0 mg of drug. The dosage of 0.025 mg/kg is given at a 3-monthly interval for a total of five doses. The calculated dose of reconstituted ZA is diluted in 50 mL of (0.9%) normal saline and infused over 30 min. The maximum dose to be given is 2 mg/infusion. ZA infusions are dispensed by the pharmacist and administered by a nurse or physician. Body weight is measured at each visit for calculation of the dose before it is administered. Our pilot data indicate that this protocol is safe in limiting first-dose hypocalcaemia.29
Concomitant therapy
All subjects (both treatment arms) will receive cholecalciferol 333 IU daily throughout the study. Although this is less than the 400 IU daily recommended in the majority of paediatric guidelines, it equates to one drop of concentrated cholecalciferol formulation and in the experience of the investigators is adequate to maintain vitamin D sufficiency in the study population. Subjects will be encouraged to have a dietary calcium intake of 1000 mg/day. Dietary calcium intake will be assessed by questionnaire at 6-monthly intervals. Compliance with vitamin D supplementation will be evaluated at a central pharmacy by weighing each bottle of cholecalciferol. A drug accountability log and an individual record for each patient are being maintained by the hospital pharmacy.
If vitamin D status is deficient at screening (25(OH) D<50 nmol/L), participants will receive cholecalciferol, 100 000 IU, at weekly intervals for 3 weeks. Participants randomised into the ZA treatment arm, are to have their first infusion when serum 25(OH) D>50 nmol/L, no greater than 6 weeks from screening date. For standard care arm, they are to continue the study visits as per protocol once serum 25(OH) D>50 nmol/L. Calcium supplementation may be administered if diet calcium intake is inadequate.
Measurements
Both control and intervention groups are evaluated following a scheduled assessment plan (tables 3A and B). Assessments consist of clinical, laboratory and imaging for both efficacy and safety outcomes.
Assessment schedule for the control group
Assessment schedule for intervention group
Efficacy outcomes
All radiographic and MRI data will be analysed centrally. DI at 24 months is the primary outcome measure. There is no current gold standard for MRI in PD and examination of MRI scans will be an exploratory variable. The evaluation of the hip range of motion are conducted by a clinician or experienced physiotherapist supervised by investigators at each sites. To minimise variation, each site is trained by a single study therapist from The CHW. Participants are required to complete the Faces Pain Scale and two sets of questionnaires, one on hip scoring (Modified Harris hip score) and another on the quality of life (PODCI), with the assistance of a parent or researcher.
Safety outcomes
Blood analysis of biochemistry and haematology are performed at the local treatment centre at screening and then be performed on the intervention group only at the infusion visits. Bone turnover markers will be performed centrally at the Institute of Endocrinology and Diabetes, The CHW where they are currently available.
Dual-energy X-ray absorptiometry (DXA) of lumbar spine, total body and bilateral femoral neck parameters will be evaluated centrally (CHW). The magnitude of any increase in bone mass from ZA are recorded. If age-matched z-score for total body or lumbar spine becomes ≥3.0, ZA therapy is discontinued. All DXA machines are calibrated using the European Spine Phantom.30 Z-scores are calculated at CHW using Australian reference data.31 32 The effective radiation dose for DXA is <2 micro Sv. Second metacarpal cortical thickness33 and metaphyseal modelling34 are also performed. These assessments provide information regarding bone turnover activity and also distal radial metaphyseal index. Radiographs are sent to CHW where they are evaluated by a single investigator.
The safety of ZA has been studied in children with a variety of bone and mineral disorders including PD.29 Approximately 80% of children experience a 48 hours flu-like illness following their first infusion with aches and pains, fever and headache.29 Symptoms respond to paracetamol. Self-limiting and asymptomatic hypocalcaemia has been reported in approximately 50% of children following their first infusion. To minimise this, subjects must be vitamin D sufficient (25 hydroxyvitamin D >50 nmol/L) and will receive calcium and calcitriol for 3 days following their first infusion. Twelve months of ZA in children with PD and avascular necrosis of bone is associated with mild increase in bone mineral density and reduction in bone turnover.35 There have been no reports of osteonecrosis of the jaw in children. Monitoring of relevant clinical and laboratory safety parameters are undertaken by researchers at each site at the time of each drug administration time point for treated group and at visits for control group. All subjects are asked about any health-related problems at each visit, together with clinical examination and biochemical testing for possible adverse events. An independent data safety monitoring board was established to monitor adverse events. The board will also monitor the rate of recruitment and meet every 12 months or more frequently if required and provides a written report to the investigators.
Medical care
Clinical progress is reviewed by the child’s treating orthopaedic surgeon as per routine practice. This typically entails 3-monthly outpatient visits with clinical assessment and pelvic X-rays. Where possible, X-rays obtained as part of routine care will be used to assess study outcome measures. This will reduce the dose of ionising radiation each child is exposed to.
Statistical methods and analysis plan
Data analyses will be carried out according to a statistical analysis plan, with the primary analysis based on the intention to treat principle. Analysis of the primary outcome will be unadjusted and by means of the two-sample t-test (with appropriate transformation of the data if there is overwhelming evidence of assumption violation). Differences in continuous variables between baseline and follow-up by treatment group, after adjusting for baseline covariates if necessary, will be performed using appropriate (generalised estimating equations) regression methods.
Dissemination plan
Data collection are completed by paper case report forms. These forms and imaging copies are forwarded to the central centre for collation and entering into a purpose built database. All data are stored in a computerised online database accessible only to trial investigators. Clinical and laboratory markers are stored in the patient hospital file, as relevant to standard care. The database are kept on site in the endocrine departments at each institution (Melbourne, Adelaide, Brisbane, Perth and Westmead). Trial data are stored in a de-identified format identifiable only by study number, with codes accessible only to investigators to ensure subject confidentiality and privacy. It will be retained for 25 years after trial completion or to 25th birthday of participants in accordance with therapeutic goods administration act and health privacy principles. Access will only be available to study investigators. At the end of storage computer files will be deleted. Results of the study will be reported according to the CONSORT statement for randomised trials.
Conclusion
This multicentre trial is a crucial step towards improving the treatment of PD. We hope by proving the efficacy, safety and outcome of bisphosphonates in a randomised controlled group of patients, it can be recommended as an effective treatment. Being the first clinical trial for bisphosphonate treatment in PD, we will also collect valuable natural history data, which can be used to inform future research.
Acknowledgments
We would like to thank all medical staff who are involved in the participant’s clinical care and follow-up assessments. Special thanks to Lynne Foxall, Magdalena Gebran and all other study coordinators from all sites. We would also like to thank Novartis for providing zoledronic acid.
References
Footnotes
Contributors CFM, MZ, BF, CTC, DGL and VG participated in all aspects of the conception, design and funding of the study. GD, TH, MJ, ET, CW and AS were responsible to the implementation of the study at their respective site. KJ was responsible for data collection and analysis. All authors were responsible for drafting the manuscript and have read and approved the final manuscript.
Funding The study is funded by National Health and Medical Research Council (NHMRC) and Novartis for provision of drug (Alcasta).
Competing interests DL was a coinventor of the use of zoledronic acid (ZA) for the indication of avascular necrosis of bone (AVN). CHW is the registered owner of the patent of ZA for this indication and in 2003 licensed to Novartis the commercialisation of this patent. Novartis paid royalties to the SCHN (Westmead) in 2003 and DL was a recipient of a proportion of those royalties as per the hospital’s IP policy. Novartis has decided not to continue the development pathway of clinical trials that would be necessary to demonstrate ZA’s efficacy and safety sufficient to register it as a licensed indication for AVN. For this reason, we have initiated an investigator-led study to determine the efficacy and safety of ZA in children with AVN due to Perthes disease. Novartis have not had input into the design of the study but have agreed to provide the drug at no cost. There is no direct conflict of interest for DL because of the ownership/license arrangement of the patent as listed above, as it has lapsed. DL has provided consultancy services to Novartis in the past. This is not an ongoing relationship but was openly declared. DL has ongoing basic science research collaborations with Novartis, Amgen, Celgene and Acceleron, and N8 medical, relating to various pharmaceutical methods for bone repair. He is not currently undertaking any other study of ZA financed in whole or in part by any pharmaceutical company or other party and will be receiving no financial reimbursement for this study. All other trial investigators are involved only in specialist care of their individual patients and as such have no conflict of interest in this trial.
Ethics approval Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.