Article Text

Abstract
Objectives Quantify impaired respiration in currently marketed crib bumpers (CBs), mesh liners (MLs) and alternative products (ALTs) used to attenuate the interaction between the baby and the crib sides and elucidate the relationship between impaired respiration and permeability.
Methods We experimentally quantified carbon dioxide rebreathing (CO2RB) via an infant manikin and air permeability via previously published test protocols, in commercially available CBs, MLs and ALTs.
Results Differences in CO2RB in ML (median [m]=8.2%, 25th percentile [P25]=6.8, 75th percentile [P75]=8.6), ALT (m=10.5%, P25=9.8, P75=10.7) and CB (m=11.6%, P25=10.2, P75=14.3) were significant (p<0.0001). For comparison, manikin tests with a pacifier yielded CO2RB of 5.6%–5.9%, blanket draped over the face/torso yielded CO2RB of 7.7%–8.6% and stuffed animal in various positions yielded CO2RB from 6.1% to 16.1%. Differences in permeability between ML (m=529.5 cubic feet per minute [CFM], P25=460, P75=747.5), ALT (m=29.0 CFM, P25=27.7, P75=37.7) and CB (m=46.6 CFM, P25=30.1, P75=58.7) groups were significant (p<0.0001). CO2RB was poorly correlated with air permeability (max R2=0.36). In a subset of tests, CB CO2RB increased by 50%–80% with increasing penetration force, whereas the ML CO2RB was nominally unchanged.
Conclusions Government agencies and standards organisations are presently considering regulation of bedding including CBs. As paediatricians are consulted in the development of such regulations, our findings that permeability by itself was a poor predictor of CO2RB should be considered.
- crib
- rebreathing
- CO2
- SIDS
- bumper
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Bedding, pillows, bumpers and toys have been identified as suffocation risks to children in cribs. The tendency of crib mattresses and mattress covers to induce carbon dioxide (CO2) rebreathing has been characterised experimentally in the literature.
The firmness of the mattress and the ability of the mattress to form a seal around the baby’s face as important factors in generating CO2 rebreathing.
What this study hopes to add?
This study characterises CO2 rebreathing in crib bumpers, mesh liners and other products used to mitigate the crib-to-baby interaction. Product permeability, which has been proposed as a regulatory metric, is not an adequate predictor of CO2 rebreathing.
The seal and penetration force are important factors as found in mattresses and other bedding materials by previous authors.
Introduction
The environmental conditions that lead to sudden infant death syndrome (SIDS)/sudden unexpected infant death (SUID) during sleep vary, including prone sleeping, mattress firmness, crib-sharing, soft objects and loose bedding in the sleep area, smoke exposure and alcohol and illicit drug use of the mother.1 Crib bumpers (CBs) have been implicated in 48 deaths between 1985 and 2012, including 23 deaths between 2006 and 2012.2 Twenty-five of the 48 cases were found to have the ‘bumper alone’ as the cause of death, including 13 deaths from infants wedged between a bumper and crib mattress and 12 deaths with the infant’s face against a bumper without wedging, with all cited as impeding respiration. This impaired respiration associated with CBs is the focus of this report.
Our overarching goal is to examine the environmental and design factors that lead to impaired respiration in products that are used to mitigate harmful interactions between the side of the crib and the infant, and CBs are one such product. In addition, it has been suggested that mesh liners (ML) may mitigate some of the problems found with traditional CBs, as such MLs have been cited as ‘breathable and thin’.2 Thus, the purpose of this study was to quantify impaired respiration in currently marketed liners, bumpers and alternative (ALT) products and elucidate the relationship between impaired respiration and permeability of the sample.
Methods
No patients were involved in this study. All products were purchased from consumer retail outlets. By material and construction, we categorised each product into one of three categories: (1) MLs were 4 mm thick or less and were constructed of mesh fabric (1–2 mm openings) and an open fibre scrim, (2) ALT products had two exterior mesh fabric layers more than 4 mm in total thickness and may have sometimes included a fill of either padding or additional mesh sandwiched between them and (3) CBs consisted of a padded fill material, of thickness ranging from 10 to 55 mm, sandwiched between two exterior non-mesh fabric layers (figure 1).

Exemplar products tested: crib bumper (top), mesh liner (middle) and alternative (bottom).
Carbon dioxide rebreathing (CO2RB) Studies
Consistent with studies used to examine impaired respiration in infants during sleep,3–10 we used CO2RB as the metric for quantifying impaired respiration.

Anthropomorphic rebreathing surrogate (ARS) used in all testing.
CO2RB was assessed via an anthropomorphic rebreathing surrogate (ARS).3 10 The ARS makes use of a mechanical ‘lung’ of 120 mL total volume, actuated at a frequency of 45 breaths per minute and 35 mL tidal volume. The volume of the tubing connecting the lung to the manikin’s nose is similar to the infant trachea with a resistance to airflow of 40 cm H2O/L/s.
As the manikin breathes in and out of its nose, carbon dioxide is metered into the lung to simulate CO2 produced by metabolism. Interactions between the manikin’s face and external materials causes a change in the CO2 concentration in the lung, which is measured by withdrawing a very small sample and measuring the CO2 concentration (Fuji Electric Non-Dispersive Infrared Gas Analyzer, Type ZRF). Rotameters ensured constant flow rates (figure 2).
ARS postures were developed from real-world infant death and near death cases,2 11 where the overarching observation was that the face was up against the CB with or without another object applying force to the infant. Given that our goal was to evaluate the CO2RB that is affected by the material and structural characteristics of the sample, and not the mattress or other bedding, we focused our study on the scenario where the infant lying on its right or left side with their coronal plane parallel to the sample and the manikin face against the sample. Discussed later, we also examined the possibility of increased penetration force caused by an object pressing the face into the sample.
For a repeatable test setup, we changed the orientation of the crib to take advantage of gravity to apply the forces to the ARS body. This was accomplished by turning the test apparatus 90° on its side with the manikin face down on the sample. In order to prove out this approach, we conducted several tests with different samples with the crib in the normal position, and then repeated those same tests with the crib side rotated 90°. Using p<0.01 as the level of significance, none of the tested cases achieved a statistically significant difference (sample 3: p=0.03, sample 10: p=0.89, sample 13: p=0.72, sample 15: p=0.77) between the horizontal and vertical positions (online supplementary figure 1). The percent change in CO2RB between the horizontal and vertical crib side positions was 2.41% across all samples. An appreciation for the effect size can be gained from online supplementary figure 1 (available online). Thus, we conducted all experiments with the crib in the horizontal position.
Supplementary file 1
ARS head mass was 2 kg, which is in the range of a 1 to 6 month old.12 13 We recognise that 2 kg is on the higher end of the range of the head masses, but this simulates the potential worst case scenario where exogenous forces (wedging, crib-sharing partner or other objects) push the face into the sample. We used a slatted crib with flat slats 40 mm wide and a 56 mm gap between edges of adjacent slats; in all tests, we placed the tip of the nose of ARS centred in the gap between the slats.
For each sample, a baseline measurement was taken with the ARS free-breathing and in the centre of the crib away from the sample. Then, the baby was placed prone on the sample, and the manikin remained in this position until the CO2RB reached a stable value, after which the CO2RB measurement was recorded and the manikin returned to the free-breathing position in the centre of the crib. After the CO2RB returned to baseline conditions, the experiment was repeated an additional two times for a total of three measurements per sample. The time between measurements was 2–3 min.
For comparison with the ML, ALT and CB samples, we tested several typical conditions found in unattended sleeping children that have been previously studied in vivo or with an ARS,14 15 as well as discovered in retrospective death case studies.16 17 The first was an infant put to bed supine in the centre of the crib with a pacifier in their mouth. The second was the condition where a receiving blanket, which could become unwrapped from a swaddled baby placed to bed, was draped over the entire face and torso (online supplementary figure 2). In addition to these aforementioned conditions that are plausible when compliant with the safe sleeping recommendations,1 we also tested the condition where a stuffed animal was placed in the crib with the child, which would be considered unsafe by the safe sleeping recommendations (online supplementary figure 3). It is important to note that blankets and stuffed animals have been associated with infant death cases.18
Permeability studies
In addition to CO2RB testing with the ARS, each sample was subjected to an air permeability test19 that measured the volumetric flow rate of air passing perpendicularly through a known area under a prescribed air pressure differential between the two surfaces of a material. In the context of crib bedding, the air permeability test quantifies the resistance of a material to allow the baby to breathe the air on the contralateral side of the material. Each product was tested 10 times.
Data analysis
Kruskal-Wallis equality-of-populations rank test was used to compare CO2RB and permeability results across the three product categories. Across all samples, the relationship between median CO2RB and median permeability was quantified via exponential, linear, logarithmic, polynomial and power regression models. All models were built by least squares methods, and permeability was the independent variable, while the CO2RB was the dependent variable (table 1).
The mathematical model formula and coefficient of determination for all models used to evaluate the relationship between permeability (x) and CO2RB (y)
To examine the effect of penetration force into the sample on CO2RB, we evaluated CO2RB on a subset of samples with variation on the force that the head places on the sample. The manikin was placed prone on the sample (online supplementary figure 4). Then, 200 g of steel shot was added to the manikin head through a hole in the occiput, which increased the force applied by the face to the sample. Then, CO2RB measurements were made. Additional steel shot was added to head in 200 g increments for a total added mass of up to 2000 g, with CO2RB measurements at each 200 g increment.
Results
CO2RB Studies
Eighteen products were tested including 5 MLs, 3 ALTs and 10 CBs. Differences in CO2RB in ML (median [m]=8.2%, 25th percentile [P25]=6.8, 75th percentile [P75]=8.6), ALT (m=10.5%, P25=9.8, P75=10.7) and CB (m=11.6%, P25=10.2, P75=14.3) were statistically significant (p<0.0001). Ranges of CO2RB overlapped between product categories (figure 3, top). CO2RB values vary widely in CB products, compared with ML and ALT products (figure 3, top). The supine infant centred in the crib with a pacifier in its mouth yielded CO2RB measurements of 5.6%, 5.85%, 5.8% and 5.55%, and the condition with the receiving blanket draped over the entire face and torso yielded CO2RB values of 7.7%, 7.7% and 8.55%. The stuffed animal yielded the following results: when positioned on the nose of the infant CO2RB was 7.4%, 6.4% and 6.55%; proximal to the face CO2RB was 6.1% and 6.2%, and on the face CO2RB was 11.65%, 8.55% and 16.1%.

CO2RB (top) and permeability (bottom) results for mesh liners (ML), alternative products (ALTs) and crib bumpers (CBs). CO2RB, carbon dioxide rebreathing.
Permeability studies
Fifteen of the 18 products tested for CO2RB were available at the time of air permeability testing: four MLs, three ALTs and eight CBs. Differences in permeability between ML (m=529.5 cubic feet per minute [CFM], P25=460, P75=747.5), ALT (m=29.0 CFM, P25=27.7, P75=37.7) and CB (m=46.6 CFM, P25=30.1, P75=58.7) groups achieved statistical significance (p<0.0001). Ranges of permeability did not overlap between product categories (figure 3, bottom).
CO2RB was poorly correlated with air permeability (figure 4). Data were fit to exponential, linear, logarithmic, polynomial and power regression models, and none produced a coefficient of determination (R2) greater than 0.36 (table 1).
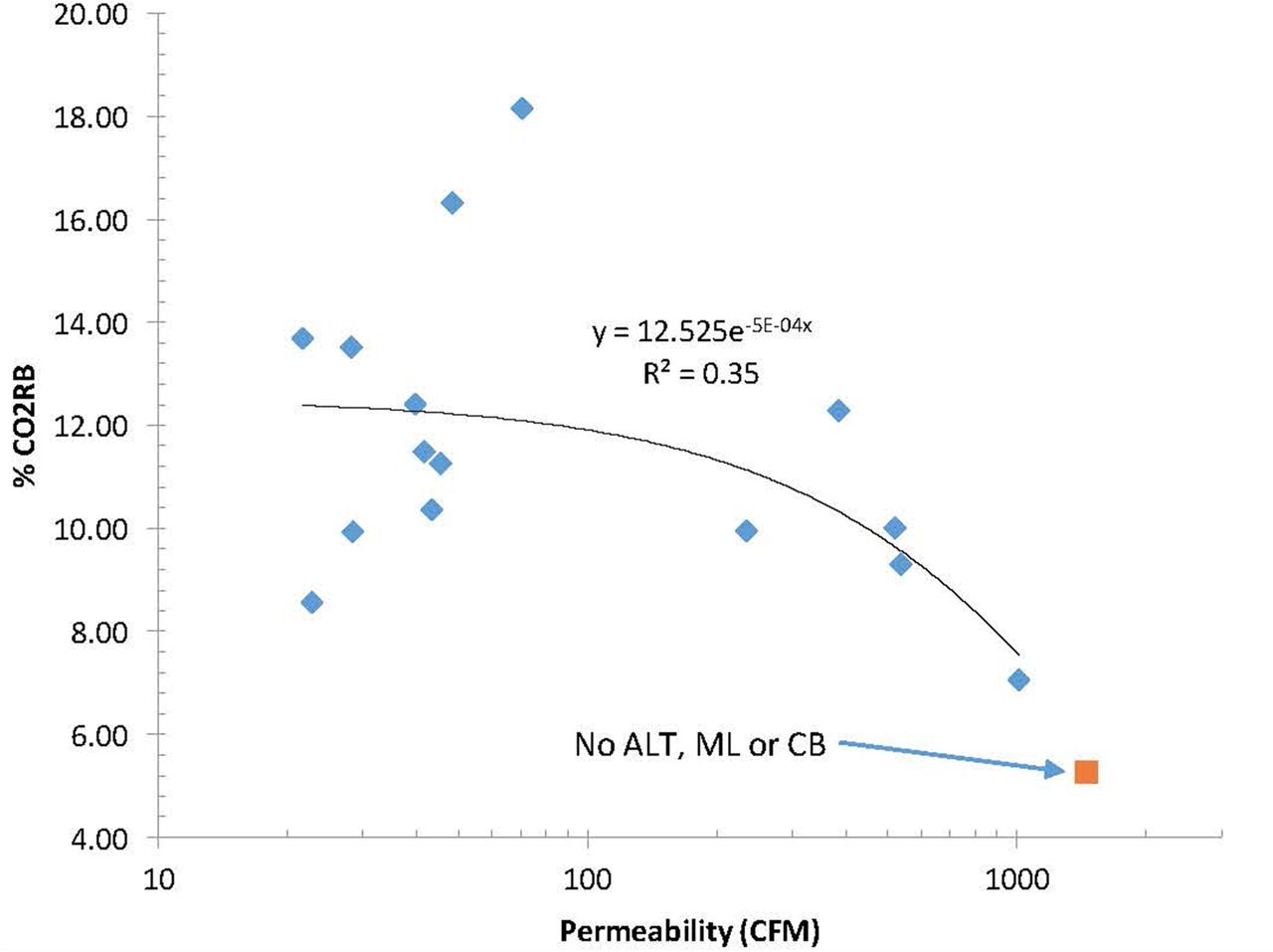
CO2RB versus permeability for all products tested with both measures (n=15). ‘No ALT, ML or CB’ case shown for reference purposes, showing CO2 concentrations and volumetric flow rates of test apparatuses without a test sample. Exponential regression model shown. ALT, alternative; CB, crib bumper; CO2RB, carbon dioxide rebreathing; ML, mesh liners.
Three products (one ML and two CBs) were tested with incrementally increasing penetration force (figure 5). Both CBs showed a higher initial (no weight added to head) CO2RB than the MLs, consistent with findings described above. Of note, the CB CO2RB increased by 50%–80% with increasing weight, whereas the ML CO2RB was nominally unchanged across the range of weight added to the head.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
CO2RB with manikin prone on ML or CB, with varying mass added to the head. CB, crib bumper; CO2RB, carbon dioxide rebreathing; ML, mesh liner.
The raw data from figures 3 and 4 have been supplied in the online supplementary material.
Discussion
Filiano and Kinney20 have posited a ‘Triple Risk Model’ where three conditions are necessary to result in SIDS—a critical developmental period, a vulnerable infant and an exogenous stressor. This model posits that ‘infants who eventually die of SIDS may appear normal clinically, but their vulnerability lies latent until they enter the critical development period between 1 and 6 postnatal months and are subject to an exogenous stressor which overwhelms already compromised cardioventilatory or other homeostatic controls’. The Triple Risk Model remains as a foundational paradigm in the analysis of infant death cases.21
One essential element of the Triple Risk Model is the exogenous stressor. In the context of deaths attributed to bedding including CBs, the exogenous stressor is impaired respiration that arises when the infant’s mouth and nose are pressed against a bedding material. It has been shown that some infants exposed to such conditions attempt self-rescue by increasing their tidal volume.9
The ML, ALT and CB product materials are mediums that store gas and thus exhaled CO2 is stored within the product, leading to the potential for CO2RB. Though the stored CO2 dissipates from the product to the atmosphere in accordance with Fick’s laws of diffusion and the permeability of the material, the rate of dissipation may be low enough that by the time the next breath begins, the baby inhales the gas stored in the sample from the previous breath cycle. Similar to studies of other bedding products,3 4 6 22 we hypothesised that CO2RB would be influenced by the tendency for the CO2 to become retained within the fibres of the ML, ALT or CB, which in turn is likely related to the gas permeability of the sample.
We empirically quantified CO2RB and permeability in ML, CBs or ALT products. We found that MLs had the lowest CO2RB and the highest permeability, compared with ALT and CB products. In addition, we found that permeability by itself was a poor predictor of CO2RB overall, though permeability did distinguish between MLs and ALTs or CBs. Of note, the CO2RB was higher in CBs than ALTs, but the permeability of ALTs was higher than CBs. This inverse relationship between CO2RB and permeability in CBs and ALTs, likely fueled the poor correlation between CO2RB and permeability shown in figure 4.
Patel and colleagues9 studied the inspired CO2 in infants face-down on bedding and demonstrated that CO2 rebreathing was predicated on the seal made between the face and the bedding material. Thus, as in the case of bedding, we posit that CO2RB in MLs, ALTs and CBs is predicated on both the permeability of material, which dictates the rate at which gas diffuses out of the sample, and the seal that the nares make with the sample, which dictates how much of the exhaled gas is directed into the sample. To be clear, by a ‘seal’ we mean that the skin of the face surrounding the nares makes nearly continuous contact circumferentially around the nares, such that exhaled gas is primarily directed into the sample and not into the atmosphere. During our testing, we noted that wrinkles or valleys sometimes developed in the sample when the baby was placed face down in the sample, and these wrinkles and valleys created air channels that break the aforementioned seal. We anecdotally observed that wrinkles and valleys sometimes occur more frequently in the thicker samples, likely leading to the variability observed in the CO2RB of the CBs as compared with the ALTs and MLs (figure 3).
To examine this further, we tested CO2RB with the manikin face down on a sample with varied weight added to the head to modulate penetration force. The CB CO2RB increased by 50%–80% with increasing penetration force, whereas the ML CO2RB was nominally unchanged across the range of penetration force. This latter point suggests that the ML has an invariant and thus more predictable performance across a wide range of environmental force conditions. This has implications for crib-sharing situations, which are discouraged by the 2016 American Academy of Pediatrics guidelines1 but which occur in the field, and sleeping situations with other objects or bedding. That is, the ML shows a stable CO2RB that is independent of applied force, and thus should a baby’s head be pressed against the ML by a crib-sharing partner or other object the CO2RB will remain at unweighted head levels (figure 5). In contrast, CB CO2RB increases with applied force, indicating that increased exogenous force to the back of the head (such as in crib sharing or wedging2) may lead to unpredictable and elevated CO2RB levels in CBs.
Approximately 1 in 7 infant deaths and 1 in 3 postneonatal deaths in the USA were attributed to SUID in 2010.23 SUID is defined as any sudden and unexpected death, whether explained or unexplained occurring during infancy. Following investigation, SUID can be attributed to a cause of death (suffocation, asphyxia, entrapment, infection and so on). SIDS is a subcategory of SUID and is the assigned cause of death when, after a thorough investigation, a cause of death cannot be explained.24 The practice of investigation, autopsy and the assigning of causes of death on the death certificate vary greatly by geographic region. Thus, the national data in the USA lacks consistency in the definitions of infant death aetiologies.2 With the aforementioned limitations, we can still gain some information from national cause of death data. In 2015, SUID deaths were attributed to the following aetiologies: SIDS (43%), accidental suffocation and strangulation in bed (25%) and unknown (32%).25
Scheers et al 2 queried the Consumer Product Safety Commission databases for CB-related deaths and injuries between 1985 and 2012. In that study, 32 deaths were attributed to the CB alone. These included the following scenarios: 13 cases where ‘infants wedged between a bumper and crib mattress’, 12 cases where the ‘infant’s face against a bumper without wedging’, 3 cases where the ‘infant’s arm caught between the bumper and the mattress/side rails found with their faces pressed against a bumper’. In addition, four cases of deaths were not related to CO2RB (fall and strangulation).
In that same study, 16 deaths were attributed to the CB and another object. These include nine deaths from ‘wedging between a pillow and a bumper’, five deaths from ‘infants wedged between a bumper and a recliner’, one death in a ‘crib depression where the bumper prevented the infant from turning her face to the side to breathe,’ and one death from ‘wedging between a co-sleeping twin and a bumper’.
In addition, the authors reported 11 apparent life-threatening events attributed to the CB: two infants ‘found with their faces pressed into bumper’, one case of an infant ‘wedged between a bumper and mattress’, one case of an infant ‘found under a bumper’ and seven additional cases that were not related to CO2RB (choking, strangulation and fall).
CO2RB has been studied in human volunteers (as opposed to experimental surrogates) in controlled settings. Hunt7 studied 46 infants (2.6±0.3 months) who were clinically diagnosed as having a near-miss (N-M) SIDS event and 21 control subjects (2.1±0.4 months) exposed to 5% CO2/normoxic breathing. The definition of N-M SIDS included children with one or more observed episodes of sleep aponea associated with marked pallor or cyanosis and requiring at least minimal stimulation. Control subjects were asymptomatic for sleep aponea. Of note, the authors found that infants with a clinical N-M SIDS history and diminished ventilator response slopes have as a group a concomitant abnormality in arousal (as defined by absence of agitation, eye opening or crying). It is difficult to compare these findings with the data presented herein, as nasal end-tidal partial pressure CO2 was reported by Hunt, whereas we measured percent CO2 in the lung, and the infant respiratory rate and volume was not controlled by Hunt, whereas our ARS rate and volume remained constant. However, Hunt’s finding that diminished arousal was found in infants exposed to elevated CO2 levels supports our use of CO2RB as a metric for impaired respiration.
Though the study of rebreathing in CBs is limited to the data presented herein, there is enough similarity to rebreathing with crib mattresses that the methods and data from crib mattress rebreathing experiments can be used as basis for the current study. Most notably, Kemp et al 4 measured CO2RB and mattress softness. CO2RB was assessed using a manikin with CO2 measurement capability, with the manikin prone on the mattress. The manikin head was weighted to physiological range. Mattress softness was measured by estimating the contact area between the face and manikin. Of note, the authors found a correlation between softness and CO2RB. Similarly, Kanetake and colleagues22 developed a spherical head-form that accurately and repeatably assessed softness via measurement of contact area. Using a CO2RB manikin, the authors concluded that it was difficult to estimate the rebreathing potential of the bedding on the basis of its softness. Based on these studies and the aforementioned clinical studies of infant response to CO2RB, we theorise that two conditions are necessary for storage and rebreathing of exhaled gases in bedding:
An adequate seal is made around the mouth and nose such that exhaled gas is directed into, and gas can be inhaled from, the storage medium (the CB, ML or ALT).
The storage medium has sufficient thickness and density and insufficient permeability to make previously exhaled gas available for inhalation.
Limitations
Our research is subject to certain limitations. First, the mechanical compliance (stiffness) of the ARS face has not been shown to have fidelity to the human infant, nor has the variability in human facial anthropometry been examined; both of these factors may influence the interaction between the face and the sample. Second, the ARS has not been validated to show that the CO2 measurements correspond with similar measurements in human infants. To mitigate these two limitations, we have used the ARS to compare the performance of various samples and with other sleeping conditions (blankets, pacifiers and stuffed animals); without additional research, none of the CO2RB values reported herein should be interpreted as that which would be expected in a human infant. Further research is needed to validate the ARS measurements against human infants. Finally, our ARS measured CO2 concentration in the lung, not in the blood. That said, we note that end-tidal CO2 has been shown to be correlated with arterial blood CO2 measurements in infants with respiratory distress,26 and thus we feel our CO2 measurements are reasonable estimate of relative hypercarbia.
Supplementary file 2
Supplementary file 3
Acknowledgments
The authors gratefully acknowledge the contributions of R T Cimini of Bureau Veritas for conduct of the permeability tests, Matthew Howsare (Mintz Levin PC) formerly of the Consumer Product Safety Commission and Susan Klobuchar and Steve Marton of BreathableBaby LLC for insight and guidance on background and study design.
References
Footnotes
Contributors MRM and ML designed and conducted all experiments. ML was primarily responsible for design and fabrication of the experimental apparatus. MRM was primarily responsible for data analysis and writing the manuscript, with editing by ML.
Funding This research was supported by BreathableBaby, LLC, which provided salary support for study design, data analysis and manuscript preparation, and the costs of laboratory testing. At the time of project inception and before data collection began, the sponsors and the authors decided to submit the data for publication in the peer-reviewed literature.
Competing interests The authors report personal fees from BreathableBaby, LLC, during the conduct of the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data from figures 3 and 4 are available in the online materials.
Patient consent for publication Not required.