Article Text

Abstract
Objective Chronic fatigue syndromemyalgic encephalomyelitis (CFS/ME) is relatively common among children and adolescents; however, little is known about the physical activity levels and patterns of this population. The aim of this study was to examine the underlying patterns of physical activity among youth with mild-to-moderate CFS/ME. Cross-sectional associations between physical activity patterns with self-reported physical function, pain, fatigue, anxiety and depression were also examined.
Design Baseline cross-sectional data from the Managed Activity Graded Exercise iN Teenagers and pre-Adolescents randomised controlled trial.
Patients Children and adolescents (aged 8–17 years) diagnosed with mild-to-moderate CFS/ME who wore an accelerometer for at least three valid weekdays.
Analyses Latent profile analysis was used to identify physical activity patterns. Linear regression models examined associations between physical activity classes and self-reported physical function, pain, fatigue, anxiety and depression.
Results 138 children and adolescents (72.5% females) had valid data. Overall, participants did less than half the government recommended level of physical activity for children and adolescents, but not all were inactive: three (2.2%) did more than 1 hour of physical activity every day, and 13 (9.4%) achieved an average of 60 min a day. Adolescents (≥12 years) were less active than younger children, but activity levels were similar between genders. Three latent classes emerged from the data: ‘active’, ‘light’ and ‘inactive’. Compared with being ‘inactive’, being in the ‘light’ class was associated with greater self-reported physical function (10.35, 95% CI 2.32 to 18.38) and lower fatigue (−1.60, 95% CI −3.13 to −0.06), while being ‘active’ was associated with greater physical function (15.26, 95% CI 0.12 to 30.40), but also greater anxiety (13.79, 95% CI 1.73 to 25.85).
Conclusions Paediatricians need to be aware that physical activity patterns vary widely before recommending treatment.
Clinical trial registration ISRCTN registry: 23 962 803
- chronic fatigue syndrome
- physical activity
- children
- adolescents
- latent profile analysis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Between 0.1% and 2% of secondary school-aged children are affected by chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME).
Vigorous exercise can trigger CFS/ME symptoms, leading to some patients avoiding physical activity.
Physically active patients with CFS/ME report lower levels of fatigue than their inactive counterparts.
What this study adds?
Children and adolescents with chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME) are less active than the general child population, but not all are inactive. 9.4% of participants met physical activity recommendations.
Compared with being ‘inactive’, ‘active’ children reported greater physical function but increased anxiety, while ‘lightly’ active children reported greater physical function and reduced fatigue.
Paediatricians need to recognise that physical activity varies between patients with CFS/ME when they recommend treatment.
Introduction
Chronic fatigue syndrome or myalgic encephalomyelitis (CFS/ME) is characterised by persistent or recurrent debilitating fatigue lasting longer than 3 months, with other symptoms including malaise, headaches, muscle and joint pain, sleep disturbances and concentration difficulties.1–3 Anxiety and depression are also common among patients with CFS/ME.4 The prevalence of paediatric CFS/ME is between 0.1% and 2%.5–8 The UK National Institute for Health and Care Excellence (NICE) recommends patients with CFS/ME manage their condition by improving sleep quality, limiting rest periods, introducing ‘low level’ physical and cognitive activities and eating a well-balanced diet.2 Patients with mild-to-moderate CFS/ME should also be offered cognitive behavioural therapy, graded exercise therapy or activity management.2
CFS/ME symptoms can be triggered by vigorous exercise,9–11 or a sudden increase in physical activity.12 13 However, little is known about the relationship between objectively measured physical activity and the symptoms of CFS/ME. The majority of studies that have examined physical activity among patients with CFS/ME have focused on adult populations.9–19 Adult patients with CFS/ME are considered to be less physically active compared with population data16 18 19 and physically inactive adults report greater fatigue.14 15 However, the majority of studies used self-reported questionnaires to assess physical activity levels, which have low reliability and correlation with objective physical activity measurements (eg, accelerometry) in patient and healthy populations.16 20 21 Patterns of physical activity among adult patients with CFS/ME have been classified into two subgroups, namely ‘fluctuating active’ and ‘passive’, with proportions of 75% versus 25%, respectively.17 ‘Fluctuating active’ or ‘boom-bust’ patients generally show infrequent bursts of activity followed by extreme exhaustion, whereas ‘passive’ patients tend not to take part in activities.17
Less is known about physical activity levels and patterns in paediatric CFS/ME. One study investigated exercise capacity in children and adolescents with CFS/ME (N=20, mean age 14.9±3.7 years), finding that maximal exercise capacity was only reduced in a minority of patients and was related to current physical activity levels.22 Another study investigated the efficacy of cognitive behavioural therapy for adolescent patients with CFS/ME (N=29, mean age 15.6±1.3 years), with treatment protocols adapted to patients’ accelerometer-assessed physical activity patterns (‘passive’ vs ‘active’).23 Passive and active patients showed equal improvements for fatigue, functional impairment and school attendance,23 and rates of improvement were larger than seen in previous studies where one protocol was used to treat all patients.24 These results suggest that adapting treatment to different physical activity patterns may improve treatment outcome.23
Children and adolescents with CFS/ME experience higher rates of mood disorders than healthy populations,25–27 with around 30% of adolescent patients with CFS/ME experiencing anxiety and/or depression.26 27 For most children, anxiety and depression appear to develop because of their condition.28 29 While comorbid mood disorders are associated with increased disability, fatigue and pain, there is no evidence on the relationship between comorbid mood disorders in CFS/ME and objectively measured physical activity.
Little is known about physical activity levels and patterns in paediatric CFS/ME and how physical activity is associated with physical function and other health outcomes. Therefore, this study aimed to: (1) determine physical activity patterns for children and adolescents with mild-to-moderate CFS/ME at treatment commencement and (2) investigate how these activity patterns are cross-sectionally associated with physical function, pain, fatigue, anxiety and depression.
Methods
The current analyses used baseline data from the Managed Activity Graded Exercise iN Teenagers and pre-Adolescents (MAGENTA) study,30 which investigated the effectiveness of graded exercise therapy versus activity management for treating CFS/ME in patients aged 8–17 years. Between September 2016 and September 2018, data were collected from 237 young people with CFS/ME in Bath (N=235) and Newcastle (N=2), UK. Written parent consent and young person consent/assent was received for all participants.
Recruitment
Paediatricians and general practitioners referred young people with probable CFS/ME to specialist services in Bath and Newcastle. The clinician conducting the initial assessment in the CFS/ME specialist service identified eligible children and adolescents (diagnosed with CFS/ME based on NICE guidance2 and aged between 8–17 years). Exclusion criteria included being severely affected by CFS/ME, referred for cognitive behavioural therapy at first clinical assessment and/or unable to attend clinical sessions. NICE defines severe CFS/ME as being unable to do activity for themselves, only carrying out minimal daily tasks, having severe cognitive difficulties and/or depending on a wheelchair for mobility.2
Outcome measures
Data routinely collected at first clinical assessment included age, sex, months of illness, Physical Functioning Scale of the 36-Item Short Form Health Survey (SF36-PFS),31 pain visual analogue scale, Chalder Fatigue scale (CFQ-11),32 Spence Children’s Anxiety Scale (SCAS)33 and Hospital Anxiety Depression Scale (HADS).34 SF36-PFS comprises 10 items encompassing a hierarchical range of difficulties,31 with items scored (1–3) based on perceived limitations and higher scores indicating greater physical function. Young people were asked to indicate pain severity along a continuous line from ‘no pain’ to ‘pain as bad as possible’. CFQ-11 measures the extent and severity of physical and psychological fatigue, with items scored on four-point scales ranging from ‘less than usual’ to ‘much more than usual’ and higher scores indicating greater fatigue.32 SCAS identifies symptoms of anxiety disorders in young people via 44 items measured on four-point scales ranging from ‘never’ to ‘always’, with higher scores indicating greater anxiety.33 HADS is a 14-item scale measured on individual four-point scales assessing agreement with statements related to anxiety and depression (eg, ‘I feel tense/wound up’).34 Due to the sensitive nature of some items, HADS was only collected from participants aged 12 and above.
Accelerometer measures
Participants were asked to wear a waist-worn ActiGraph GT3X+ accelerometer for seven consecutive days. Accelerometer data were processed using Kinesoft (V.3.3.75; Kinesoft, Saskatchewan, Canada) in 60 s epochs and were included if participants provided at least three valid weekdays. A valid day was defined as at least 500 min (from 06:00 to 23:00), after excluding intervals of ≥60 min of zero counts allowing up to 2 min of interruptions. Mean minutes of sedentary, light, moderate-to-vigorous physical activity (MVPA) and vigorous-intensity physical activity were established using age-appropriate cut-points.35
Statistical analysis
Descriptive statistics (means, SDs, t-tests, Wilcoxon) were used to describe the sample regarding their physical activity by age and gender. The t-tests were used to examine the differences between boys and girls, while Wilcoxon rank-sum tests were used to examine the differences between two age categories (8–11 years, 12–17 years), due to the small number of children aged 8–11 years. All analyses were performed using STATA V.15. Latent profile analysis estimates the number of latent homogeneous classes in a heterogeneous sample based on the pattern of responses on two or more observed continuous variables. Three to seven adherent days from the participant’s accelerometry was used to determine classes of participants who tended to accumulate their physical activity or sedentary behaviour in a similar daily pattern. Underlying classes were determined based on participants who shared similar means for the following weighted indicators: proportion of sedentary behaviour from total wear time per weekday/weekend day, MVPA as a proportion of non-sedentary time per weekday/weekend day.
To select the appropriate number of classes and maximise model fit, a series of latent class models (2–6 class models) were fit to the data. Beyond this, the sample sizes of extreme cases were likely to be too small. To detect model identification problems, 100 iterations of each model were run using randomly generated seed values. Statistical fit indices (Bayesian Information Criterion (BIC),36 Akaike Information Criterion (AIC)37) and conceptual considerations were used to determine the number of classes that adequately described the sample. Lower BIC and AIC values were preferred. Additionally, theoretical implications and distinctiveness of each latent class profile (entropy) were examined, with the aim of having high correspondence between established classes and some practical interpretation of what the classes indicated.
Linear regression models were used to examine whether physical activity (using the emergent latent classes) was associated with physical function as the primary analysis. Secondary analyses examined whether physical activity additionally was associated with pain, fatigue, anxiety and depression. Models were adjusted for age (years), gender and time since diagnosis (months). We adjusted for time since diagnosis because we hypothesised that children who had been ill for longer would be less fit and engage in lower levels of physical activity.
Sensitivity analyses were conducted with participants who provided one or 2 days (weekday or weekend) of valid accelerometer data, with models rerun and results qualitatively compared.
Public and patient involvement
A Patient Advisory Group (PAG) was involved throughout the development of the protocol and has remained involved throughout the running of the trial, with PAG meetings being held every 6 months. Minutes from the PAG group will be disseminated to the Study Steering Committee and the Trial Management Group. The PAG will be consulted for the public dissemination of any product arriving from this research.
Results
The figure 1 presents the study flow of participants. The final sample included 138 participants, of those 16.7% were 8–11 years and 83.3% were 12–17 years, while 27.5% were boys and 72.5% were girls. Median time since diagnosis was 14 months (IQR 10–24). Physical activity descriptive statistics are presented in table 1. Younger children (8–11 years) were less sedentary and engaged in more physical activity than adolescents. Three participants (2.2%) achieved the UK Government’s physical activity recommendations of at least 60 min per day,38 on all valid days. Thirteen participants (9.4%) achieved an average of 60 min of MVPA per day across the week.

Flow chart of participant accelerometer data.
Descriptive statistics of the physical activity variables
To compare physical activity levels of young people with CFS/ME from the present study with children from healthy populations, we descriptively examined physical activity variables from other UK studies that used the same accelerometer cut points.39 40 The Millennium Cohort Study was a nationally representative prospective cohort study with 6497 children aged 7–8 years.39 B-Proact1v was a longitudinal study with 1223 children aged 8–9 years from south-west England.40 The table 2 shows the sedentary time, MVPA (median, IQR) and proportion meeting the recommendations (%, SE). Young people with CFS/ME in the present study were more sedentary, less active and less likely to meet the recommendations than their healthy counterparts (9.4% vs, 50.8% Millennium Cohort and 46.4% B-Proact1v).
Comparison between data of patients with chronic fatigue syndrome or myalgic encephalomyelitis and daily physical activity data from healthy populations
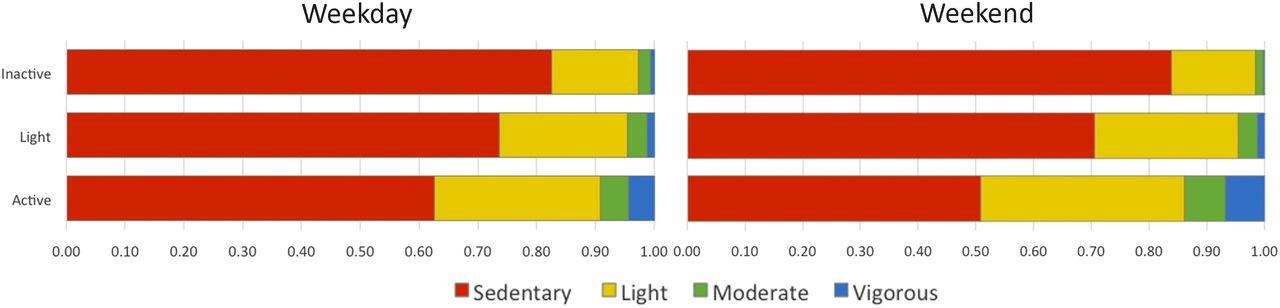
Model fit indices (online supplementary table S1), as well as ease of class interpretability and conceptual meaning, suggested that the three-class latent class model was the most appropriate for the data. The three latent classes were classified as: ‘active’, ‘light’ and ‘inactive’. The table 3 presents the latent class prevalence and proportion of time spent in each activity category. The figure 2 graphically displays the proportion of time spent in each activity level on weekdays and weekend days for each latent class. The mean number of minutes per day of MVPA and sedentary time were ‘active’ 71.63 and 416.28 min, ‘light’ 34.34 and 546.96 min and ‘inactive’ 17.14 and 588.67 min. The expected proportions of the population in each class were 9.0% ‘active’, 43.1% ‘light’ and 47.9% ‘inactive’.
Supplemental material
Latent class prevalence and proportion of total time spent in each activity

{kind=link}
{kind=link}
Proportion of time spent in activity on weekdays and weekend days.
The table 4 presents the associations between the emergent physical activity latent classes and young people’s self-reported physical function (SF36-PFS). Compared with being ‘inactive’, there was evidence that being categorised as ‘light’ or ‘active’ was associated with a 10.35 (95% CI 2.32 to 18.38) and 15.26 (95% CI 0.12 to 30.40) greater physical function score, respectively.
Mean difference in the children’s physical function score associated with physical activity latent classes (N=137)*
Online supplementary tables S2-S5 show the associations between the physical activity latent classes and young people’s self-reported pain, fatigue, anxiety and depression, respectively. Compared with being ‘inactive’, there was some evidence that being categorised as ‘light’ was associated with reduced fatigue, whereby young people in this group reported lower levels of fatigue (partially adjusted mean difference: −1.60, 95% CI −3.13 to −0.06). There was also evidence that being in the ‘active’ class was associated with anxiety, whereby ‘active’ young people reported a 13.79 (95% CI 1.73 to 25.85) greater anxiety score compared with the ‘inactive’ class. There was no evidence for associations between the latent classes and pain or depression scores.
Sensitivity analysis
When analyses were rerun including participants who provided 1–2 days of valid accelerometer data (N=22), a four-class model was selected based on the previous criteria. The classes were defined as ‘active’, ‘light’, ‘inactive’ and ‘very inactive’. Online supplementary table S6 shows the latent class prevalence and proportion of total time spent in each activity for the sensitivity analysis. Online supplementary table S7 presents the associations between the emergent latent classes in the sensitivity analysis and physical function score. Compared with the ‘very inactive’ class, there was evidence that being in the ‘light’ class was associated with a 17.36 (95% CI 0.23 to 34.48) greater physical function score. Online supplementary tables S8-S11 demonstrate no evidence for associations between the physical activity latent classes and young people’s pain, fatigue, anxiety and depression, respectively.
Discussion
This is the first study to link patterns of physical activity and sedentary behaviour among young people with mild-to-moderate CFS/ME with differences in fatigue, pain, disability, anxiety and depression between the emergent latent classes. The three-class model represented meaningful classes that provided more detail than unidimensional measures alone, such as whether children meet physical activity recommendations, which may not be appropriate for CFS/ME patients.
Compared with a nationally representative sample of younger children aged 7–8 years,39 paediatric patients with CFS/ME were sedentary for an additional 2.7 hours per day and participated in less than half the amount of MVPA. However, it is difficult to make comparisons, as a multination longitudinal study of children and adolescents (aged 2–18 years) from the general population, demonstrated that from the age of 5 years there is an average cross-sectional decrease of 4.2% in physical activity with each additional year.41 This is consistent with the findings from the present study, whereby younger children aged 8–11 years were more active and less sedentary than adolescents. Mean daily MVPA was less than half the government’s recommendations for physical activity.38 Among the general population, boys are less sedentary and more active than girls at all ages.41 However, in this study, there was no meaningful difference in physical activity between genders, most likely due to lower physical activity levels across the sample.
The ‘active’ class was the smallest of the three classes (8.7%), compared with much higher proportions in the ‘light’ (44.2%) and ‘inactive’ (47.1%) classes. Children in the ‘active’ class performed a mean 71.6 min of MVPA per day compared with just 17.1 min per day among the ‘inactive’ class, who were also sedentary for an additional 3 hours. These results highlight the diversity of physical activity behaviour among young people with CFS/ME, suggesting treatment protocols should be adapted based on physical activity assessment. In a study by Stulemeijer and colleagues,23 ‘active’ patients were encouraged to reduce their activity, recognise their limitations and accept their condition before building up activity levels, while ‘passive’ patients were encouraged to address and challenge beliefs that activity would aggravate symptoms and build up activity as soon as possible. Despite receiving different treatments, both groups reported decreases in fatigue severity and improvements in school attendance,23 and improvement rates were greater than studies where only a single protocol was used.24 Previous studies with adult patients with CFS/ME identified a ‘fluctuating active’ or ‘boom-bust’ physical activity pattern17; however, this pattern did not emerge from the present analyses, most likely due to the relatively small sample size and missing days of accelerometer data.
Compared with the ‘inactive’ class, being in the ‘light’ or ‘active’ class was associated with improved physical function by 10.4 and 15.3 points, respectively, which is greater than the minimal clinically importance difference for the SF36-PFS.23 42 43 There was some evidence to suggest that being in the ‘light’ class was associated with lower levels of fatigue compared with being in the ‘inactive’ class, but adjusting for time since diagnosis attenuated this association. It is possible that engaging in ‘light’ physical activity provides some protection against fatigue, but it is also possible that the ‘inactive’ group engaged in less activity because they were more unwell. This would mean that high levels of physical activity could be a marker for less severe disease. The present study found that in comparison to the ‘inactive’ class, being classified as ‘active’ was not associated with fatigue, which is different to findings in adult patients with CFS/ME.15 16 The discrepancy in findings with the present study may be due to the differences in physical activity measurement (self-report vs objective) or population (adult vs child) or the very small sample size in the ‘active’ class. Being ‘active’ was associated with greater anxiety compared with being in the ‘inactive’ class. It may be that young people are anxious because they are physically active or that anxiety is driving them to be active. However, the cross-sectional nature of the study and the very small sample size of the ‘active’ class limit any inferences that can be made. No associations were present between the physical activity latent classes and children’s pain and depression scores.
Strengths and limitations
The major strength of this study is the use of latent profile analysis to identify patterns of accelerometer-assessed physical activity in young people with CFS/ME. While cross-sectional analyses are typically viewed as a limitation in observational research, in latent profile analysis, the latent variable is assumed to be static or unchanging, making the use of cross-sectional data appropriate. Limitations include the relatively small sample size, few participants being classified as ‘active’ and missing days of accelerometer data that limited the ability to detect other physical activity patterns in the data. The SF36-PFS has been shown to be reliable and valid for a range of populations, including older adolescents (aged 14+ years), teenagers with CFS/ME, adults, psychiatric patients, patients with minor conditions and chronic diseases44 45; however, it has not yet been validated with children or younger adolescents. The sample was cross-sectional limiting our ability to hypothesise about the direction of causality. Additionally, the sample was drawn from one region in south-west England and limited to patients with mild-to-moderate CFS/ME, thus patients with severe CFS/ME were excluded. As such, our ability to extend findings to other populations is limited.
Conclusions
This study examined physical activity patterns of young people with mild-to-moderate CFS/ME. Although some patients with CFS/ME are meeting physical activity guidelines, the majority are doing less than half the recommended amount. Compared with being ‘inactive’, there was some evidence to suggest being classified as ‘active’ was associated with greater physical function but also greater anxiety, while being ‘lightly’ active was associated with greater physical function and lower levels of fatigue. Paediatricians need to recognise that physical activity varies between patients with mild-to-moderate CFS/ME when they recommend treatment. Future research is needed to investigate the relationship between physical activity patterns and treatment outcome.
References
Footnotes
Contributors ES-M analysed and interpreted the data, drafted the initial manuscript and reviewed and revised the manuscript. RJ designed the physical activity measurement component of the study, supervised data analysis and critically reviewed the manuscript for important intellectual content. LB and AB designed the data collection instruments, collected data and reviewed and revised the manuscript. EC conceptualised and designed the study, supervised data collection and critically reviewed the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding This work was supported by the National Institute for Health Research (Senior Research Fellowship, SRF-2013-06-013).
Disclaimer The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health.
Competing interests All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: EC has received a Senior Research Fellowship from the National Institute for Health Research; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Patient consent for publication Not required.
Ethics approval Ethical approval was received from the NHS research ethics committee (Ref: 15/SW/0124).
Provenance and peer review Not commissioned; externally peer reviewed.