Article Text

Abstract
Introduction Anticipated or actual pain in neonates results in use of paracetamol for prolonged pain relief in many neonatal intensive care units. Clinical trials examining safety of paracetamol exposure in neonates have been of short duration (1–3 days) and hepatic biomarkers and paracetamol metabolism are rarely reported in the same studies.
We aim to investigate the safety (hepatic tolerance) and effectiveness of prolonged paracetamol exposure in neonates by measuring hepatic biomarkers, plasma concentrations of paracetamol and its metabolites and pain scores. In addition, we study a possible interaction between ethanol and paracetamol.
Methods and analysis A multicentre interventional cohort study.
Neonates of any gestational age and up to 44 weeks postmenstrual age, treated with oral or intravenous paracetamol can be included.
Alanine aminotransferase (ALT) and bilirubin are measured at baseline or within 24 hours after treatment initiation. P-paracetamol and metabolites are measured at steady state and every 2 days (opportunistically) together with ALT and bilirubin and lastly after discontinuation of treatment. COMFORT neo pain scores are collected longitudinally. COMFORT neo pain scores and population pharmacokinetic analysis of paracetamol samples will be analysed simultaneously using non-linear mixed effects models. One and two compartment models with first-order elimination will be tested for disposition. In addition, plasma ethanol is measured if the patient receives concomitant treatment with intravenous or oral phenobarbital containing ethanol as an excipient.
Ethics and dissemination Inclusion of patients can be postponed 24 hours after the first paracetamol dose. This is intended to make the inclusion process less stressful for parents. This study uses standard dosing strategies. The potential risks are additional blood samples, which are collected opportunistically to reduce additional heel pricks.
Trial registrationnumber Ethics Comittee: H-17027244, EudraCT no: 2017-002724-25, BFH-2017–106, 05952.
- analgesia
- neonatology
- pharmacology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
In neonatal pain paracetamol is increasingly prescribed to reduce opioid use, and it has been shown to have opioid-sparing effect.
Prospective data suggest a good tolerability and no major adverse events including the absence of drug-induced hepatic toxicity when administered for 3 days or less.
A few cases have described paracetamol overdosing in neonates showing variable increase in hepatic biomarkers. All were treated with N-acetylcysteine and recovered without sequelae.
What this study hopes to add?
Safety and pharmacokinetic information on prolonged use (>72 hours) of paracetamol in term and preterm neonates.
Potential changes in hepatic biomarkers (bilirubin, alanine aminotransferase and coagulation factors II, VII and X) after prolonged (>72 hours) paracetamol administration in neonates.
Data regarding plasma paracetamol concentrations and analgesic effect.
Introduction
Adequate pain management in neonates is a major issue in neonatal care. Anticipated or actual pain in neonates results in extended use of pain medications, and paracetamol is used for pain relief in almost every neonatal intensive care unit (NICU).1 Clinical trials examining safety of paracetamol exposure in neonates are primarily of short duration (1–3 days) and hepatic biomarkers and paracetamol metabolism are seldom reported in the same studies.2–4 Since paracetamol is widely used as prolonged treatment in neonates and has a clinical significant opioid-sparing effect,5 it is highly relevant to investigate safety of prolonged intravenous or oral paracetamol. With emphasis on increased risk of hepatic toxicity, for example, by induction of the CYP450 oxidative system due to long-term exposure of paracetamol. This mechanism may be superimposed by combination with ethanol-containing drugs, which are metabolised by the same pathways. The PARASHUTE study: intravenous and oral paracetamol in neonates: safety and ethanol-drug interaction aims to improve the knowledge on safe and effective paracetamol treatment strategies in neonates.
Paracetamol metabolism
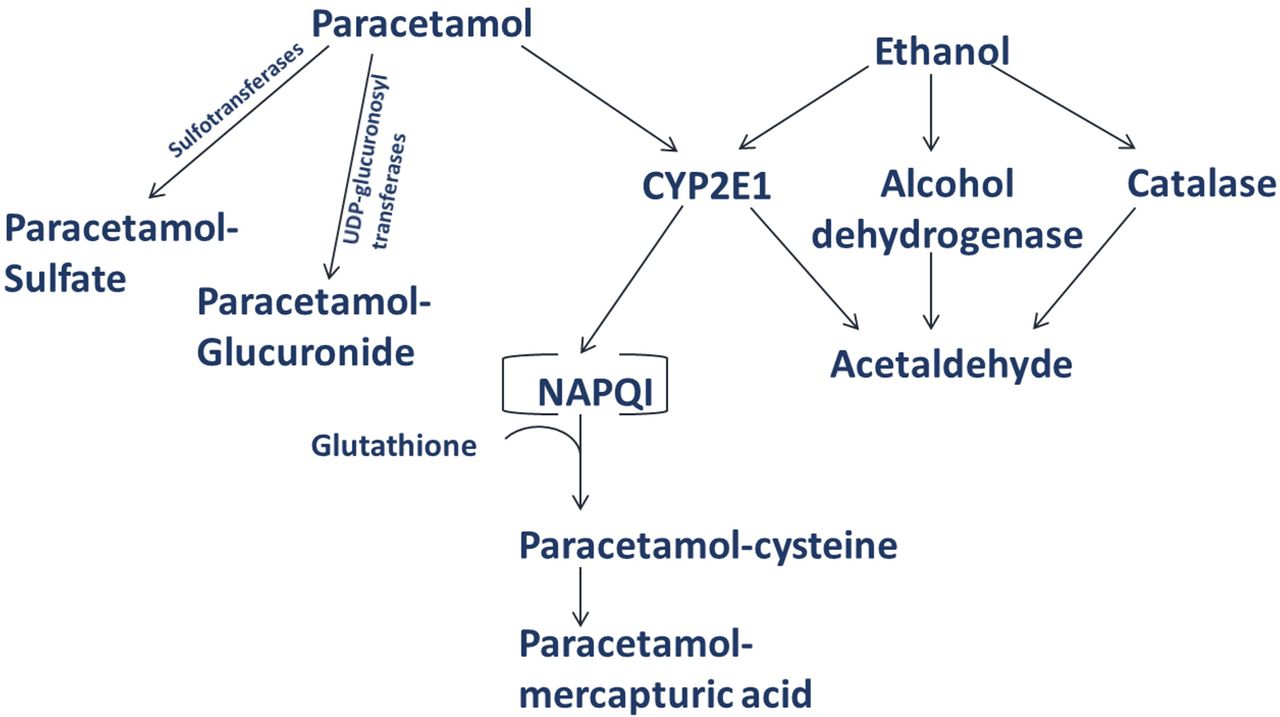
Paracetamol (N-acetyl-p-aminophenol or acetaminophen) is used for its antipyretic and weak analgesic effect. In children, paracetamol is metabolised mainly in the liver through three metabolic pathways: glucuronidation, sulfation and oxidation (figure 1). The contribution of each metabolic pathway differs by age. Sulfation is considered the major pathway in young children6–8 and shows no sign of saturation after up to 20 mg/kg intravenous paracetamol neonates<32 weeks gestational age.9 The glucuronidation pathway reaches adult levels around 12 years of age.7 One trial found no evidence of glucuronidation upregulation after up to 12 repeated paracetamol doses in neonates and infants,8 which previously was the understanding in both adults and children.8 The oxidation pathway accounts for <10% in adults10 11 and occurs primarily via cytochrome P450 2E1 enzyme (CYP2E1). The product of oxidation is N-acetyl-p-benzoquinone imine (NAPQI), which is excreted in urine as conjugates with mercapturic acid and cysteine. These metabolites may provide an indirect estimate of NAPQI formation.12 CYP2E1 activity is lower in neonates and increases gradually during the first 90 days of life.13 Hepatic micro samples have shown less CYP2E1 protein in samples from neonates compared with infants, children and young adults.14 All metabolites are excreted in urine and have no analgesic effect.12 Less than 4% is excreted unchanged in the urine in all ages.7 10 15 Overall clearance is reduced in neonates, that is, very preterm: 0.090 L/hour/kg, preterm 0.116 L/hour/kg and term infants 0.170 L/hour/kg4 and reaches 90% of adult values at 1 year of age.

Paracetamol and ethanol metabolism. The figure illustrates the hepatic metabolism of paracetamol through three different pathways: sulfation, glucuronidation and oxidation (cytochrome P450 2E1 [CYP2E1]). In addition, the metabolism of ethanol through CYP2E1 is shown.
Safety and repeated dosages
Repeated doses of paracetamol administered to neonates could shift the metabolism towards oxidation via CYP2E1 and formation of NAPQI. In adults the sulfation pathway is saturable and eventually the glucuronidation pathway at supratherapeutic doses.16 17 The risk of hepatotoxicity associated with paracetamol is caused by NAPQI (figure 1). Conjugation with glutathione renders NAPQI non-toxic. If glutathione becomes depleted by 70% or more, NAPQI formation rises, leading to mitochondrial dysfunction, cell death and necrosis.18 As suggested from case reports of paracetamol overdosing,19 neonates are capable of forming NAPQI but appear to have a lower incidence of hepatic failure than adults.20 This may be explained by relative immaturity of the CYP450 oxidation system and a larger sulfation capacity.14 In addition, a relatively larger liver volume per kilogram found in children may contribute to the low incidence.21
Three studies examined repeated intravenous paracetamol administration in neonates for: 31 hours, 48 hours and 4 days (range 1–9 days).2–4 Two of the studies measured paracetamol, paracetamol metabolites and hepatic biomarkers (bilirubin, alanine aminotransferase [ALT], aspartate aminotransferase [AST])2 4 and one trial measured paracetamol concentration and hepatic biomarkers (bilirubin, ALT, gamma-glutamyl transferase (GGT), alkaline phosphatase and albumin).3 Notably, paracetamol was administered repeatedly for several days despite a threefold increase in ALT in one patient and moderate increase in three patients.3 For all patients the authors proposed that other causes could explain the elevated enzymes, for example, total parental nutrition.3 Few studies examined multiple oral doses of paracetamol in neonates.1 Anderson et al randomised 30 neonates (gestational age at birth 31–40 weeks) and infants to receive either paracetamol suppositories or oral solution administered over 2 days and measured only pharmacokinetic parameters.22
A review from 2018 found 19 ongoing studies examining paracetamol for persistent ductus arteriosus, with a variable focus on safety with few studies reporting hepatic biomarkers as secondary outcome and none measures paracetamol metabolites.23
In one trial, a NICU database and pharmacy register were used to examine hepatic biomarkers in 189 neonates who had received repeated doses of paracetamol for a median of 60 hours (range 6–480 hours); no significant increase in ALT, AST or GGT was found.24
At least five cases of paracetamol overdoses in preterm neonates have been published. Doses ranged from 136 to 446 mg/kg/dose. N-acetylcysteine was administered for up to 7 days. Increased international normalised ratio and bilirubin were seen in some cases but no other signs of hepatotoxicity were identified and no long-term consequences were detected.19
Analgesic effect of paracetamol and pain scores
According to a number of studies and systematic reviews, the way of administration, as well as, loading and maintenance dose influence the target blood concentration and hence the analgesic effect of paracetamol.1 2 25 Existing evidence from one clinical trial and one newer dosing guideline supports a mean steady state target paracetamol concentration of 9–11 mg/L to achieve analgesic effect in neonates born between 26 and 41 gestational weeks.25–27 This is based on pain scores (Leuven Neonatal Pain Score) correlated with plasma paracetamol in 19 neonates receiving intravenous paracetamol as single analgesic. However, only few data exist and treatment recommendations varies between countries.26 Furthermore, two studies have shown significant morphine-sparing effect of paracetamol.5 28
Numerous pain scores are used throughout NICUs internationally. All Danish NICUs use the COMFORT neo pain score for evaluation of pain in neonates. The COMFORT neo pain score has been used for preterm and term neonates for prolonged and acute pain.29–31
Ethanol-paracetamol interaction
A number of excipients can interact with drug metabolism and neonates might be more susceptible to this type of interaction.32 Ethanol (alcohol) is an excipient used in many intravenous and oral formulations, for example, phenobarbital, to increase solubility or act as a preservative. The pharmacokinetics and safety of ethanol in neonates are poorly described.32 In one trial, ethanol and the metabolite acetaldehyde were measured in 49 preterm infants receiving iron and furosemide compared with a control group. They found that blood ethanol in the exposed group was low, but the acetaldehyde level was consistent with moderate alcohol exposure.33 Both paracetamol and ethanol is metabolised by CYP2E1 and the two substrates may compete for the limited capacity of the enzyme.17 Alcohol may modify CYP2E1 activity and deplete glutathione stores in adults.34 Additionally, phenobarbital inhibit glucuronidation and potentiate oxidation in vitro while human studies suggest a protective role in paracetamol-induced hepatotoxicity with no clear mechanism described.17
Objectives
We aim to explore if prolonged (>72 hours) treatment with intravenous or oral paracetamol administered to neonates is associated with hepatotoxicity assessed by hepatic biomarkers (ALT, bilirubin and coagulation factor II, VII and X), paracetamol metabolites and paracetamol concentration (table 1).
Objectives and outcomes measures in the PARASHUTE study
Secondary aims are: first, to collect COMFORT neo pain scores and associate these with paracetamol concentrations. Second, to examine if ethanol-containing drugs (intravenous/oral phenobarbital) are associated with higher plasma ethanol and if the presence of ethanol may interact with paracetamol (table 1).
Methods and analysis
Design and population
The study is a multicentre interventional cohort study.
Neonates with any gestational age at birth and up to 44 weeks postmenstrual age admitted to the two largest NICUs in Denmark, Rigshospitalet, Copenhagen University Hospital and Aarhus University Hospital, are eligible for enrolment. The neonatal patients can be included when they are expected to receive paracetamol (oral or intravenous) for >72 hours.
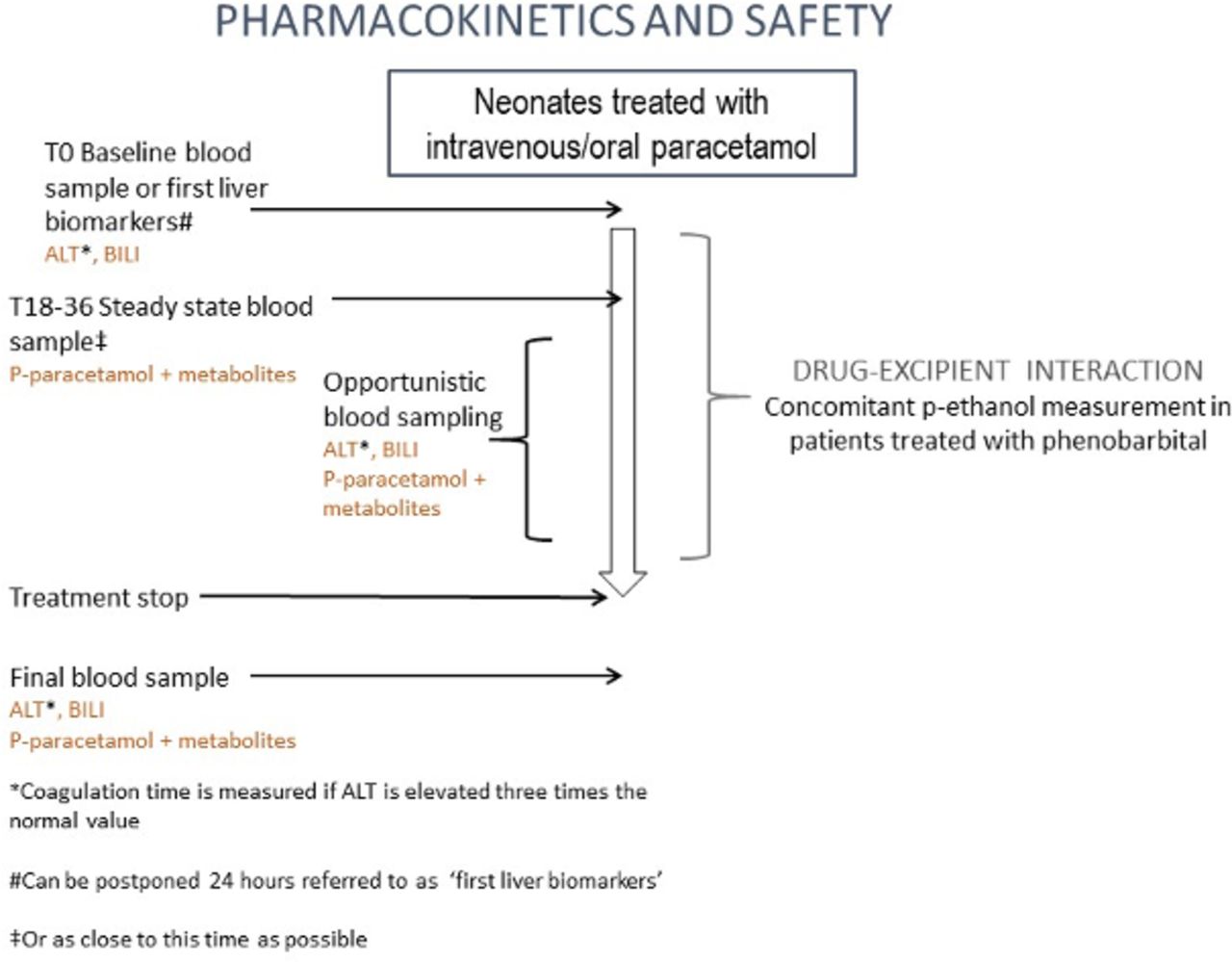
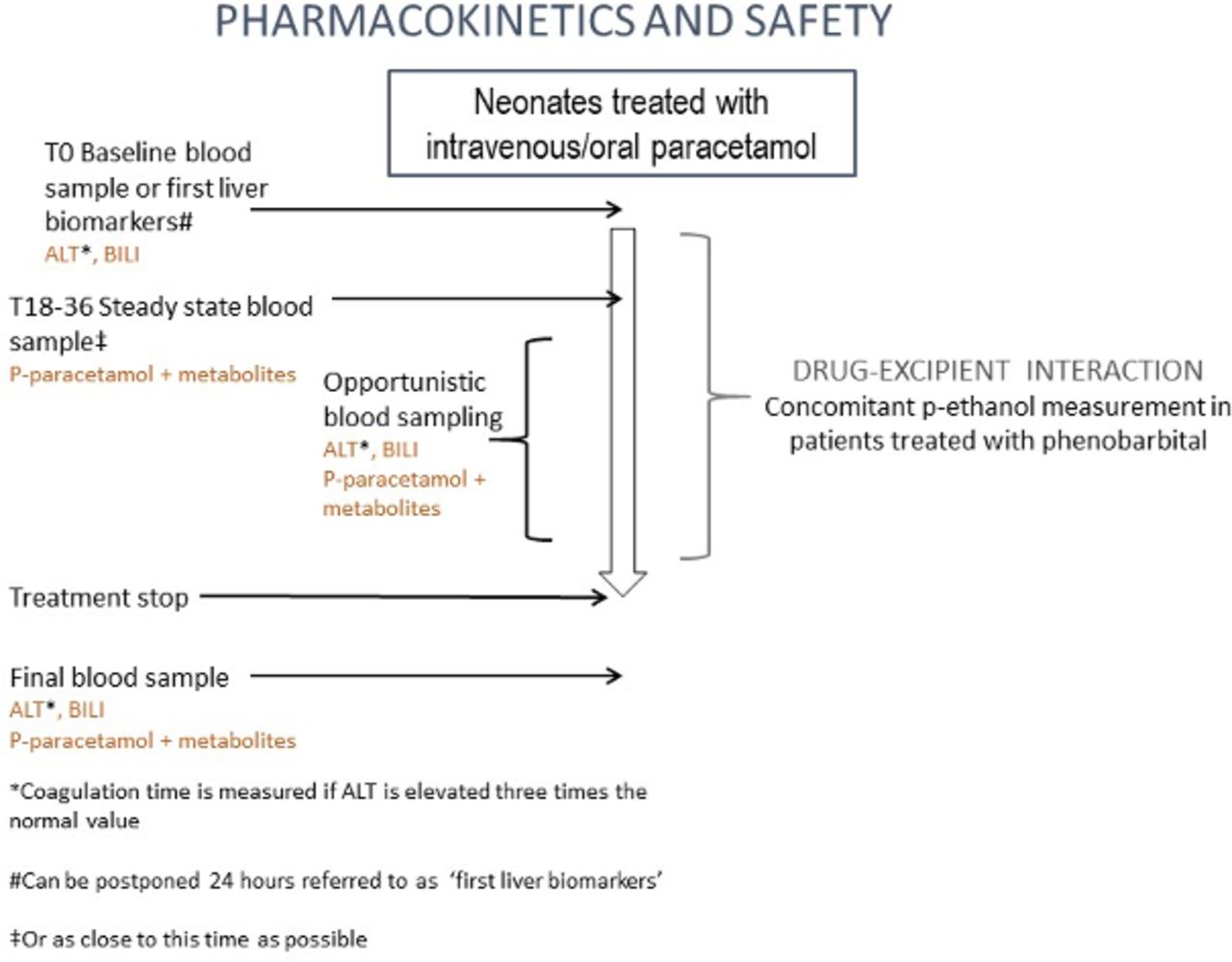
A recent audit of medical records from the NICU at Rigshospitalet revealed that approximately 10% of the patients received intravenous paracetamol and 5% oral paracetamol for >3 days (unpublished data, see online supplementary table S1). Hence, the patient is treated at the clinician’s discretion and the therapeutic strategy is not decided by a protocol. The duration of treatment and dose and administration (intravenous or oral) of paracetamol will follow the prescription by the attending physicians in the NICU (oral paracetamol was included in Amendment A approved March 2018). Only standard medicines are used. Eligible patients can be enrolled before or after administration of paracetamol according to eligibility criteria (tables 2 and 3). Inclusion and measurement of ALT and bilirubin may be postponed for 24 hours (figure 2 and table 3). The subsequent blood sample for measuring paracetamol or its metabolites is drawn 18–36 hours or in close proximity after consecutive administrations of paracetamol. This time interval is chosen as steady state is expected to occur approximately 18–36 hours after administration of the drug with or without loading dose, shown by Allegaert et al.35 The blood sample will be repeated 0–24 hours after treatment discontinuation. After the first sample, plasma paracetamol, metabolites, ALT and bilirubin will be measured opportunistically36 every second day. After 6 days of consecutive paracetamol treatment samples are taken every third day to reduce the number of samples and to ensure feasibility of blood sampling during long treatment periods. Coagulation factors will be measured in addition if ALT increases to more than three times the upper normal value, this is standard in the NICUs involved. ALT, bilirubin and coagulation factors measured after treatment discontinuation will be collected until normalisation. Discontinuation of treatment and potential follow-up are done at the discretions of the responsible clinician. All paracetamol doses are collected, other medicines are permitted and registered together with diagnosis, weight, length, head circumference, Apgar score and birth method. This study does not include data on perinatal exposure of paracetamol since paracetamol is an over-the-counter drug in Denmark and is used frequently. The nature of the study will therefore not reliably be able to backtrack during which part of the perinatal period the neonate has been exposed and to which extend. All COMFORT neo scores are collected during paracetamol treatment and all nurses are certified with a kappa value >0.65.
Supplemental material
{kind=link}
{kind=link}
Study design. ALT, alanine aminotransferase; BILI, bilirubin.
Inclusion and exclusion criteria for the PARASHUTE study
Time schedule for participants in the PARASHUTE study
Patient involvement
Patients were not directly involved in the design of this study.
Analysis
Samples will be analysed by high-performance liquid chromatography-electrospray ionisation-tandem mass spectrometry (HPLC-ESI-MS/MS) for simultaneous quantification of acetaminophen, acetaminophen-glucuronide, acetaminophen-sulfate, acetaminophen-glutathione, acetaminophen-cysteine and acetaminophen-N-acetylcysteine in small volumes of human plasma and urine.37 Acetaminophen-d4 and acetaminophen-d3-sulfate are used as internal standards (IS). Analytes and IS are recovered from human plasma or serum (10 μL) by protein precipitation with acetonitrile. Calibration concentration ranges are tailored to literature values for each analyte for the biological matrix. Prepared plasma samples are analysed on an Agilent 1260 Infinity HPLC system (inline solvent micro-degasser, binary LC pump, high-performance thermostatted autosampler and 1290 Infinity thermostatted column compartment) interfaced with an Agilent 6460 triple-quadrupole mass spectrometer (Agilent Technologies, Santa Clara, California, USA). MassHunter Workstation software (Agilent Technologies) is used for instrument control, data acquisition and ESI-MS/MS parameter optimisation and data analysis. Chromatographic separation is achieved through use of an Agilent Poroshell 120 EC-C18 column with a 20 min run time per injected sample. The analytes can be accurately and precisely quantified with multiple reaction monitoring over 2.0–3.5 orders of magnitude. Mean intra-assay and inter-assay accuracies range from 85% to 112%, and intra-assay and inter-assay imprecision do not exceed 15% for any analyte.
Sample size
Because of limited knowledge about paracetamol metabolites in neonates and since the correlation between these metabolites and threshold for hepatotoxicity is unknown, sample size calculation is impossible, that is, this is an explorative and hypothesis generating study.
Previous studies,2–4 investigating intravenous paracetamol administrations up to 3 days, included 15, 35 and 50 patients, respectively. It was therefore decided to include a minimum of 60 patients and a maximum of 120 patients. The study is stopped when 120 patients who receive paracetamol for >3 days are included or on 30 April 2019.
Data
Data will be managed by an electronic data capture tool (REDCap) hosted at the Capital Region of Denmark. REDCap is a secure, web-based application designed to support data capturing for research.38 REDCap provides an intuitive interface for validated data entry; second, trails for tracking data manipulation and export procedures, and automated export procedures for seamless data downloads to common statistical packages and ultimately, procedures for importing data from external sources. For analyses the data will be exported to SAS and the software R V.3.5.1 to create a comma-separated input data file that is readable for software for non-linear mixed effect modelling, NONMEM.
Pharmacokinetic and pharmacodynamics modelling
Structural and stochastic model development
During the data compilation, the paracetamol plasma concentrations will be logarithmically transformed prior to modelling, and concentration-time data will be fitted to both one and two compartment models with first-order elimination for the disposition. Different models to characterise the absorption will be tested for the oral-administrated paracetamol. Interindividual variability and interoccasion variability will be tested in relationship to the pharmacokinetic parameters. Both exponential, proportional and combined residual error models will be tested.
Covariate model
Once the base model (structural and stochastic model combined) have been identified, the influence of the different covariates (eg, weight, length, body mass index) will be tested on the pharmacokinetic parameters, possible correlation will be identified through visual inspection. If possible, relevant covariates will be tested on relevant parameters, as judged by visual inspection, in stepwise forward and backward deletion using the stepwise covariate model tool (PsN).
Simulation
COMFORT neo pain scores and population pharmacokinetic analysis of paracetamol samples will be analysed simultaneously. An E max model with lag time will be tested for pain. The pharmacodynamics relationship with the paracetamol concentration and COMFORT neo scores will only be assessed in the periods where the patients receive paracetamol as the only analgesic. However, the longitudinally COMFORT neo scores might hold important data on the pain history over time.
Model evaluation
Selection criteria for final model will be evaluated using prediction-corrected visual predictive checks and bootstrap analysis, a statistic significant level of p<0.05 improvement of fit will be used.
Ethics and dissemination
As this study follows normal dosing strategies, the potential risks relate to the additional blood samples (0.2 mL for paracetamol and metabolites and 0.4 mL for ALT and bilirubin). Blood samples from heel pricks are considered low risk39 when performed by experienced staff. Blood samples will be drawn from indwelling catheters whenever possible to minimise pain or taken by heel prick by experienced NICU staff. Blood loss will not exceed 3% of total blood volume (which corresponds to 2.4–2.7 mL/kg) over a 4-week period or 1% of total blood volume at any single blood draw.40 The loss will be monitored closely. Clinical samples will be given priority over study-specific samples. The samples are stored until they can be shipped for analyses at the Center for Human Toxicology, University of Utah.
Informed consent will be signed by both parents or legal guardian(s). To reduce parental stress following the process of consent and to provide more time for information, inclusion can be postponed 24 hours from the first dose of paracetamol has been administered. ALT and bilirubin should preferably be measured before first administration of paracetamol. However, it is accepted that they are obtained within 24 hours from first administration (inclusion after treatment start and delay of hepatic biomarkers was included in Amendment B approved August 2018).
Normal procedures apply for reporting adverse events and adverse reactions to the Danish Medicines Agency. In relation to the study, only unknown or serious adverse events, and reactions and unexpected serious adverse reactions will be reported to the Danish Medicines Agency and the Ethics Committee.
Perspectives
At present, few hepatic safety data exist on prolonged paracetamol treatment. All results from the current study will be published in peer-reviewed scientific journals regardless of the findings. After publication, the main results will be available at clinicaltrialsregister.eu. Furthermore, the study may generate information used in future national and international guidelines for prolonged treatment of pain in neonates.
This study was approved by the Regional Ethics Committee case no.: H-17027244, the Danish Medicines Agency EudraCT: 2017-002724-25 and the Danish Data Protection Agency: BFH-2017–106, I-Suite no.: 05952.
The two sites were initiated by the Good Clinical Practice (GCP) units at Copenhagen University and Aarhus University in February 2018. The first patient was included in April and June 2018, respectively. The GCP units will monitor the study in accordance with the ICH Harmonised Tripartite Guideline for GCP.
References
Footnotes
Contributors HH, SH, TBH and SSH-K were involved in the conception of the study. HH, SH, TBH, SSH-K, JvdA and KD contributed to the design of the study, the protocol and applied for all permissions. HH, TBH, SH, KD and SSH-K applied for the funding. All authors were involved in preparing the trial sites, acquisition of data, in writing the protocol article and in its revision prior to submission.
Funding This studywas supported by the Danish Regions grant no. 1332.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.