Article Text

Abstract
Background and significance Blast injuries arising from high explosive weaponry is common in conflict areas. While blast injury characteristics are well recognised in the adults, there is a lack of consensus as to whether these characteristics translate to the paediatric population. Understanding blast injury patterns in this cohort is essential for providing appropriate provision of services and care for this vulnerable cohort.
Methods In this mixed-methods review, original papers were screened for data pertaining to paediatric injuries following blasts. Information on demographics, morbidity and mortality, and service requirements were evaluated. The papers were written and published in English from a range of international specialists in the field.
Results Children affected by blast injuries are predominantly male and their injuries arise from explosive remnants of war, particularly unexploded ordinance. Blasts show increased morbidity and mortality in younger children, while older children have injury patterns similar to adults. Head and burn injuries represent a significant cause of mortality in young children, while lower limb morbidity is reduced compared with adults. Children have a disproportionate requirement for both operative and non-operative service resources, and provisions for this burden are essential.
Conclusions Certain characteristics of paediatric injuries arising from blasts are distinct from that of the adult cohort, while the intensive demands on services highlight the importance of understanding the diverse injury patterns in order to optimise future service provisions in caring for this child blast survivor.
- paediatric
- blast
- trauma
- conflict
- outcomes
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Approximately one in six children live in conflict zones, with the main global burden borne by citizens of low and middle income countries (LMICs).1 Children enmeshed in conflict and post-conflict zones are frequently exposed to high-order explosives (HEs), either through explosive remnants of war (ERW) such as landmines and unexploded ordinance (UXO), military ordinance such as shelling and aerial bombardments or acts perpetrated by non-state actors such as improvised explosive devices (IEDs) and suicide bombing.2 HE can inflict unique and unusual injuries on the child through the blast overpressure wave (primary blast injury), energisation of materials causing fragmentation (secondary blast injury), bodily displacement or crush injuries (tertiary blast injuries) and through burns, inhalation, toxic or psychological trauma (quaternary blast injuries).3
The United Nations Convention on the Rights of the Child (UNCRC) seeks to secure both the safety and the well-being of all the world’s children. The long-term consequences of conflict injury constitute grave violations of numerous articles, including Article 3 which calls for signatories to recognise the best interest of the child ‘in all decisions and actions that affect children’. Similarly, Article 6 recognises every child’s right to life and development, and Article 28 seeks to ensure their right to education. Article 23 specifies that children with a disability ‘have the right to live full and decent lives’, and Article 39 states that ‘children…who are victims of war must receive special support to help them recover…’ Blast injury and its immediate effects are covered by Article 3.3, which states that medical care of the child be delivered and supervised by providers competent in that field.4 However, paediatric care in conflict zones is often delivered by personnel for whom experience of dealing with paediatric blast injuries is unusual.5 Primary studies increasingly recognise the complex patterns of injury sustained in the adult population following blast exposure3; however, there is a lack of consensus as to whether applying lessons learnt from the adult population translates appropriately into paediatric cohorts.6 Bree et al 7 argued that principles for life-saving interventions, such as prioritising catastrophic haemorrhage, airway, breathing and circulation, are just as applicable in children as adults. Conversely,Fendya et al 8 contend that directly applying adult trauma principles to the paediatric population neglects the social, anatomical, physiological and psychological differences between adults and children, affecting the validity of these inferences.
While primary studies have described injuries sustained by the blast-injured child, no study has attempted to synthesise the data to identify recurrent characteristics in this vulnerable cohort. Understanding the characteristics of such injuries to the paediatric population will advance efforts to prevent, mitigate and treat these injuries in domestic and deployed health systems.3 The aim of this review is to provide an overview of injury patterns and challenges in caring for the blast-injured child in order to define future research needs for protection, mitigation, immediate medical treatment and rehabilitation.
Methods
In this mixed-methods review, original peer-reviewed quantitative, qualitative and mixed-method observational studies, in addition to grey literature, were screened for data on explosive injuries in paediatric cohorts. By using all study designs, greater capture of relevant literature was achieved, although this meant the data were unsuitable for a formal systematic review. PubMed and Scopus (including Embase) were searched. Search terms including ‘Paediatric’ OR ‘Pediatric’ OR ‘Child*’ OR ‘Children’ AND ‘Blast’ OR ‘Explosi*’ OR ‘Explosion’ were used to capture potential studies. Articles had to be written in English and published before 16 December 2018. Studies involving adult and children were included, in addition to articles where the mechanism of injury was mixed. This decision was taken in order to accurately reflect the settings the studies represent, where victims in conflict zones are heterogeneous and subject to a variety of combat-related mechanisms. Studies were omitted if they did not specify explosive mechanisms or include children.
Children are defined as all humans under the age of 18 years (as specified by the UNCRC).4 The heterogeneity and arbitrary nature of what defines a child is acknowledged, and studies often use individual definitions. Within this review, ages are defined; thus, <1 year are infants, 1–8 are young children, 9–13 are older children and 14–18 are adolescents.
Patient and public involvement
No patients or members of the public were involved in this review.
Results
Study selection of the 74 studies included in this review are shown in figure 1. Of these, 26 used trauma registries (table 1), 26 single-centre hospital-based case series (table 2), 8 used multicentre hospital-based case series (table 3), 13 used community surveillance (table 4) and 1 used grey literature (table 5).
The 26 studies using trauma registries
The 26 studies using single-centre hospital-based case series
The eight studies using multicentre hospital-based case series
The 13 studies using community surveillance
The one study using grey literature
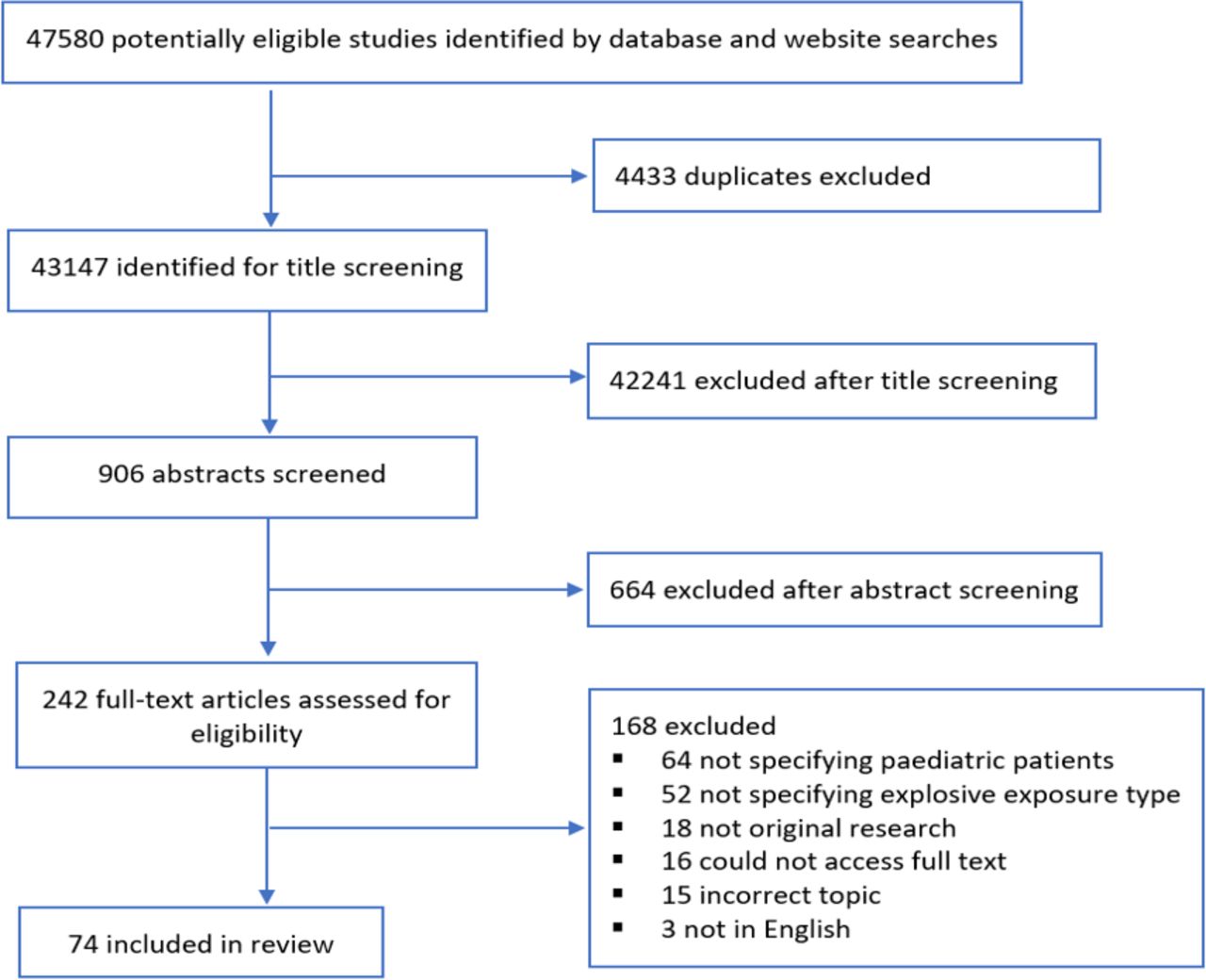
Study selection.
Demographics
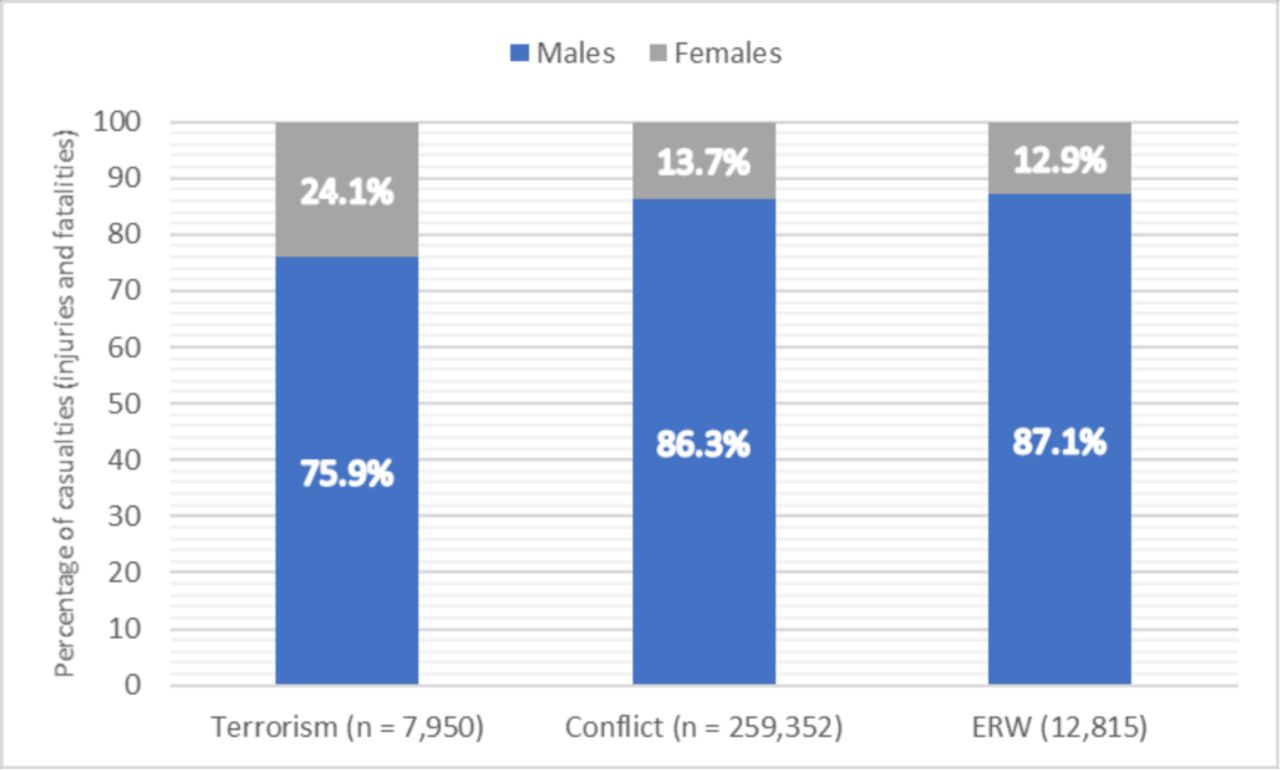
Following the use of explosive weaponry by non-state actors against civilians, the most commonly injured paediatric cohort are males aged 10–18 years old,9–11 while children involved in conflict and ERW blast injuries were generally aged between 4 and 10 years old.12 13 Perpetrators target busy areas such as restaurants and nightclubs which older children and adolescents might frequent,10 11 14 while cultural factors within LMICs in these social areas result in a predominantly male cohort.9 11 14–21 Similar gender findings are observed in children following conflict and ERW-related injuries where all studies showed male predominance in victims, with over 70% male in three quarters of the studies (figure 2).

Gender differences in casualties following blast. ERW, explosive remnants of war.
ERW contribute considerable morbidity and mortality both during and following conflict. As seen in figure 3, children were more likely to be injured by UXO compared with adults, while landmines affected a predominately adult cohort.22–30 It should be noted that statistics on prehospital mortality for children in conflict settings is generally an underestimation due to the difficulties in reporting and monitoring. It should be noted overall that there is limited statistical information available currently to researchers wherever they work with blast-injured children and that thus the percentages used in some of the papers they considered were unable to be supported with the full range of statistical confirmation. It is hoped that this review will provide focus for those organisations that seek to provide statistics on child conflict injuries, for instance, many explosive weapons observation groups do not or who are unable to distinguish between adults and children in their reporting.

{kind=link}
{kind=link}
{kind=link}
Percentage of casualties (injuries and fatalities) by specific modalities.
UXOs have been described as small, colourful and toy-like, promoting child interaction and subsequent injury from handling, resulting in often fatal upper limb, head, neck or chest injury.24 25 31–33 Due to the social nature of children, these interactions commonly occur in groups, leading to multiple casualties in 45%–63% of events involving children compared with 30%–40% in adults.27 30 34
Occupation and education play a role in ERW injuries. It is common for children in LMICs, particularly males, to assist their family with herding and farming as opposed to attending school. This may affect the likelihood to exposure to ERWs through increased freedom to roam where such devices are present.28 35–37 A lack of formal education impacts the child’s ability to read warning signs; only 6%–22% of victims were aware ERWs were present,21 38 and of these, only 0%–11% had received ERW risk education.17 21 35 38
Children are particularly vulnerable to wide-area explosives such as aerial bombardment and shelling, particularly in the primarily urbanised environments of modern conflicts. In the Syrian Civil War, three quarters of wide-area explosives were used in civilian residential areas that children frequent, with these mechanisms responsible for 82% of child deaths.39 40
The following section reviews what is known of mortality in children before reviewing injury types.
Mortality
Comparison of paediatric wartime mortality data is difficult as many studies do not differentiate mechanism of injury. Edwards et al’s41 study on 4913 children between 2002 and 2010 presenting with blast injuries remains the single largest data set. The reported mortality rate of 8% matches well with the mortality rates of 6%–9% quoted in paediatric trauma deaths from Iraq and Afghanistan, although these studies displayed all trauma mechanisms as opposed to specifying blast trauma.35 42–46 Between 2006 and 2013, Thompson et al 47 noted a mortality rate over double of that quoted by Edwards et al following paediatric blast injury in Afghanistan (18%). Operational tempo and the increasing use of IEDs have been hypothesised to underlie these discrepancies in mortality.47
Age-related variation in mortality has been described. Matos et al noted mortality was highest at 24% in young children (5–8 years old),48 while Schauer et al and Spinella et al found greatest mortality in 0–4 years old.49 50 Similarly, Borgman et al and Matos et al noted that children <8 years old had increased trauma mortality compared with 8–16 years old (10%–18% vs 4%–7%),48 51 while Spinella et al noted a similar increase in mortality in young children (<6 years old) compared with 6–16 years old (11% vs 4%).50 Few studies directly compare adult and paediatric mortality, and comparisons between studies are difficult due to methodological differences. What is common is that mortality in children following combat-related trauma is considerably higher than that of paediatric non-combat trauma (2%–3%)52 and adult military combat casualties (1%–3%).53 54
A wide range of paediatric mortality is reported following mine strikes, ranging from 4% from 46%.24–29 31 32 55 56 Shuker57 suggested that approximately half of paediatric victims die within minutes of mine explosion, likely due to penetrating head injury, and catastrophic haemorrhage causing non-survivable injuries, in keeping with adult literature.53 54 Time critical injuries following blasts may represent particular problems in LMICs, where prehospital evacuation chains may be protracted. Coupland nd Korver58 noted that in 1991, only 14% of paediatric and adult ERW victims were admitted in less than 6 hours, while the majority (58%) were admitted between 6 and 24 hours and 28% presented after 24 hours. Even in recent conflicts, Bitterman et al 59 found <10% of children presented within 1 hour, with over a third presenting after 6 hours. Protracted evacuation of paediatric victims adds to blast mortality, reinforced by studies observing a 85%–91% mortality of children either at scene or en route to health facilities.29 57
Vascular injuries
Penetrating injuries occur in 38%–76% of blast-exposed children,9 11 14 23 42 43 45 60 with incidence greater in older children aged 10–16 years old compared with 0–10 years old (65%–83% vs 47%–63%).16 48 In keeping with penetrating injury patterns, vascular injury was observed in 3%–12% of children following blast trauma,9 11 23 61 considerably higher compared with non-blast conflict trauma where vascular injury occurred in 0.6%–1% of paediatric victims.9 14 18 61 62
Vascular damage and subsequent haemorrhage following explosions have been identified as a significant cause of childhood fatalities, ranging from the primary cause of death in 21%–38% during the Syrian Civil War37 63 to 63% following IED and suicide attacks in Pakistan,19 while mortality rates following penetrating injuries in civilian settings are considerably lower (5%).61 Extremity trauma was most highly associated with vascular injuries, with the majority of vascular injuries occurring in the lower limb (38%–58%) followed by the upper limbs (25%–28%).61 64 This is in keeping with adult data where 54% of injuries were sustained to the extremities.53 Despite its high prevalence, extremity vascular wounds confer reduced risk of death compared with vascular damage within the torso, attributed as the primary cause of death in 71% of paediatric deaths and conferring a fourfold increased risk of death compared with extremity vascular injuries.61
Data on vascular damage are clear: older children and adolescents sustain similar rates of vascular injury to adults, particularly to the extremities, while mortality following penetrating trauma is primarily the result of injuries to the vasculature within the torso.
Head injuries
The prevalence of head injuries following blasts are diverse, ranging from 6% to 54%,10–12 14 36 43 45 46 59 61 62 65–70 while adult combat data range from 16% to 29%.53 This variation is due to the heterogeneous definitions of head injury described in these studies, with few studies differentiating between superficial scalp wounds, blunt traumatic brain injury (TBI) or penetrating TBI. Where head injuries were documented, TBI was recorded in 21%–62% of paediatric victims, of which 38%–39% were defined as penetrating.11 69 71 Unsurprisingly, papers noted over double the incidence of paediatric penetrating head injury in blast trauma compared with mainly blunt civilian trauma (13% vs 6%), while the reverse was true in closed head injuries, with half the incidence of closed head injuries in blast injuries compared with civilian trauma (22% vs 44%).9
Cerebral haemorrhage and direct cranial damage following blast have been attributed as a leading cause of death in children, responsible for 46%–71% of fatalities.23 45 65 67 72 Creamer65 noted penetrating wounds to the head accounted for 44% of child deaths in the emergency department (ED), while open skull fractures with cerebral evisceration was documented in 88% of paediatric fatalities following the 1995 Oklahoma City bombings.73 While penetrating head injuries undoubtedly carry high mortality, Woods et al 74 noted that eight children survived to hospital discharge despite penetrating head injuries deemed initially unsurvivable, suggesting such are not unequivocally fatal.
Er et al 67 noted that children were more likely to be injured in the head compared with adults (54% vs 40%) following aerial and shelling during the Syrian Civil War, while young children aged between 0 and 4 years old were more likely to undergo neurosurgical procedures compared with other ages,44 75 48% of which were craniectomies or craniotomies for penetrating brain injury, mainly secondary to IED blasts.75 Suggested reasons for this increase may relate to anatomical predispositions, particularly in infants, such as large head to body ratios in addition to reduced skull rigidity,16 as well as the relatively shorter distance from the head to ground-based ERW and IEDs compared with adults.12 16 25 33 57
There is a clear lack of studies investigating long-term outcomes following blast-associated head injuries. While significant cognitive, intellectual and functional sequelae arising from non-blast TBI (nbTBI) have been described, controversy exists as to whether nbTBI is analogous to blast-induced TBI,76 and the paucity of paediatric data means this comparison is even more problematic.
A unifying message is that head injuries are associated with high morbidity and mortality in paediatric blast trauma, while the long-term consequences remain largely unknown. Head injuries are commonly penetrating compared with civilian practice, and increased operative demand in infants and toddlers for neurosurgical procedures may stretch medical service expertise.
Facial and ocular injuries
Blasts result in injury to the face in between 27% and 48% of paediatric victims, compared with 12% resulting from gunshot wound (GSW)10 12 70 and 10% in adults.53 Relative to other blast-related injuries, facial injuries in isolation are associated with reduced mortality.12 However, Gataa and Muassa77 noted that of the patients presenting with facial injuries, 29% had concomitant eye injury, 22% had TBI, while life-threatening facial bleeding occurred in 10% of patients. In addition to physical sequelae, facial injuries are associated with functional and psychological disorders stemming from stigmatisation of disfiguring injuries with implications for future social, economic and marital prospects.77
Despite only comprising 0.3% of the anterior body surface, the eye is sensitive to blast injury, with ocular injuries in 4%–28% of children following trauma related to combat or ERW.34 36 43 45 59 62 65 66 71 In keeping with patterns of facial injury, an increased prevalence of eye injury is associated with blast injuries compared with GSW (13% vs 3%).10 Landmines are often associated with multiple foreign bodies on the conjunctiva, cornea and sclera, in addition to sight-threatening injuries such as enucleation or eye globe perforation.24 Monocular enucleation was observed in 4%, while bilateral enucleation, and hence blindness, was more common (14%).24 34 Compared with adult victims of landmines and cluster bombs, children have more eye injuries (14% vs 8%)30 as well as twice the prevalence of eye globe perforation (28% vs 14%)67 and complete loss of vision (21% vs 10%).25 Without adequate support, both monocular and bilateral vision loss may translate to developmental and educational deficiencies in the growing child.
Facial and eye injuries are frequent following exposure to blasts,and should raise suspicion of intracranial injury. Important are the social and education implications of these disfiguring injuries in the growing child.
Torso injuries
Following blast injury, trauma to the torso is common, varying from 12% to 46% between studies10 12 19 24 43 45 46 59 61 64–70 and peaking in 5–10 year olds.11 16 Er et al’s67 study on civilian paediatric injuries during the Syrian Civil War noted that the abdomen was less commonly injured compared with adults (12% vs 20%), while chest injury with accompanying lung contusion was present in 51% of children with torso injuries, compared with 35% in adults. Both chest and abdominal injuries from blast are typically classed as ‘severe’.12 Abdominal injuries accounted for 18%–19% of injury-specific deaths following blast in the paediatric population, while chest injuries have been attributed to 8% of deaths in the ED.43 Explanations for this susceptibility to severe and life-threatening torso injuries include a lack of body armour compared with adult combat victims and the observation that children have flexible rib cages allowing greater damage to underlying structures without rib fracture, contributing to the increase in lung contusion observed.61
When organ-specific injuries were examined, blast was most likely to cause open penetrating wounds of the bowel and intra-abdominal organs, affecting the small intestine in over a third (34%) and the liver, spleen or pancreas in 36%.43 78 79 Where internal organ damage was sustained, injury-specific mortality almost doubled from 15% to 29%.63 These injuries were frequently contaminated due to bowel rupture, requiring multiple procedures and a high rate of antibiotic usage.80 The thinner abdominal walls, reduced intraabdominal fat and larger solid organs relative to the body cavity increase the likelihood of visceral damage following penetrating trauma, while delayed signs of visceral damage support the role of repeated examination and radiological input, even in the absence of external damage.
In the context of total operative procedures performed, laparotomies comprised a significant component of total surgical workload, encompassing 12%–23% of all paediatric procedures performed.35 47 81 Children were more likely to require laparotomies following combat trauma compared with paediatric non-combat, and primarily blunt, abdominal trauma (13$ vs 2%). Children in combat zones were also twice as likely to undergo laparotomies compared with US service personnel (12% vs 6%).50 In addition to the high prevalence of abdominal injuries, children frequently swallow air when frightened or in pain, resulting in gastric dilation. As well as increasing vomiting risk, this may erroneously suggest abdominal injury57 and lead to laparotomy. Despite this, Arafat et al 79 noted that only 8% of laparotomies were negative, supporting the role of explorative laparotomies in penetrating trauma following blasts.
Compared with both adults and children in non-conflict settings, the blast-injured child is more likely to sustain injuries to the chest. While abdominal injuries are less frequent, they are more likely to involve visceral damage and require operative management compared with adult combat trauma.
Extremity injuries
Extremity injury is one of the defining features following blast-related trauma. Extremity injuries within conflict zones are observed in just under half of children (45%), its prevalence increasing in blast injuries (69%),70 with a retrospective study finding 100% of traumatic amputations and 96% of bone injuries to hand and foot were secondary to blast injuries.66
Studies describe extreme variation in the prevalence of upper limb injuries following blasts, ranging from 6% to 74%,11 19 22–24 26 35 45–47 59 61 65 66 68 69 82 with the greatest upper limb injury reported following UXO and cluster munition strike.24 31 Compared with adult and particularly following ERW blast, children were more likely to sustain upper limb injuries19 25 27–29 55 with a corresponding increase of 150%–300% requiring operative amputation, typically at the level of the finger.23 28 55 83 Traumatic amputation of the upper limb was common and limited to the hands in 44%–94% of children sustaining upper limb injuries,24 65 while transradial and transhumeral amputation was less frequent (14%–34%)35 69 but were more likely to be bilateral.34 Arm fractures necessitating surgical fixation were observed in 45%,82 while upper limb vasculature was commonly disrupted.61 64 69
Similarly, prevalence of lower limb injuries shows variation between studies on blast affecting 25%–86% of children,19 22–24 35 45 46 59 65 68 69 82 with landmine strikes particularly associated with lower limb injury22–24 ; 20%–29% required operative amputations, normally at the transtibial plane.23 34 65 Lower limb injuries were less common in children compared with adults,25 27–29 56 with incidence lowest in 0–3 year olds,16 while increasing in adolescents to mirror adults.25 Traumatic amputations were less frequent compared with the upper limb, occurring in 14%–35% of lower limb injuries.24 35 69
Landmines drive debris, footwear and clothing upward between planes of the soft tissues and bone, leading to degloving injuries of the leg, perineum and lower abdominal viscera, as well creating serious potential for soft tissue and bone infection in the remaining limb.33 58 While large bony defects of the lower limb are problematic in children,84 reconstruction with limited shortening (<2 cm) has been associated with good outcomes, with the capability for highly active growth plates to remodel and compensate for this.66 85 However, 75% of new growth occurs in the distal femur and tibia growth plates, with the distal limb most prone to explosive disruption.33
The long-term physical, psychosocial and financial repercussions of amputation must not be underestimated. Physical complications are greatest following TA and below knee amputations, and include anterior and varus bowing, heterotopic ossification and osseous overgrowth requiring operative or prosthetic revision.86 Overgrowth is particularly problematic in younger patients (under 12 years), with 15% of patients sustaining amputations requiring re-vision of their stump. Protracted phantom limb sensation (PLS) and phantom limb pain (PLP) are reported in over 50% of children following blast-related amputation, similar to that seen in adult literature following blasts,87 yet over five times higher than in children requiring amputation following non-traumatic indications such as malignancy. Increased PLS has been reported in lower limb amputations, while PLP was increased in upper limb amputations.16 88 Social acceptance of the child amputee is culturally specific, with stigmatisation in certain cultures negatively impacting the child’s psychological, social and educational status.89 While there is a paucity of outcome and long-term costing studies in LMICs, the financial burden of prolonged rehabilitation and repeated revision of prosthesis on the children and host country’s health system is likely to be considerable.89
Like adults involved in blast trauma, older and adolescent children are prone to extremity injury, particularly of the upper limb, while infants and toddlers experience less extremity injuries. Limb injury causes diverse complications in the growing child with increased requirement for re-revision compared with adults.
Burn injuries
Multiple retrospective studies have noted that the majority of burns in children result from civilian mechanisms such as scalding, open fires and flash burns from household cooking fuels,43 51 90–92 while approximately 9%–12% is the result of HEs observed in combat blast modalities,90 92 less than observed in adult combat populations (52%).88 Unlike civilian mechanisms, however, blast-induced burns rarely occur in isolation, with multidimensional injuries playing a significant role in the child’s prognosis.11 92 93 While postmortem findings following the Syrian Civil War attributed only 0.5% of deaths being secondary to burns,63 conflict-related burn victims had higher mortality compared with non-conflict related burn victims (47% vs 3%),91 and significantly greater than blast related burns in adult military populations (5%).88 Severe burns following blasts were sustained in 30% of children and fatal in 36%–40%.12 46
Creamer65 noted the median age of burn victims as 6 years old. At this young age, the anatomical disproportionality of the child increases the total body surface area, resulting in significant burn surface area (BuSA). Thus, approximately half of paediatric burns in conflict zones result in BuSA >15% (32,127), while 13% of children have BuSA exceeding 40%(127). A high BuSA exceeding 40% has been linked to myocardial damage and hypotension, making haemodynamic management challenging, while complications including nosocomial infection of the burn eschar and pneumonia are not uncommon.91 Within LMICs, protein loss and weight-based fluid resuscitation is complicated by malnourishment, while cold fluids may accentuate hypothermia.90
In conflict-related burns, the head and neck are most frequently affected, potentially leading to thermal inhalation injuries.92 93 Thermal inhalation injuries in paediatric victims are difficult to assess, and clues to inhalational injuries such as increased respiratory rate may be incorrectly interpreted in the context of physiological age discrepancies. In addition, the paediatric subglottis represents the narrowest section of the upper airway and deteriorates rapidly from burn-induced laryngeal oedema, especially in the context of failed intubation attempts72 leading to rapid oxygen desaturation. Between 21% and 33% of children were identified as having inhalational injuries requiring pre-emptive or immediate intubation to protect the airways,62 93 similar to that seen in adult combat casualties (26%).88 Of this paediatric cohort with inhalational injuries, 39% died,93 significantly greater than in adult populations (4%).88
Prognosticating factors noted for burns include increased time to presentation, prolonged hospital length of stay and requirement for critical care input.91 This relates to the resource-intensive management of the paediatric burns patient. Like adults, hospital length of stay (LOS) for burns patients are two to three times that of the general paediatric population,45 92 while intensive care unit (ICU) requirements are increased, particularly in burns secondary to blast injuries.91 92 Operative demands of paediatric burn victims are significant. Children aged 6 months to 3 years were between 4 and 14 times more likely than adults to require surgical input, reflecting the significant burden of burns (39% of this cohort compared with 2%–6% in adults73). While other conditions may be treated by a single operation, burns often require serial procedures,73 with an average of two operations per patient. This creates a disproportionate operative volume in both adults and paediatric patients compared with other surgical emergencies.73Burns induced by blast injuries require more escharotomies (27% vs 4% p<0.001) and fasciotomies (67% vs 30% p=0.002) when compared with civilian burn mechanisms.91
Additionally, the requirement for postoperative support and rehabilitation adds to the resource requirements. Children are rarely left without functional sequelae, with limited joint mobility and impaired tactile sensation presenting significant future challenges for rehabilitation,94 while high rates of psychological morbidity including suicidal ideation have been reported in adolescents.95 Under-resourcing psychological and functional rehabilitation will likely lead to high rates of morbidity and mortality.73 The degree to which these services are available within conflict zones and LMICs is uncertain. Ethical questions naturally arise when performing interventions where health systems are unlikely to address a child’s long-term needs. Examination of existing paediatric burn services within zones of interest and longer term follow-up of paediatric blast burn patients are required to determine the problems and needs for this cohort.
Service provision
Relative to total admissions, paediatric victims affected by blasts constitute a disproportionately large resource burden on operative workload, as well as intensive care and hospital beds. Approximately 47%–82% of paediatric blast victims require surgery,11 16 45 47 79 particularly adolescents.16 The requirement for multiple operative procedures was common in the paediatric cohort, especially in burn and orthopaedic surgery due to the requirement for surgical revision (34%–80% of children required ≥2 procedures12 36 43 45 46 65 66 78; 25% required ≥4 procedures).43 Operative requirement was greatest in 9–14 year olds, requiring on average five procedures per patient, prolonged ICU and hospital stay, while 0–3 year olds required the least operative management.44 This study suggested the reduced requirement for operative input in 0–3 year olds may be due not only to the reduced burden of extremity injuries requiring repeated debridement, but potentially because the equipment was inappropriate for this young cohort. This is supported by observations that infants and young children aged 0–10 years old with an Injury Severity Score ≥15 were four times less likely to go to surgery compared with adults, while adolescents (11–15 years) were two times more likely to receive operative input.16
Multidisciplinary surgical services were required in 80% of patients, with orthopaedic, plastic, general neurosurgical, ophthalmic and vascular surgeons often working in partnership.69 Debridement and primary skin closure represented the most common procedure, in 35%–100% of studies,23 35 45 47 50 65 68 82 in keeping with shrapnel injuries leading to multiple and frequently contaminated superficial injuries.68 82 Children are likely to do well with thorough debridement, with well-perfused tissues allowing optimal healing and scar formation.66 85
Retrospective studies of US military medical treatment facilities (MTF) in Afghanistan have found that while children comprised only 3%–6% of their total admissions, this demographic required approximately double the total bed spaces (7%–11%),42 62 96 and on average three times the LOS of coalition troops admitted over the same time period.42 50 Approximately 40% of paediatric admissions required an LOS exceeding 7 days, while in half, the LOS exceeded 14 days.11 14 Spinella et al noted that while children aged 11–17 years old were the greatest proportion of children occupying beds, <1-year-old cohort had the longest stay.50 This contrasts with other studies finding young children<8 years old had the shortest LOS, while children(8–14 years old) had the longest.12 42
A similar burden is observed in the ICU, with between 20% and 45% children requiring ICU admission,5 11 45 49 62 67 78 79 93 the majority following explosive or ballistic trauma. Children were often younger (0–10 years old),16 with one recent study noting children aged <1 year and 1–4 years most often requiring admission (53%–66% respectively).49 Children under 8 years old required an ICU LOS over twice that of children aged >8 years.48 Harris et al 5 noted that despite representing only 12% of admissions, children occupied on average 35% of ICU beds, with a brief surge in numbers resulting in 100% occupancy from children, the majority requiring ventilatory and ionotropic support. This specialised service was often provided by non-paediatric experts, which could result in two healthcare providers per paediatric patient.5 Ventilatory equipment is often age specific, and although multiple examples of ingenuity and adaptation of adult equipment exist,5 78 children may overwhelm the unprepared MTF.
One of the key challenges is providing sustainable health services in the host country. MTFs may be capable of delivering exceptional paediatric care in the acute phase following blasts, but recovery from morbidity is dependent on long-term rehabilitation85 normally provided by the host country. Not only can this place exceptional strain on local health authorities, but if provisions are not available, the child is likely to undergo a protracted decline.5 85 Failure to secure recovery in the long term is likely to result in the limitations in observing the Articles of the UNCRC, as listed in the Introduction to this review.
Reasons for the high rate of admission and prolonged stay may be multifactorial. Admission criteria for host nationals to a coalition MTF typically require threat to life, limb or eyesight, with resulting prolonged stay. Interestingly, however, children with mild to moderate traumata are three times more likely than adults to be admitted.16 This may reflect a lack of certainty in initial assessment of injury severity from health practitioners unaccustomed to dealing with children. Within conflict zones, rearwards evacuation of civilians is not always possible, and health interventions such as ventilatory support may not be sustainable by host countries without deterioration in service standards, leading to prolonged admission until the child can be safely moved.5
Following up recovery is a recurring theme when exploring long-term challenges of blast injuries in children.6 Children are a complex cohort to monitor. Geographical displacement, particularly in the context of a conflict, increases the likelihood of this vulnerable cohort being lost to follow-up. This can impact not only the child’s rehabilitation and coordination with local health authorities, but also cause difficulty in assessing long-term functional outcomes which are needed to detect future health needs. Increasingly, there is recognition of the need for formalised trauma registries accessible in the host country, assisting the follow-up of this vulnerable demographic.6 12 62 96
Conclusion
This review has focused on research based on those child patients injured by blast primarily (although not exclusively) in conflict zones in the Middle East and Afghanistan. Although the papers under review were written by authors from a wide variety of nationalities and professions that encounter paediatric blast injury and its effects, they all wrote in English for journals which assumed a level of English fluency in their readership. Non-English research, both written and published in non-English journals, was outside the purview of the study. The authors of the study sincerely hope that future work will be able to address this by comparing research on paediatric blast injury done in settings and with study parameters that may differ from those considered here. In doing so, a truly global understanding of the condition may be achieved, beyond our focus on today’s conflict zones.
Most paediatric blast injury is inflicted in these settings but is not exclusive to them. In Britain in May 2017, a bomb detonated at the Manchester Arena killing 23 people and injuring 139, most of whom were children. The attack placed a sudden and significant burden on medical services in the city, which had no experience of paediatric blast injury in the 21st century, let alone on this kind of scale.
Wherever in the world they live, and whatever the circumstances of the explosion, the social and anatomical profile of children makes them uniquely vulnerable to one of the most complex and demanding trauma conditions that any medical professional or system can treat. This paper has characterised paediatric blast as a diverse injury pattern, which must be seen as distinct from its adult equivalent. This pattern should be fully understood from point of wounding through the postoperative and rehabilitation phases of treatment. This continuum approach would enable both better long-term care of the patient and improved support of medical systems bearing the intense burden of that care.
It remains to be seen whether the monitoring of the long-term effects of paediatric blast injury in well-resourced environments is any better than that in areas of instability. Monitoring of patient outcomes should be integrated with the monitoring of treatment so that relevant practice and skills can be continually assessed. Thus, the authors join with other organisations concerned with the welfare of the world’s children (such as the recently established BRANCH Consortium—Bridging Research and Action in Conflict Settings for the Health of Women and Children) in calling for immediate action to fill the evidence and policy gaps relating to child conflict injury and the interventions needed to improve its long-term outcomes.
It has been our intention in conducting this review to provide specific technical medical detail of one of the greatest horrors in our world today—that of the direct effects of war on children. We hope it will be useful to everyone, from medical researchers to humanitarian organisations, who seek to mitigate those effects, and secure the safety and well-being of children wherever they grow up. It is not only coherence in treatment and understanding of child blast injury that is required, it is a restatement of global commitment to the UNCRC, so that today’s horrors will not become those of tomorrow.
Supplemental material
Acknowledgments
The authors are grateful to Dr David Inwald for his detailed comments on this review.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.
- 98.
- 99.
- 100.
- 101.
- 102.
- 103.
- 104.
Footnotes
Contributors JMH was responsible for the analysis of the data and the writing of the main body of the work. AB and ERM made substantial contributions to the concept of the work. AB supervised the design and analysis of the bioengineering material used by JMH. PP and JMH acquired and sorted the medical journal articles for relevance to the field. PP oversaw the analysis for tables and figures and substantially contributed to the general supervision of the overall project. ERM contributed the Introduction and Conclusion text material. AB, ST, PP and ERM gave extensive critical revisions for important intellectual and technical content and approved the final version of the draft. All authors have agreed to be accountable for all aspects of the work. ERM is the corresponding author and is responsible for submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement There are no data in this work.