Article Text

Abstract
Objective To identify studies that highlighted medication administration problems experienced by parents and children, which also looked at health literacy aspect using a validated tool to assess for literacy.
Study design Ten electronic databases were systematically searched and supplemented by hand searching through reference lists using the following search terms: (1) paediatric, (2) medication error including dosing error, medication administration error, medication safety and medication optimisation and (3) health literacy.
Results Of the (1230) records screened, 14 studies were eligible for inclusion. Three analytical themes emerged from the synthesis. The review highlighted that frequencies and magnitudes of dosing errors vary by the measurement tools used, the dose prescribed and by the administration instruction provided. Parent’s sociodemographic, such as health literacy and language, is a key factor to be considered when designing an intervention aimed at averting medication administration errors at home. The review summarised some potential strategies that could help in reducing medication administration errors among children at home. Among these recommendations is to show the prescribed dose to the parents or young people along with the verbal instructions, as well as to match the prescribed dose with the measuring tool dispensed, to provide an explicit dose intervals and pictographic dosing instructions.
Conclusion The findings suggest that in order to optimise medication use by parents, further work is needed to address the nature of these issues at home. Counselling, medication administration instructions and measurement tools are some of the areas in addition to the sociodemographic characteristics of parents and young people that need to be considered when designing any future potential intervention aimed at reducing medication errors among children and young people at home.
- pharmacology
- qualitative research
- health services research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Medication administration errors occur frequently among children.
Parent’s health literacy could be associated with medication administration problems in children.
Studies examining parent administrator paediatric medicine accuracy were mainly from one particular research group in the USA with participant parents using non-standardised measuring tools.
What this study adds?
The nature of medication administration error’s happening at home are not well documented across each age group.
The need to explore parents and patients perspective in regards to medication administration challenges happening at home.
Introduction
When it comes to medication administration for children at home, a significant burden of responsibility relies on the parents or on the patients themselves.1 It has been documented that medication administration errors among children is well known to occur.2 Previous studies recognised that more than 40% of parents and caregivers make dosing errors in an outpatient setting.3 4 The inability to administer medication correctly may result in adverse drug events and poor patient clinical outcomes.5 Causes of medication administration problems at home are multifactorial and potentially depend on various factors.2 So, in order to improve medication administration by parents and patients, an initial assessment of the current problems and factors that may contribute to this issue must be identified first.
Previous studies have recognised potential factors that can contribute to clinician-led medication administration errors in children, but there have been no studies recording both the types and risk factors that can contribute towards caregiver’s medication administration problems as well as young people.6 7 According to the European Health Literacy Survey, conducted across eight different countries, the prevalence of low health literacy levels varies from 29% to 62%.8 9
Owing to this, high prevalence of low health literacy levels and its potential association with medication administration issues among children. This review aimed at identifying studies that highlighted medication administration problems experienced by parents and children, which also looked at health literacy aspect using a validated tool to assess for literacy. In this systematic review, the common medication administration problems occurring at home as well as the potential causalities and risk factors other than health literacy that further could contribute to medication administration errors have been highlighted.
Methods
This review was conducted in accordance with the Cochrane Handbook for Systematic Reviews, and followed Preferred Reporting Items for Systematic Reviews andMeta-Analyses (PRISMA) reporting guidelines.10 11 The review protocol is registered on PROSPERO (ID: CRD42018091590).
Patient and public involvement
There was no patient and public involved in the design, or conduct, or reporting, or dissemination of this review.
Eligibility criteria
Studies were eligible for inclusion if they were related to medication administration errors among children and adolescent between the ages of 0–18 years old as per the WHO definition of population age group. This includes studies reporting medication-related problems outside the clinical setting; where the parent or the child is responsible for administering or taking the medication. Studies must have assessed the health literacy levels of the participants using a validated health literacy assessment tool. Any study that looked only at education levels of the participants without assessing the literacy levels was excluded. There were no restrictions on the date of publication, only English language articles studies where included.
Search strategy
The search strategy was designed initially by the research team and verified by an information specialist using the Population, Intervention, Comparison and Outcomes model. The reviewer (DTD) systematically searched PubMed, Scopus, Web of Science, Cochrane Library, OpenGrey, NHS Digital Department of Health Office for National Statistics, BBC News, Bielefeld Academic Search Engine, E-thesis Online Service and Conference proceedings through Web of Science for studies from database inception to September 2020.
Search terms summarised in online supplemental material, table S1 included a comprehensive list of synonyms and multiple Boolean operators relating to: (1) paediatric (2) medication error including dosing error, medication administration error, medication safety and medication optimisation and (3) health literacy. DTD further performed reference tracking of all included studies to identify any potential studies to be included in the review.
Supplemental material
Study selection
Two reviewers (DTD, ZBS) independently evaluated each study for eligibility to reduce bias using the inclusion criteria above. The titles and/or abstracts of all identified studies were reviewed independently, and full manuscripts that appeared to potentially relevant.
Data extraction process and synthesis
Two reviewers (DTD and ZBS) independently extracted data using a standardised predefined spreadsheet. Inconsistencies in extracted data were resolved through consensus discussion by a third reviewer (CH), if necessary. Results were synthesised and summarised according to analytical themes. Thematic analysis was opted by the research team as it is known for its flexibility and ability of identifying patterns of meaningful information within the data.12
Quality appraisal
The quality of the included papers was independently assessed by two reviewers (DTD, ZBS) using Critical Appraisal Skills Programme checklists.13 14 Discrepancies were resolved through discussion and consensus.
Results
A total of 672 citations were retrieved from the database and other searches. After screening titles and abstracts, 38 publications were obtained in full text and assessed for suitability. Of which, 14 met the inclusion criteria and were included in the analysis (see figure 1 for PRISMA flow chart). 15–28 See online supplemental material, table S2 for reasons of exclusion.
Supplemental material

Flow diagram for the study selection based on Preferred Reporting Items for Systematic Reviews andMeta-Analyses flow diagram.
The details of the 14 studies are presented in (tables 1 and 2). 15–28 The majority of the included studies were published in the last 12 years. All of the studies (n=14) took place in the USA.
Characteristics of the observational included studies in the review (listed by health literacy test)
Characteristics of the randomised controlled experiment included in the review (listed alphabetically according to first author)
Overall, 11 studies recruited parents or caregivers of children aged between 30 days to less than 9 years old, 2 studies had recruited parents with no age limitations of the child and 1 study recruited only women of childbearing age. The majority of the studies (n=13) did report the ethnic composition of their recruited sample and they were vastly Hispanic or black African American parents or caregivers. One study had only exclusively recruited women from a white ethnic background.22
Quality appraisal
The results from the quality appraisal are shown in online supplemental material, tables S3 and S4. All identified studies were included in the final synthesis with a greater emphasis on the higher quality studies.
Supplemental material
Synthesis of results
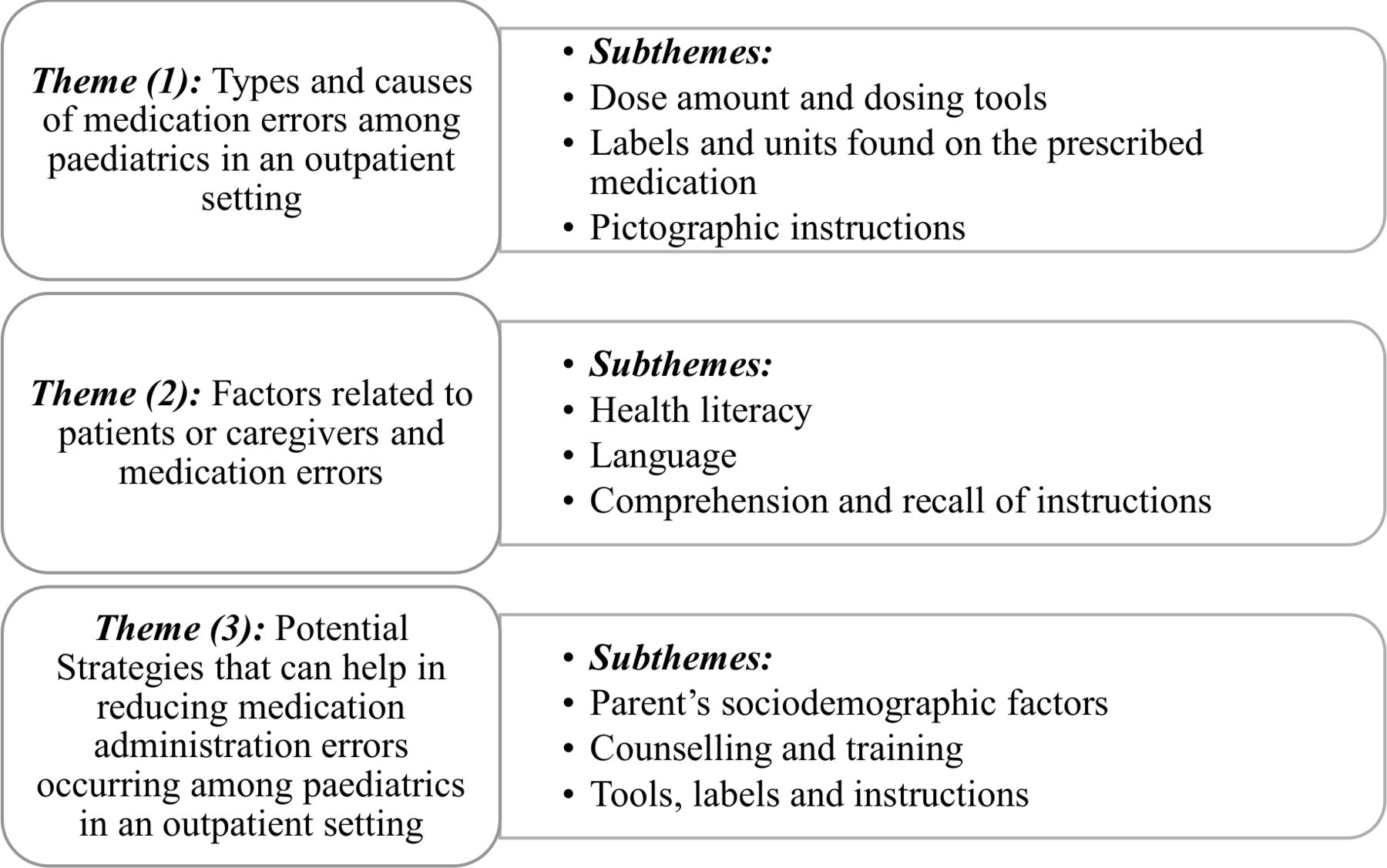
The data from the 14 studies were analysed and three analytical themes emerged from the analysis and a summary of the review results are demonstrated in figure 2.

{kind=link}
{kind=link}
List of the review results.
Types and causes of medication administration errors among children led by parents or child outside a clinical setting
Eight of the included studies indicated that paediatric dosing errors are among the most common medication errors made by parents.15 18–21 23 24 26 Among these studies, two randomised trials identified that overdosing errors are more common among parents.23 24 While another cross-sectional study looking at parents with child on a short course prescribed medication reported that the majority of the parents measured below the prescribed dose.15 A study by Morrison et al 20 reported that parents who made underdosing errors made more dosage errors and frequency errors compared with those who made an overdosing error.
From the included studies, it was noticed that the magnitude and frequency of dosing errors by parents were influenced by two factors: measurement tool used by parents and the dose volume (amount) . In one study, parents stated that non-standardised kitchen spoon was their primary dosing tool.17 Two studies reported that errors were more common with measuring cups than with syringes, in particularly with small dose volumes (amounts).21 24 In a cross-sectional study conducted in the USA, the majority 66% of the parents considered oral syringes are the best tool for dosing accuracy, while 23.5% believed that cups were the best; however, few 10.1% believed that dosing spoon, measuring spoon, kitchen teaspoon and droppers were the best.27 Another study reported that larger dosing errors (>40% deviation of the recommended dose) were made by parents using cups with printed marking and etched markings; this was thought to be due to confusion about teaspoon versus tablespoon instructions, assumptions that the cup is the unit of measure and the full cup is the dose.16 Labels and units of the prescribed medication were contributing factors to dosing errors.24 Parents made significant dosing errors when the units found on the medication bottle label were not similar to the units used on the dosing tool.24 Parents who used teaspoon/tablespoon units were likely to use a non-standardised dosing instrument and make errors in measuring the prescribed and intended dose.19 The final potential factor was the type of instructions provided. For liquid medication, less errors were seen among parents who were provided with text-plus-pictogram instructions 43.9% compared with text-only instructions 59.0% and this group were also less likely to make overdosing errors.26 Parents who received standard medication counselling were 47.8% more likely to make dosing errors when compared with parents who received pictogram instruction (5.4%).25
Factors related to patients or caregivers and medication errors
Health literacy
Health literacy of caregivers in the studies were assessed; six conducted further analyses of its influence on dose accuracy and other cofactors related to medication errors. Yin et al 17 reported that caregivers with inadequate or marginal health literacy were more likely to use a non-standardised dosing instrument and further lacked knowledge on weight-based dosing for over the countermedication when compared with caregivers with adequate health literacy. Another study by Yin et al 16 found a significant association between health literacy and dosing errors using cups and dosing spoons. In adjusted analysis conducted by Williams et al,27 they found that there was a strong association between health literacy levels and measurement tool preference in particular cups, parents with limited literacy reported that dosing cups were the tool of choice most of the time (aOR=2.4). The use of a teaspoon/tablespoon was associated with errors in the intended dose for those with low health literacy but not for those with adequate health literacy.19 Harris et al 21 identified that parents with limited health literacy and limited English proficiency (LEP) made the most dosing errors. Similarly, Samuels-Kalow et al 18 revealed that parents with inadequate and marginal health literacy committed dosing errors, but the sample size of this group was small compared with the adequate health literacy group.
Language
Association between health literacy and lack of knowledge of weight-based dosing varied by English speaking caregiver’s. For English speaking caregivers, 88.6% of inadequate or marginal health literacy caregivers were unaware of weight-based dosing in comparison to 54.1% of caregivers with adequate health literacy.17 In contrast, Yin et al 26 found that there was no significant relation between dosing error and LEP. However, there were some differences in teaspoon-associated errors in measurement by language.19
Comprehension and recall of instructions in relation to parent sociodemographic status
Yin et al 25 reported that parents from a low sociodemographic status who were prescribed a daily dose and who received a simple language, pictogram instructions sheets, were less likely to make errors in knowledge of dose frequency and dose accuracy compared with the control group who received standard medication counselling (0% vs 15.1%). Participants among the interventional group were less likely to report incorrect medication preparation related to shaking the medication before administration for both daily doses (10.9% vs 28.3%, p=0.04) and as needed medication (21.5% vs 43.0%).25 Participants in the interventional group were less likely to use a non-standardised measurement tool compared with the parents in the standard group (daily dose: 93.5% vs 71.7%; as needed: 93.7% vs 74.7%).25 Torres et al, 28 a cross-sectional study that analysed data from a randomised control study, looked at parents preference and perceptions in regards to units of measurements. It was found that over 80% of the parents perceived a change to millilitre only instructions would be easy in comparison to 14% found it some how hard and 4.1% very hard.
Interventions aimed at reducing medication administration errors occurring among children outside a clinical setting
Parent’s sociodemographic factors
Four studies suggested that parental sociodemographic risk factors should be considered when designing an intervention aimed at averting medication administration errors.16 17 21 26 Among these factors were parents’ health literacy as well as language. Kalow et al suggested that efforts to streamline interpreter services must be continued as well, to having a more formalised approach in place to elucidate the patient’s preferred language for communication.18
Counselling and training
Three studies suggested that provisional dose counselling (showing the patient how to prepare the dose) in combination with verbal counselling could be associated with less dosing errors.15 17 23 A study by Yin et al 15 indicated that errors occur across different counselling approaches, and they have recommended developing new strategies to ensure that parents understand medication instructions as well as the need for further research to identify the best counselling strategies and how to incorporate these within clinical practice. Yin et al 24 suggested the need for intensive teaching, training and coaching programmes that can accommodate for different parental health literacy levels.
Tools, labels and instructions
Yin et al suggested a promising strategy that could potentially help to reduce paediatric-dosing errors, which was to match the dosing tool with the prescribed dose volume and move towards more simplified numerical markings on the measurement tools as well as to move to millilitre-only units.24 26 28 Wallace et al 22 indicated in his study that some parents would prefer instructions with explicit dosage intervals with the exact time and dose to be specified on the label. Harris et al 21 suggested improving the availability of language concordant labels that could accommodate for different health literacy levels. Three studies from this review strongly suggested the importance of using pictographic dosing instructions and how it could be a positive aid in reducing paediatric dosing errors.23 25 26 Majority of parents would be comfortable with millilitre dosing instructions only.
Discussion
The results of this study suggest that parents appear to make a range of medication errors, particularly with liquid medications as documented by prior studies that were conducted also in the USA as well as studies from this review.2 4 23 25 The majority of the included studies indicated that dosing errors were among the most common medication errors made by parents, which is consistent with another study, which was conducted on Spanish-speaking Latino parents.15 19 21 25 29 This review identified possible causality behind parents dosing errors other than just the effect of health literacy; these errors could be linked to the: dose volume prescribed, measurement tools used, units used on the labels and the instructions provided.
Although standardised measurement tools are usually dispensed with the prescribed liquid medications in the UK, this review identified that the studies published in the USA indicated that parents still use non-standardised liquid dosing tools as their primary measuring tool; this has been previously linked with medication administration errors by both Yaffe et al and McMahon et al.30 31 The review found that pairing the medication labels to the closest measurement tool size, particularly for millilitre-only labels and tools, could be associated with a reduction in parent dosing and administrating error rates, as well as a decrease in the likelihood of parents using non-standardised measurement tools as suggested by another research.19 32
The review showed that the use of simple pictographic-based medication instructions with explicit dosage intervals could reduce dosing errors by parents. This finding was consistent with previous existing data from both South and West Africa as well as the USA regarding the use of pictographic illustrations as a supportive tool to aid parents in administering medication to their children correctly.33–41 Potentially, this could benefit both parents and caregivers with limited or low health literacy levels.
Our findings are consistent with prior USA studies investigating the link between adult’s sociodemographic factors, particularly health literacy, and medication administration problems.42–45 Four studies explicitly highlighted that sociodemographic factors, such as health literacy and language, must be incorporated into any future intervention that aims to reduce parental dosing and administration errors.
The results of the review highlighted several interventions to aid parents and patients to potentially reduce medication administration errors at home. This include the use of plain language combined with provision of using the dosing tool provided as well as incorporating pictographic instructions which were consistent in four of the included studies.15 23 25 26 Pictographic-plain instructions significantly improve the accuracy of dosing and administering medication to children especially for those parents with insufficient health literacy.25 26
This study emphasised potential areas that could be incorporated into real practice that could help with reducing medication administration errors done by parents/caregivers and patients. Potential strategies include personalised training and coaching that accommodate different health literacy levels and languages as well as the possibility to match the dosing tool with the prescribed volume alongside the use of millilitre units.
Our review is subject to several limitations. There were two major limitations to our study. First, we only included studies in English, so publication bias may exist and non-English studies that are related to this topic might have been missed. Second, we only included studies that evaluated literacy using a validated tool. This resulted in only studies from the USA being included. The excluded studies that are of relevance to the topic, but outside the scope of this review are listed in (online supplemental table S2). Literacy is a problem worldwide, but of greater importance in low-income and middle-income countries. Future reviews should include these studies by broadening the search strategy.
Furthermore, although the study aimed at including medication administration challenges for younger people aged between 16 and 18 years old, however, none was included, as they did not pass the eligibility criteria for this review. Future research are needed where younger people aged 16–18 years old are included as participants. In addition, the generalisability of the study results maybe low; this is because the majority of the studies were conducted in the USA and emerged from the same research group Yin et al. This research group has highlighted several limitations in their studies, such as the use of hypothetical scenarios that might not be a true reflection on how parents measure the dose at home.16 23 24 26 For some randomised trial studies in this review, it was difficult for the research team to maintain blindness as some of the participants revealed their allocated group, while for the cross-sectional studies, no conclusion of the causes could be drawn.17 19 25 Finally, the date of publication for one of the studies was 13 years old,17 which would not take into account the changes that have occurred in terms of interventions that would vary locally, nationally and internationally. However, this review highlights that non-standard dosing still occurs to date due to parent preference based on recent evidence in 2018.28
Conclusions
The findings suggest that in order to optimise medication use by parents, further work is needed to address the nature of these issues at home. Counselling, medication administration instructions and measurement tools are some of the areas in addition to the sociodemographic characteristics of parents and young people are among the factors to be considered when designing any future potential intervention aimed at reducing medication errors among children and young people at home.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @DaniaDahmash
Presented at The review preliminary results was published on the BMJ (Archives of Disease in childhood) after an abstract was submitted for the NPPG 2018 conference for the purpose of poster presentation.
Contributors All authors have contributed in this manuscript.
Funding Aston University, Birmingham, UK, is funding Dania Dahmash PhD project, which as part of her project this review was conducted.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. All data relevant to the study are included in the article or uploaded as supplementary information. All data relevant to this study is included within the manuscript.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.