Article Text

Abstract
Objective There is evidence that birth and care in a maternity service associated with a neonatal intensive care unit (NICU) is associated with improved survival in preterm babies born at <27 weeks of gestation. We conducted a systematic review to address whether similar gains manifested in babies born between 27+0 and 31+6 weeks (hereafter 27 and 31 weeks) of gestation, or in those with a birth weight between 1000 and 1500 g.
Methods We searched Embase, Medline and CINAHL databases for studies comparing outcomes for babies born between 27 and 31 weeks or between 1000 and 1500 g birth weight, based on designation of the neonatal unit where the baby was born or subsequently cared for (NICU vs non-NICU setting). A modified QUIPS (QUality In Prognostic Studies) tool was used to assess quality.
Results Nine studies compared outcomes for babies born between 27 and 31 weeks of gestation and 11 studies compared outcomes for babies born between 1000 and 1500 g birth weight. Heterogeneity in comparator groups, birth locations, gestational age ranges, timescale for mortality reporting, and description of morbidities facilitated a narrative review as opposed to a meta-analysis.
Conclusion Due to paucity of evidence, significant heterogeneity and potential for bias, we were not able to answer our question—does place of birth or care affect outcomes for babies born between 27 and 31 weeks? This supports the need for large-scale research to investigate place of birth and care for babies born in this gestational age range.
- neonatology
- evidence based medicine
- health service
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Babies born at <27 weeks of gestation in maternity services linked to neonatal intensive care units (NICU), compared with local neonatal units (LNUs) have improved outcomes.
Babies born between 27 and 31 weeks of gestation form a considerably larger patient group, and, in the UK are cared for in both NICU and LNU settings.
What this study adds?
In nine studies addressing place of care for babies born between 27 and 31 weeks of gestation, there was significant heterogeneity in study design and outcomes, and potential for bias.
Systematic review of the published literature reveals a lack of evidence about place of birth for babies born between 27 and 31 weeks of gestation.
Large-scale research studies are needed to determine the effect of place of birth on outcomes for babies between 27 and 31 weeks of gestation.
Introduction
The concept of regionalisation was introduced into neonatal care in the 1970s, with the aim of improving outcomes while reducing associated costs.1–8 Worldwide, especially in resource richer settings, this system has been implemented through clinical networks. Perinatal centres (comprising fetomaternal and neonatal units) of different levels work together to care for mothers and their babies in a unit which is close to home and can provide the appropriate level of care.
In the USA, Australia and New Zealand, and in many parts of Europe, care is centralised and all babies born at <32 weeks of gestation and/or of very low birth weight (VLBW; <1500 g) are provided with tertiary level care in neonatal intensive care units (NICUs) (table 1). In the UK, due to concerns regarding the time and travel burden this would impose on families, and unit capacity and staffing, a more regionalised system was implemented, consisting of three-tiers (NICU, local neonatal unit (LNU) and special care unit (SCU)), with both NICU and LNU caring for babies born at <32 weeks of gestation (table 2).9
International summary of organisation of neonatal care services, extracted from national guidelines and relevant reviews
Summary of differences between three levels of neonatal care within the UK, adapted from British Association of Perinatal Medicine61 62
There is evidence supporting both models of neonatal care provision. EPICure 2 and similar international studies show that, for preterm births at <27 weeks of gestation, birth in a maternity service with a NICU, as opposed to an LNU, is associated with significantly better rates of survival to discharge.10–13 Similarly, a meta-analysis by Laswell et al and more recent studies have shown improved outcomes when all babies born <32 weeks of gestation and/or of VLBW are cared for in NICU.14–18
Therefore, in babies born <27 weeks there is a similar care pathway internationally; they are cared for in NICU. This is not true for babies born between 27+0 and 31+6 weeks (hereafter 27 and 31 weeks) of gestation. Specifically, within the UK these babies may be born and cared for in a centre with either a NICU or LNU, depending on maternal choice at booking, presentation to the nearest hospital, and neonatal unit cot availability and staff capacity at the time of delivery.
Babies born between 27 and 31 weeks account for around fourfold more throughput in neonatal units compared with those born at <27 weeks, and make up 12% of all preterm babies born in England. In 2014, they used twice as many neonatal bed days per year compared with the <27 weeks group.19 20 Therefore, we wanted to investigate whether birth or care in a NICU as opposed to an LNU affects outcomes for these babies as it does for their more preterm counterparts. To answer this question, we conducted a systematic review.
Methods
Criteria for considering studies
Our aim was to identify studies comparing outcomes for babies born between 27 and 31 weeks of gestation by the designation of neonatal unit linked to the maternity services where the baby was born or subsequently cared for (NICU vs non-NICU setting). To ensure we were not excluding evidence from studies published before the 1980s5 21 22 and from countries which categorised babies by birth weight as opposed to gestational age,17 23 24 we also included studies comparing outcomes for babies with a birth weight between 1000 and 1500 g. Of the commonly used birth weight stratifications, this weight range best aligned with the 50th centile for weight for preterm babies born between 27 and 31 weeks of gestation (see online supplementary figure S1).
Supplemental material
Literature search
We conducted a search in Embase, Medline and CINAHL databases (1977–2018), using terms related to our patient group (including ‘newborn, neonate, premature, preterm, infant, low birth weight’), intervention (including ‘regionalisation, centralisation, level of care, size, volume, maternal/neonatal transfer, inborn, outborn’) and outcomes (including ‘mortality, morbidity, death, survival’). We did not specify specific morbidities within our search strategy (for the full search strategy, see online supplementary figure S2). Articles were analysed by AQTI and TP, with EMB arbitrating any differences of opinion as to suitability for inclusion. Study authors were contacted for further information if the gestational age range contained or overlapped with, but was not exactly 27 to 31 weeks, or outcome data were in a non-numerical format. The reference lists of articles retrieved from the search, and three systematic reviews on this topic were analysed,14 25 26 as well as a search for relevant ‘grey’ literature (including research and industry reports, conference proceedings, theses, preprints, etc) in OpenGrey, Scopus, Embase and Web of Science databases (1977–2018). All searches were limited to the English language.
Supplemental material
Analysis
To determine the feasibility of meta-analysis, we assessed articles included in the systematic review for uniformity of study characteristics, patient populations, and outcome measures. We assessed risk of bias in included studies using a modified version of the QUIPS (QUality In Prognostic Studies) tool.27
Results
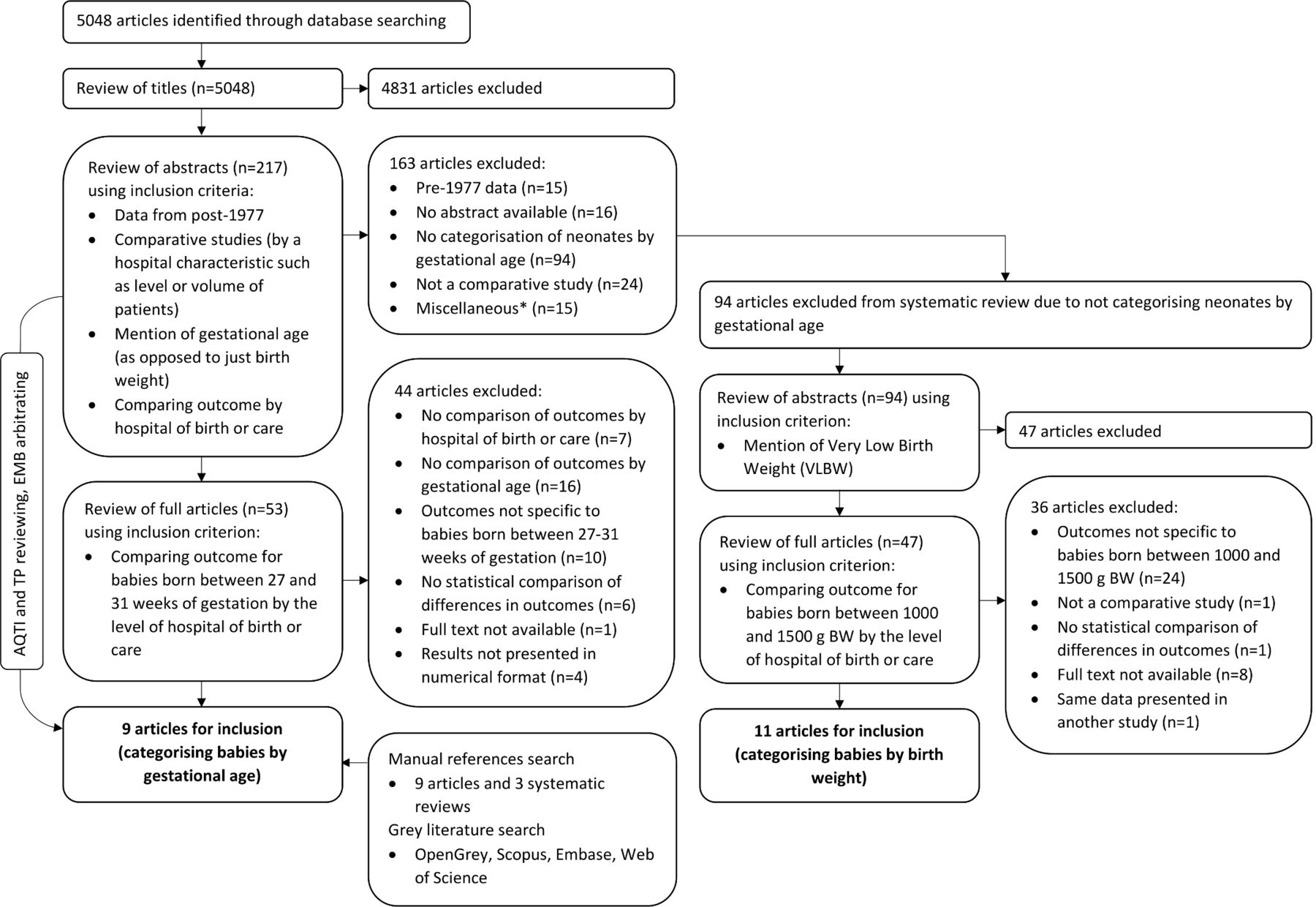
Of the 5043 articles identified (figure 1), 9 studies were eligible for inclusion based on reporting outcomes for babies born between 27 and 31 weeks of gestation by designation of hospital of birth or care.13 28–35 A further 11 studies were identified based on birth weight categorisation (1000 to 1500 g).1 18 36–44 In these, it was not possible to extract information about those born between 27 and 31 weeks to allow comparison with the nine other studies. There was heterogeneity in multiple areas—comparator groups, gestational age comparisons, timeframe for reporting mortality and description of morbidities (table 3). Therefore, a meta-analysis was deemed inappropriate and a narrative review was conducted.
{kind=link}
Flow diagram showing results from systematic review search strategy for studies categorising neonates by gestational age and birth weight. *Miscellaneous include studies excluded due to comparing outcomes in NICU versus NICU/a geographical area/paediatric hospitals/neonatal care in a non-regionalised healthcare system; studies investigating degree of regionalisation/incidence and avoidability of ex utero transfers; and studies comparing birth asphyxia in term infants/success of using early nasal CPAP. BW, birth weight; CPAP, continuous positive airway pressure; NICU, neonatal intensive care unit.
Study characteristics and outcomes for studies characterising neonates by gestational age and birth weight
The studies were all of cohort design but could be divided into three groups based on the following comparators (table 3): (group 1) inutero versus exutero transfer to a NICU for continued care; (group 2) birth at a maternity service linked to a NICU versus non-NICU irrespective of subsequent main place of care; (group 3) main place of care in a NICU versus non-NICU, irrespective of the place of birth. Here, place of care referred to either the entirety of care (peripartum and postnatal) or the level of unit of care after the baby was transferred exutero.
Mortality, based on location of birth/care
Group 1 (inutero versus exutero transfer to a NICU):
We identified five studies that categorised babies by gestational age. Two found significant differences in survival to discharge28 and infant mortality,13 respectively, although Lamont et al found this only for babies born between 28 and 29 weeks of gestation. The other three studies did not find a significant difference.31–33 Of the four birth weight studies investigating this outcome, three found a significant difference (in neonatal mortality,44 predischarge mortality38 and survival up to 2 years of age42).
Group 2 (birth at a maternity service linked to a NICU vs non-NICU):
Of the two gestational age studies, neither found a significant difference in mortality.29 34 Of six studies categorising babies by birth weight, three studies1 36 43 found a significant difference in neonatal and infant mortality and three did not.18 37 41
Group 3 (main place of care in a NICU vs non-NICU):
Of the two gestational age studies in the third group. Jonas et al found a significant reduction in neonatal mortality,35 but Field et al did not (undefined timeframe).30
Morbidity, based on location of birth/care
Group 1 (inutero vs exutero transfer to a NICU):
Of the five studies that categorised babies by gestational age, there were conflicting results for incidence of intraventricular haemorrhage (IVH)28 33 and respiratory distress syndrome (RDS).32 33 A significant reduction was found in the incidence of chronic lung disease in babies born between 27 and 29 weeks (but not between 30 and 31 weeks),33 and no significant difference found for necrotising enterocolitis (NEC) and retinopathy of prematurity (ROP).33 Two birth weight studies also provided conflicting results for incidence of IVH.39 40
Group 2 (birth at a maternity service linked to a NICU vs non-NICU):
Two studies looked at morbidity outcomes. The gestational age study found an insignificant difference in the incidence of asphyxia (not strictly an outcome, but reported as such in this study).34 The birth weight study found significant reduction in composite outcomes of bronchopulmonary dysplasia or death, IVH (grade III or IV) or death, ROP or death, but not NEC (Bell stage II or III) or death.18
None of the identified studies specifically investigated babies born between 27 and 31 weeks of gestation; data presented here was within the context of larger gestational age ranges. We did not identify any gestation-specific data (ie, by week of gestational age).
Quality assessment
Results of quality assessment of the nine studies that categorised babies by gestational age are summarised in table 4. Further details for these, and the 11 studies categorising babies by birth weight are provided as online supplementary tables S1 and S2.
Supplemental material
Supplemental material
Assessment of study quality (categorising babies by gestational age) using modified QUIPS tool (for in-depth analysis, see online supplementary tables S1 and S2)
Of the nine studies, none were of reasonable quality across all five domains of our modified QUIPS tool. One study was of reasonable quality across three domains,29 four studies across two domains13 33–35 and four studies across zero domains.28 30–32 Most significant sources of potential bias included inclusion of babies with life-threatening congenital anomalies, lack of definition of non-NICU birth locations, inclusion of birth settings in which an inadequate level of care would be provided (ie, home, or hospitals without obstetric or paediatric units) and lack of adjustment for confounding factors.
Discussion
This is the first review to investigate outcomes of preterm babies born between 27 and 31 weeks of gestation by the level of neonatal unit of birth and/or care. Overall, the evidence identified in our review was limited, conflicting and prone to bias. The literature was heterogeneous with respect to gestational ages studied, study design and outcomes.
Strengths of our review include the use of a comprehensive search strategy and inclusion of studies based on birth weight between 1000 and 1500 g to avoid exclusion of relevant data. A limitation is the exclusion of non-English studies. A narrative review was undertaken since a meta-analysis was not appropriate, reflecting the quality of available literature.
There have been two previous similar systematic reviews. In the 1980s, Ozminkowski et al25 carried out a meta-analysis investigating neonatal mortality for babies with birth weight <1500 g by hospital of birth. They identified 19 articles (1972–1984), a meta-analysis of which showed that odds of neonatal mortality for inborn babies was 62% of that for outborn (OR 0.62, 95% CI 0.55 to 0.69), but with a significant degree of heterogeneity. Subgroup analysis of the eight studies which provided data on babies with a birth weight between 1001 and 1500 g (n=3180) revealed consistent, statistically significant OR in favour of inborn status (0.53, 95% CI 0.36 to 0.79). The type of studies included (inborn vs outborn) is similar to the five we identified comparing inutero and exutero transfers.38–40 44 However, Ozminkowski et al did not provide information on level of unit or birth location from which outborn babies were being transferred to NICU.
Considering the overall group of preterm babies born at <32 weeks, Lasswell et al14 conducted a meta-analysis of studies from 1976 to 2010, in which neonatal or predischarge mortality data were provided for births in level 3 units compared with lower level units. Forty-one studies met their inclusion criteria, from the USA, Canada, Europe, Australia, Israel and Ghana. Studies were classified as of insufficient quality if they provided ‘no hospital information or lack of clear description of the distinction between hospital levels’. Even when excluding these studies, their meta-analysis showed increased odds of mortality for birth in non-level 3 units for VLBW (36% vs 21%; adjusted OR (aOR) 1.60, 95% CI 1.33 to 1.92) and very preterm (12% vs 7%; aOR 1.42, 95% CI 1.06 to 1.88) babies. Subgroup analyses were only performed for babies with birth weight of <1000 g.
Watson et al45 advanced this analysis, by identifying that within this cohort of babies, it was predominantly those born at <27 weeks of gestation for whom place of birth had a major impact. They showed that care in a high volume (within the top quartile) or tertiary neonatal unit (NICU) was associated with significantly lower mortality to discharge for babies born at <27 weeks, but not for those born between 27 and 32 weeks of gestation.
However, this analysis could be taken a step further, by exploring outcomes by week of gestation for babies born between 27 and 31 weeks. This population represents a heterogeneous group; at the lower end of this gestational age range they often require significant intensive care interventions, whereas lower dependency care may be appropriate for the more mature babies. Across the whole spectrum of gestational age, the risk of adverse neurological and physical outcomes and the need for long-term health, social and educational care increases with increasing prematurity.10 46–49 If the more immature babies within this population have similar outcomes as those born at <27 weeks (regarding place of birth/care), then caring for them in LNU may be associated with worse outcomes and long-term costs. Conversely, perhaps more mature babies would do better in LNU, through the avoidance of overmedicalisation. Watson et al45 found that babies born between 27 and 32 weeks of gestation and cared for in NICU were more likely to receive ROP treatment than those born in non-NICU, although this might reflect differences in severity of illness of babies born and cared for in NICU. Even if outcomes are comparable, keeping mothers and their babies in local units could avoid unnecessary transfers and improve family-centred care. The cost to the UK NHS (National Health Service) of providing the same level of care in NICU versus LNU has not been quantified but may also be different. Therefore, grouping babies born between 27 and 31 weeks together might obscure benefits of birth/care in one type of unit over the other.
Conclusion
There is currently a paucity of evidence and data to guide the management of preterm babies born between 27 and 31 weeks of gestation with respect to place of birth or care and further research is therefore required.
Future perspective
The OptiPrem project, funded by the National Institute for Health Research - Health Systems and Delivery Research (NIHR HS&DR) Stream,50 has been designed to address the question posed by our systematic review. OptiPrem will use data from the National Neonatal Research Database, linked to Hospital Episode Statistics and national mortality statistics through NHS digital services. The project will evaluate associations between place of birth/care for babies born between 27 and 31 weeks of gestation, neonatal and infant mortality, and key neonatal morbidities, by week of gestation. Parent and staff perspectives, and costs of care will also be explored as these would be important drivers for health service change if infant health outcomes are not directly influenced by place of care.
References
Footnotes
Collaborators The OptiPrem Study Group include Elaine M Boyle, Neena Modi, Oliver Rivero-Arias, Brad Manktelow, Sarah E Seaton, Natalie Armstrong, Miaoqing Yang, Abdul Qader Tahir Ismail, Vasiliki Bountziouka, Caroline S Cupit, Alexis Paton, Victor L Banda, Elizabeth S Draper, Kelvin Dawson and Thillagavathie Pillay (Chief Investigator).
Contributors AQTI, EMB and TP developed the idea for the systematic review. AQTI conducted the literature search and prepared the initial draft of the manuscript. AQTI, EMB and TP revised the manuscript and approved the final manuscript for submission.
Funding This work is supported by the NIHR HS&DR Stream, Project number 15/70/104, and by the Royal Wolverhampton NHS Trust, Protocol number 2016NEO87. AQTI is undertaking a PhD with the University of Leicester, with funding from the OptiPrem project. He is supervised by TP and EMB.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.