Article Text

Abstract
Objective We aimed to conduct a systematic review of the available literature to determine the effects of confirmed cases of COVID-19 in pregnant women from the foetal perspective by estimation of mother to child transmission, perinatal outcome and possible teratogenicity.
Methods Data sources: eligible studies between 1 November 2019 and 10 August 2020 were retrieved from PubMed, Embase, LitCovid, Google Scholar, EBSCO MEDLINE, CENTRAL, CINAHL, MedRXiv, BioRXiv and Scopus collection databases. English language case reports, case series and cohort studies of SARS-CoV-2 confirmed pregnant women with data on perinatal outcome, congenital anomalies and mother to child transmission were analysed.
Results 38 case reports, 34 cohort and case series describing 1408 neonates were included for evidence acquisition of mother to child transmission. 29 case reports and 31 case series and cohort studies describing 1318 foetuses were included for the evaluation of perinatal outcome and congenital anomalies. A pooled proportion of 3.67% neonates had positive SARS-CoV-2 viral RNA nasopharyngeal swab results and 7.1% had positive cord blood samples. 11.7% of the placenta, 6.8% of amniotic fluid, 9.6% of faecal and rectal swabs and none of the urine samples were positive. The rate of preterm labour was 26.4% (OR=1.45, 95% CI 1.03 to 2.03 with p=0.03) and caesarean delivery (CS) was 59.9% (OR=1.54, 95% CI 1.17 to 2.03 with p=0.002). The most common neonatal symptom was breathing difficulty (1.79%). Stillbirth rate was 9.9 per 1000 total births in babies born to COVID-19 mothers.
Conclusion Chances of mother to child transmission of the SARS-CoV-2 virus is low. The perinatal outcome for the foetus is favourable. There is increased chances of CS but not preterm delivery.The stillbirth and neonatal death rates are low. There are no reported congenital anomalies in babies born to SARS CoV-2 positive mothers.
- data collection
- microbiology
- mortality
- neonatology
- virology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key message
What is known about the subject?
Studies specifically analysing all aspects of the foetus in SARS-CoV-2 positive mothers are not currently available. There are some systematic reviews reporting maternal outcomes, vertical transmission and neonatal outcomes involving a lesser number of pregnancies separately but aspects like foetal complications and teratogenicity are not adequately reported.
What this study adds?
The confirmed congenital transmission rate was found to be 9/1408 (0.63%). The risk of caesarean delivery is significantly higher in SARS-CoV-2 positive mothers but there is no significantly higher risk of prematurity. There is evidence of foetal distress, and neonatal respiratory symptoms in COVID-19 mothers but stillbirth is low.
Introduction
Novel coronavirus infection and associated coronavirus disease-2019 (COVID-19) pandemic has changed our lives forever and has compelled us to reconsider almost everything we have long taken for granted. Among the different coronaviruses severely affecting human species, Middle East respiratory syndrome coronavirus (MERS-CoV), severe acute respiratory syndrome coronavirus (SARS-CoV) and SARS-CoV-2 are significant, causing MERS, SARS and COVID-19, respectively. SARS-CoV-2 strains show significant sequence homology to SARS-CoV and MERS-CoV.1 As the pandemic evolved, there were significant advances in our knowledge about various aspects of the COVID-19 including epidemiology, clinical features, transmission, detection and management modalities. Discoveries along the process of evolution are still contributing to our management practices.
There were concerns regarding the maternal and foetal effects since the beginning of the pandemic. The earlier evidence of COVID-19 in pregnancy pointed towards pregnancy being considered as low risk for the disease and no difference in disease behaviour in pregnant and non-pregnant women was reported.2 On the contrary, a newer study involving pooled data from more than 8000 women in the USA pointed towards a significantly higher rate of intensive care unit (ICU) admission (adjusted relative risk (aRR)=1.5) and need for mechanical ventilation (aRR=1.7) in pregnant women as compared with non-pregnant women, even when adjusted for race/ethnicity and underlying comorbid conditions.3 Similar findings were reported from other studies from the USA and Sweden.4–6
However, these studies did not specify adequately foetal effects resulting from congenital or neonatal infection in SARS-CoV-2 positive mothers and consequent perinatal outcomes. Evidence of COVID-19 specifically focusing on foetal and neonatal outcomes are lacking. Most of the reported literature have smaller studies. Previous systematic reviews focusing on the outcomes of all coronaviruses have reported a higher risk of pre-eclampsia, preterm birth, miscarriage and perinatal death.
Through this article, we want to analyse the published evidence on the foetal perspective of COVID-19 infection concerning mother to child transmission (congenital or neonatal infection) and perinatal outcome through a systematic review. This will aid in alleviating uncertainties faced while doing patient counselling and help in subsequent management during these testing times.
Methods
Search strategy
A systematic search of PubMed, Embase, LitCovid, MedRxiv, BioRxiv, Google Scholar, EBSCO MEDLINE, CINAHL and Scopus electronic database was done. Medical subject handling terms (MeSH) and free-text term keywords like vertical transmission, perinatal outcome, foetal, neonate, newborn, pregnancy were used in combination with COVID-19, 2019-nCoV, SARS-CoV-2 to search for data from 1st November 2019 till 10th July 2020. Thereafter manual update was done on weekly basis till 10th August 2020. The references of relevant studies were also searched.
The keywords detail and full search strategy used in each of PubMed, Embase, LitCovid, MedRxiv, BioRxiv, Google Scholar, EBSCO MEDLINE, CINAHL and Scopus electronic database are as follows: both medical subject headings (MeSH) and keywords: “2019 novel coronavirus infection” OR “COVID-19” OR “COVID19” OR "coronavirus disease 2019” OR “nCoV infection” OR “2019-nCoV” OR “2019 novel coronavirus” OR “2019 coronavirus” OR “novel coronavirus” OR (2019 AND coronavirus) OR “SARS CoV-2” OR “SARS CoV2” AND “vertical transmission” OR “foetal outcome” OR “perinatal outcome” OR “neonatal outcome” OR “pregnancy” OR “congenital infection” OR “mother-to-child transmission” OR “(transmission AND vertical)” OR “(transmission AND fetomaternal)” OR “teratogenicity”.
Selection criteria
The search consisted of only English language articles (original English articles and other language articles with available English translation) including case reports, case series and letters to editors containing case information. After a thorough screening, no randomised clinical trials were found.
Inclusion criteria
The studies fulfilling all of the following criteria (1, 2 and 3) were included for review.
Studies reporting pregnant women with confirmed COVID-19 who had delivered.
Studies containing the results of the SARS-CoV-2 test (including reverse transcriptase-Polymerase Chain Reaction (RT-PCR) and serological tests) in both mother and newborn samples.
Studies that present the out-come of vertical transmission or congenital transmission or neonatal transmission or the perinatal outcome or congenital anomaly.
Exclusion criteria
Exclusions consisted of studies in pregnant women yet to deliver, duplicated studies, review articles, articles in languages other than English where translation was not possible, studies where infection in mothers is not confirmed, or where neonatal testing was not done. Conference abstracts, expert opinions and critical appraisals were also excluded.
Both the authors (RD, SSK) reviewed all titles independently. The potential relevance of the studies to be included for review were agreed on by discussion. Selected titles and abstracts were further screened between studies to reject overlap of cases.
Full-text copies of the selected papers were obtained and the relevant data regarding study characteristics, evidence of vertical transmission and perinatal outcomes were extracted by the same two reviewers independently. In the case of individual case reports, if the same patient was included in more than one study with similar characteristics and findings, only the report with a larger number of patients was included. As far as possible, single case reports were cross-checked with other reports from the same location and hospital. If a case series included multiple locations, the individual reports from the same centres were excluded. Similarly, if the time-frame of the reported cases matched from the same centre, the characteristics were compared to decide regarding the inclusion or exclusion from the study. Finally, studies were screened by assessing selection, comparability and exposure for inclusion into evidence acquisition of mother to child transmission (congenital or neonatal transmission) and/or perinatal outcome measures (online supplementary tables 1A,B).
Supplemental material
Study outcomes
Mother to child transmission
Evidence of mother to child transmission (congenital or neonatal transmission) is indicated by positive RT-PCR status in different samples like the neonatal nasopharyngeal swab, cord blood, amniotic fluid, breast milk and placental tissue. Transmission of infection from mother to foetus generally includes transmission through germ cells or the placenta during pregnancy, via the birth canal during labour and delivery, and the postpartum period through breast feeding or close contact. The transfer of micro-organisms during pregnancy is seen with many of the common pathogens with resultant effects ranging from asymptomatic infection, intrauterine growth restriction (IUGR), intrauterine death and structural anomalies as a sequel of infection. Some pathogens like cytomegalovirus or Zika virus produce mild to no symptoms in the pregnant patient but can cause congenital infection with severe consequences.7 Viruses specifically can be transmitted to the foetus via the maternal blood when it enters the placental villus, containing the foetal blood vessels or by direct access to the placenta from the lower genital tract by ascending infection.8 Again even when transferred trans-placentally during the antenatal period, the specific timing of maternal infection can have different effects on the foetus. The first-trimester infection can cause severe structural anomalies whereas second and third-trimester infections are more likely to cause functional organ abnormalities.9
Several factors are contributing to the concerns of mother to child transmission in COVID-19. It is known that the SARS-CoV-2 uses Angiotensin converting enzyme-2 (ACE-2) receptors for entry into the cells. ACE-2 receptors are detected in various parts of the uterus, vagina, decidual cells and placenta.10–13 Recently, the case definition for SARS‐CoV‐2 infection in pregnant women, foetuses and neonates has been published with a categorisation of infection into confirmed, probable, possible, unlikely and not infected groups.14
Congenital infection with intrauterine foetal death (IUFD)/stillbirth is14:
Confirmed from foetal tissue or autopsy material if the virus is detected by PCR from foetal or placental tissue or electron microscopic detection of the viral particle in tissue or viral growth in culture from foetal or placental tissue.
A probable infection if the virus is detected by PCR in the surface swab from the foetus or placental swab on the foetal side.
Unlikely if it is positive in the maternal side of the placenta but foetal tissues are not tested and not present if it is not detected in foetal tissue in an autopsy.
Similarly, congenital infection in live-born symptomatic neonate is14:
Confirmed when the virus is detected by PCR in umbilical cord blood or neonatal blood collected within the first 12 hours of birth or amniotic fluid collected prior to the rupture of the membrane.
A probable infection when there is the detection of the virus by PCR in nasopharyngeal swab at birth (collected after cleaning baby) AND placental swab from the foetal side of the placenta in a neonate born via caesarean section (CS) before rupture of membrane or placental tissue.
Possible when there are anti-SARS-CoV-2 IgM antibodies in umbilical cord blood or neonatal blood collected within the first 12 hours of birth or placental tissue but nasopharyngeal swab test at birth is negative.
Unlikely or absent when samples are negative within 12 hours of birth (nasopharyngeal swab, umbilical cord blood or neonatal blood) and antibody testing is not done or negative, respectively.
If a live-born neonate has no clinical features of infection, congenital infection is14:
Confirmed by detection of the virus by PCR in cord blood or neonatal blood collected within the first 12 hours of birth.
Probable if the virus is detected by PCR in amniotic fluid collected prior to rupture of the membrane but no detection in umbilical cord blood or neonatal blood collected within the first 12 hours of birth.
Possible when there is anti-SARS-CoV-2 IgM in umbilical cord blood or detection of the virus by PCR in placental tissue but PCR in umbilical cord blood, amniotic fluid and neonatal blood (<12 hours of life) is negative.
Furthermore, infection acquired intrapartum in a symptomatic neonate is confirmed if the virus is detected by PCR in nasopharyngeal swab at birth (collected after cleaning the baby) AND at 24–48 hours of age AND alternate explanation for clinical features excluded.14
Intrapartum neonatal infection in asymptomatic neonate is confirmed by detection of the virus by PCR in nasopharyngeal swab at birth (collected after cleaning the baby) AND at 24–48 hours of age.14
Postpartum infection is confirmed if a neonate shows symptoms beyond 48 hours of life and the nasopharyngeal swab is positive beyond 48 hours which was negative at birth.14
If a neonate is born with a specific structural sequel of an infection, intrauterine infection is a probability. The probability of infection also depends on the presence of the agent in the genital tract and time taken from exposure to detection by definitive tests to differentiate between intrapartum and postpartum infection. Furthermore, the sensitivity of RT-PCR testing is different for detecting SARS-CoV-2 in different samples. Therefore, it is rational to test samples from multiple sites to improve detection and reduce false-negative cases.9 15
Perinatal outcome
Perinatal outcome measures included foetal outcomes like foetal complications in SARS-CoV-2 positive pregnant women, gestational age at delivery (preterm delivery), mode of delivery, birth weight and stillbirth. The neonatal period is defined as the time period from birth until the end of the first 28 days of life. Events in the early neonatal period (first 7 days) usually are related to the pregnancy more significantly and it is also included in the definition of the perinatal period. In this review, we have assessed the neonatal outcomes using the APGAR score at 1 min and 5 min of life, neonatal symptoms, admission into neonatal ICU, and neonatal death, as the parameters. An APGAR score of less than 7 at 1 min and 5 min after birth in a newborn is defined as a low APGAR score in this study.16 Any outcome measures not explicitly mentioned were considered not to have been reported.
Foetal distress (FD) is assessed during labour by non-reassuring or pathological cardiotocographic (CTG) findings and meconium-stained amniotic fluid.17 18 For this research, studies reporting FD, abnormal or non-reassuring or pathological CTG, foetal compromise, meconium-stained amniotic fluid are included under FD. Other foetal complications were prelabour rupture of membranes and preterm prelabour rupture of membranes.
Preterm delivery is defined as delivery of a viable product of conception before 37 completed weeks of gestation.
Delivery can be vaginal delivery (including instrumental) and by CS. For this research, instrumental vaginal deliveries (VDs) and normal VDs were considered together.
Both the Royal College of Obstetrics and Gynecology and the American College of Obstetricians and Gynecologists have adopted the definition of IUGR as an estimated foetal weight less than 10 percentile. The term IUGR has been used interchangeably with small for gestational age (SGA). SGA is a term commonly used for a neonate with birth weight less than 10th centile.19 20
For this research, stillbirth was considered as foetal death beyond 24 weeks of gestation, and stillbirth rate (SBR) is calculated as the number of stillbirths per 1000 total births.
Statistical analysis
Pooled proportions of categorical variables were calculated with percentage after obtaining the positive rates of each of the SARS-CoV-2 testing methods used, wherever applicable. Odds Ratio (OR) was calculated for the foetal outcome of preterm delivery and mode of delivery in the SARS-CoV-2 positive mothers from the pooled data (combining the studies where the control group of SARS-CoV-2 negative pregnant women was available) with 95% CI and p values. The percentage of the most common variables were also calculated.
Public and patient involvement statement
This research is not ‘coproduced’ with patients, carers or members of the public.
Results
Mother to child transmission
Search results
Out of 100 records selected for full-text review, 3 Chinese, 1 Italian, 1 Dutch and 1 Spanish studies were excluded due to non-availability of English translation. 72 studies fulfilled the eligibility criteria and were included in the qualitative synthesis. 38 studies were case reports containing 4 or fewer number of cases and 34 studies had 5 or more number of patients (figure 1).
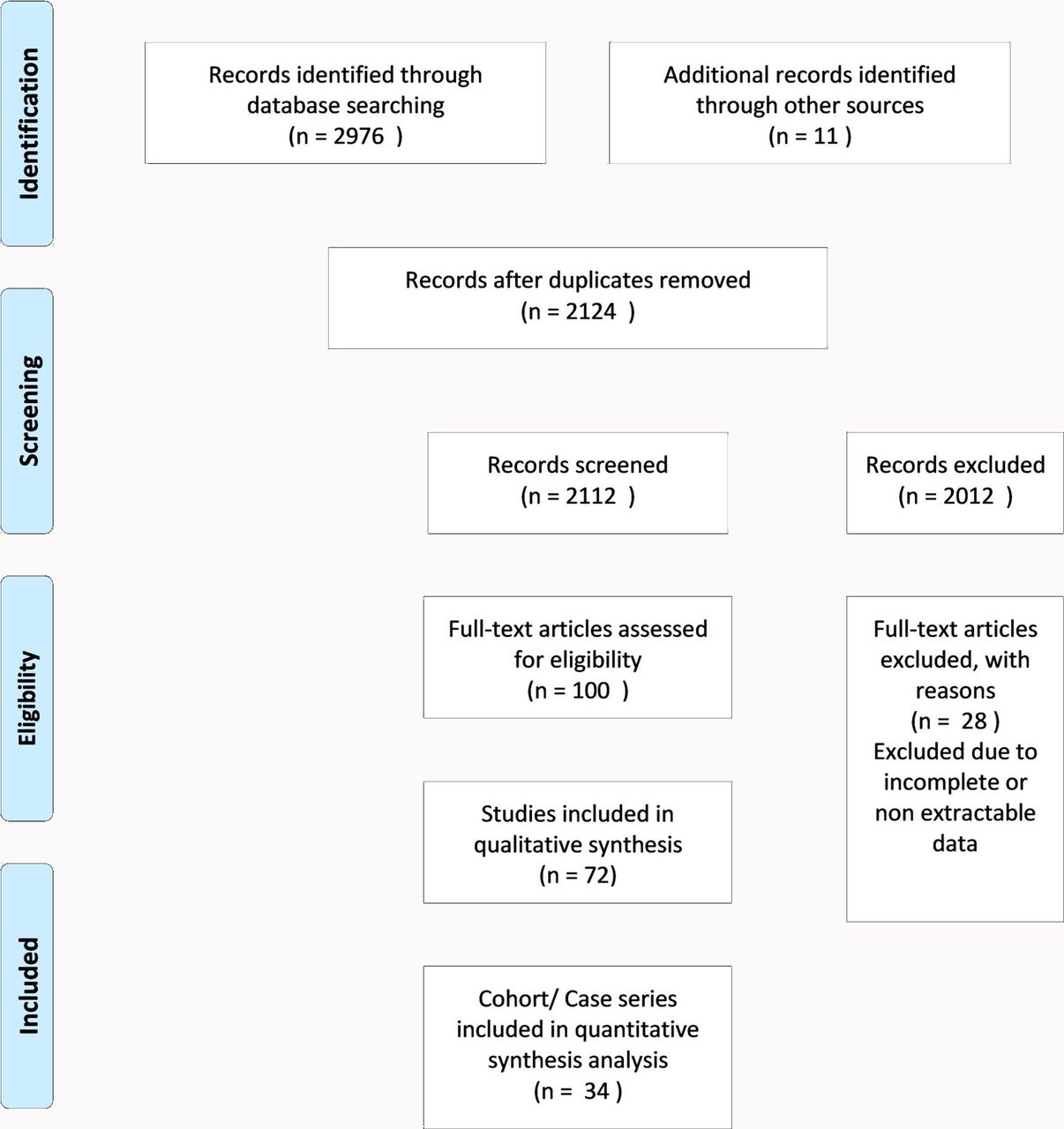
Image-PRISMA-1-Mother to child transmission.
Since evidence from randomised control trials were not available until the time of the search, 34 studies having 5 or more number of patients were considered for qualitative analysis.21 22 However, the findings from the case reports were also noted. The majority of earlier studies were from China but later studies contained cases from the rest of the world (online supplementary tables 1A,B).
Systematic review
Tests for diagnosis of SARS-CoV-2 were done in a total of 1408 neonates. The most common type of sample tested was neonatal nasopharyngeal samples (NP swab) (67 out of 72 studies) followed by the placenta, amniotic fluid and cord blood. In the majority, samples were taken from more than one site. In a few studies, the same type of sample was repeated at different intervals (eg, NP swab and breast milk samples) (table 1).
Studies and type of samples
Neonatal nasopharyngeal swab
In our review, a total of 1388 neonates born to mothers with COVID-19 infection were tested by NP swabs. 51 neonates were found positive by the RT-PCR test constituting 3.67% of total pooled samples (table 2a).
Mother to child transmission-test positive (pooled result)
The largest cohort study from the UK involved 427 pregnant women with COVID-19. 244 out of the 262 neonates were tested by NP swab. Six of the neonates were positive for SARS-CoV-2 within 12 hours of birth and six more were positive after 12 hours of birth (12 out of 244; 4.9%).23 Studies involving 181 women and 116 women in China showed two positive neonates out of 181 (2 out of 181; 1.1%) in the first study and no positive cases for SARS-CoV-2 in the other study.24 25 An analysis of 141 women from a hospital in India showed that 3 of the 131 neonates were tested positive for SARS-CoV-2 by NP swab.26 In another study in a New York Hospital, 48 neonates born to 55 women were all tested negative on day 0 of life. 27 However, one Italian study found three infants positive by NP swab out of 42 tested within 48 hours after birth.28
One recent case report revealed that RT-PCR was positive for SARS-CoV-2 in all of the samples for amniotic fluid, vaginal swab, blood and non-bronchoscopic bronchoalveolar lavage fluid as well as NP swab and rectal swabs collected at 1 hour of life, and then repeated at 3 days and 18 days suggesting a trans-placental transmission.29
As stated earlier NP swab positivity at different neonatal ages plays an important role in confirming or ruling out the viral transmission from a SARS-CoV-2 positive mother.
On further analysis of the positive samples, the congenital infection was confirmed in five live-born neonates, possible in five neonates and probable in two neonates. Neonatal infection acquired intra partum was confirmed in two neonates, probable in five neonates and possible in 14 neonates. Similarly, neonatal infection acquired post partum was confirmed in seven neonates and infection was unlikely in one neonate (table 2b).
Analysis of evidence of congenital/ intrapartum/postpartum transmission
However, in a larger study, out of 12 neonates with positive NP result (six within 12 hours of life and six at more than 12 hours of life), further analysis was not possible due to lack of follow-up swab results and unavailability of test results of other maternal samples like placenta and amniotic fluid. 23
Amniotic fluid
In our review, 58 samples of amniotic fluid were tested in 19 studies with a positive result in four samples.29–31 Congenital infection is confirmed in two of the studies in live-born neonates . 29 30 Congenital infection is also confirmed in a dichorionic, diamniotic (DCDA) twin expelled at 24 weeks by positive amniotic fluid result. 31
Placenta
A total of 22 studies were identified in our review where the placenta was examined for the presence of SARS-CoV-2 or related pathological changes. A total of 111 placental samples were tested and 13 were found positive for SARS-CoV-2. PCR for SARS-CoV-2 RNA was positive from the placenta in two case reports where there were spontaneous miscarriage and dilatation and curettage, respectively confirming a congenital infection. 32 33 In one of them, the umbilical cord was also positive for the virus, but the foetal organs were tested negative. The virus was confirmed to be localised mostly in the syncytiotrophoblastic cells of the placenta by immunohistochemistry for the SARS-CoV-2 spike protein as well as electron microscopy and it was identical to the typically locally isolated virus. 32 In another study, electron microscopy showed the presence of the virus in the foetal side of the placenta. The virions were present in the mesenchymal core of the terminal villus and were demonstrated to be invading a syncytiotrophoblast and a microvillus. However, the neonate delivered at 28 weeks in this pregnancy was tested negative for the virus. 34
Evidence of probable mother to child transmission was obtained in another case where the newborn was found positive for the virus by nasopharyngeal swab, plasma and stool samples along with the placenta. 35 Similarly, confirmed congenital transmission of the virus was demonstrated by another study where SARS-CoV-2 was detected in amniotic fluid aspirated before the rupture of the membranes, vaginal swab, neonatal blood, bronchoalveolar lavage fluid and neonatal swabs on repeated occasions at 1 hour, 3rd day and 18th day of life. The trophoblastic cells showed SARS-CoV-2 N protein on immunostaining. 29
Placental pathological examination showed an array of changes including vascular malperfusion, fibrin deposition, and chronic villitis, intervillositis, and villous infarctions in our review. Two of these studies showed vascular malperfusion in 10 out of 20 placentas and 12 out of 15 placentas, respectively but there were no assessments of placentas in these studies for the presence of SARS-CoV-2 infection. However, neonatal swabs were negative for the virus.36 37 Similar pathological changes were seen in another study involving five SARS-CoV-2 positive pregnant women but the placentas were negative for the virus on direct testing for SARS-CoV-2.38 Chronic intervillositis was also seen in the pathological examination of the placentas of two women where the neonates were positive for SARS-CoV-2 by nasopharyngeal swab testing.39 Examination showed severe chronic villitis in another case where there was a stillbirth at term but direct tests of foetal tissues and placenta did not show infection with the virus.40
Other samples
Various other samples were tested for SARS-CoV-2 by different studies. Anal swab, rectal swab or faecal sample was positive in 9.6% of neonates in our study. The stool sample was positive in two of the studies on day 2 and day 7 of life.35 41 The urine sample was tested in only three studies without any positive results.42–44 Breast milk was tested by RT-PCR in 10 of the studies with a pooled positive rate of 5.3% (3 out of 56).35 45–53 In one of the studies, the breast milk sample was positive in four consecutive days coinciding with the maternal symptoms in one woman but it was negative in milk samples of another woman. Both the babies were positive by the nasopharyngeal swab test and were symptomatic.52 A vaginal swab was tested in 23 women with one positive result (4.3%).29 Since IgM cannot cross the placenta, elevated IgM levels in the neonate indicate possible congenital infection, as seen in some of the neonates in this review.54 55 However, the assay of IgM for the detection of infection has significant false-positive results.
Perinatal outcome
Search results
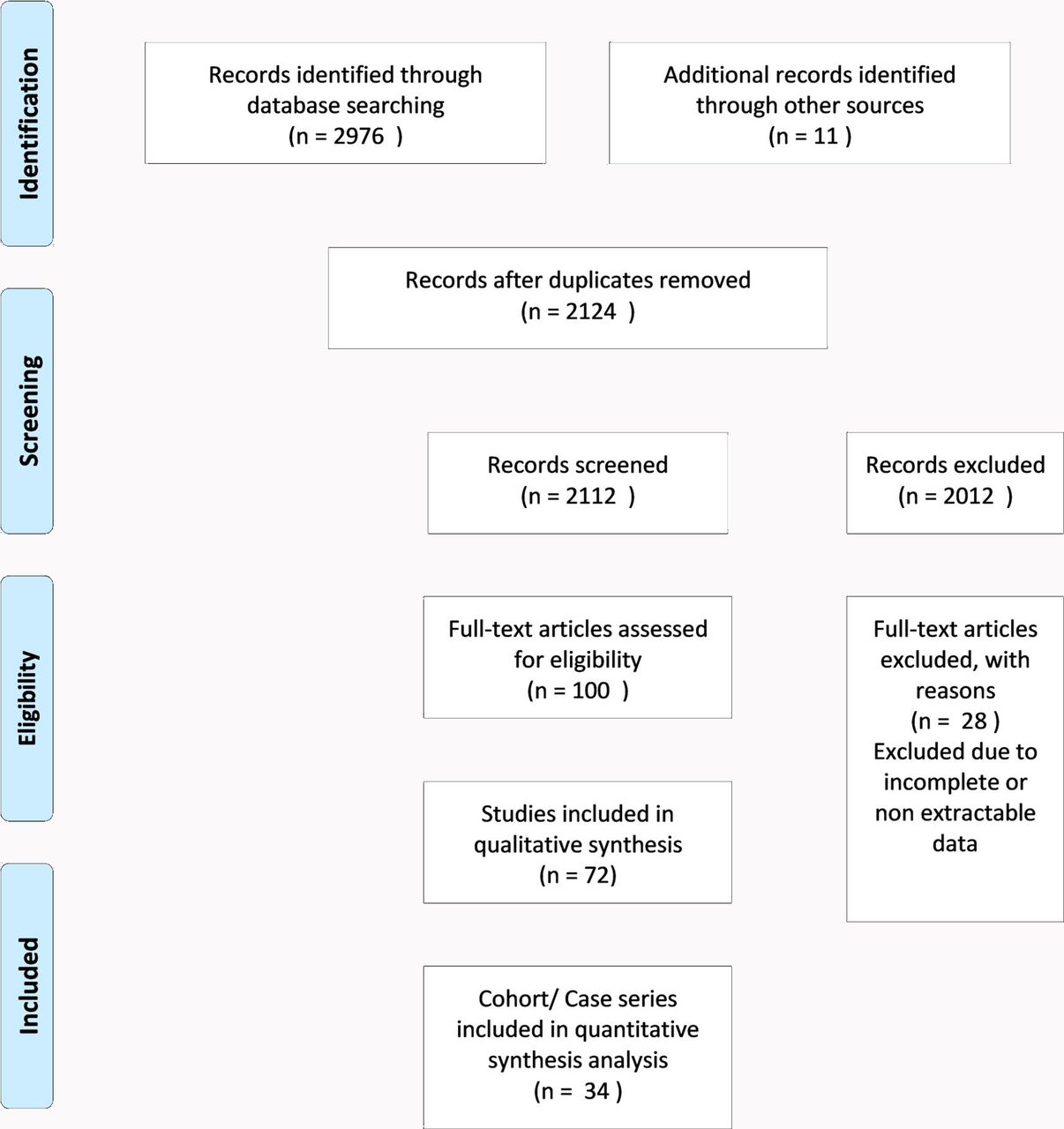
Out of 73 records selected for full-text review, 1 Chinese and 1 Spanish study were excluded due to unavailability of English translation. A total of 60 studies fulfilled the eligibility criteria and were included in the qualitative synthesis. Thirty-one studies qualified as case series/cohort and 29 studies contained four or fewer cases in our review (figure 2). No randomised control trials were available until the time of the search.

{kind=link}
{kind=link}
Image-PRISMA-2-Perinatal outcome.
Systematic review
Foetal outcomes
Foetal complications in SARS-CoV-2 positive pregnant women
In our review, a total of 30 studies reported any foetal effects excluding all pregnancy losses or IUFDs (table 3). The most commonly reported effect was foetal distress in 36 out of 1311 pregnancies (2.74%). In addition to foetal distress, some studies have reported non-reassuring or pathological cardiotocography (CTG) (11 out of 1311; 0.83 %), and some have mentioned meconium-stained amniotic fluid (3 out of 1311; 0.22%), both findings can also be considered as evidence of foetal distress.29 56–62 In another study involving 262 deliveries, the foetal compromise was seen in 37 foetuses and an emergency CS was done in 9 of them. 23 Thus, the cumulative chance of foetal distress in pregnant women with a positive test for SARS-CoV-2 is 6.63%.
Foetal outcome
Premature rupture of membrane (PROM) was reported in 42 pregnancies from 13 studies and Preterm PROM (PPROM) was reported in 14 pregnancies.24 41 42 45 50 57 60 63–70 IUGR was reported in 12 foetuses in five studies.24 63 65 71 72 The highest number of IUGR foetuses was reported in 6 out of 10 foetuses in another study.71 Besides, SGA was reported in another study in 2 out of 10 foetuses.57 Chorioamnionitis was reported only in one study involving three foetuses.5
Mode of delivery
Mode of delivery was available for a total of 1311 out of which 8 were twin pregnancies. 761 (60%) were delivered by CS and 506 (40%) by VD out of 1267 pregnancies from case series. In case reports, out of 44 deliveries, 25 were CS (56.8%) and 19 (43.2%) were VD bringing the percentage of CS to 59.9% and VD to 40.1% in the pooled data (table 4). Few studies in our data compared the CS in the SARS-CoV-2 positive pregnant women to negative controls comprising of 122 CS in the positive group out of 233 and 650 CS in the control group out of 1562 in the pooled data. OR for CS in SARS-CoV-2 positive mothers is 1.5421 (95% CI 1.1701 to 2.0324) and p=0.0021 which is statistically significant.26 60 66 73
Perinatal outcome (pooled data)
CS was the only mode of delivery in the majority of early published case reports as in the early days of the pandemic, elective CS delivery was the mode preferred by most of the countries for maternal indications.29 30 35 44 45 48 49 51 54 55 64 74–84 As the pandemic progressed, favourable outcomes were reported from vaginal delivery by many studies.50 62 72 85–87 It was also demonstrated that the chances of the virus being present in the vaginal fluid is very remote. In the later and larger case series, CS deliveries were only done for obstetrical indications.26 In a study involving 134 deliveries, there were 67 CS and 67 VDs. The rate of CS was not statistically different in women with positive SARS-CoV-2 as compared with negative pregnancies.26 In yet another study, there were significantly higher rates of CS deliveries in cases (14 out of 16) as compared with the control group (57 out of 121) (p<0.001) but there was no difference in the groups with regards to chronic illnesses or pregnancy complications.66 However, when done for maternal COVID-19 indications, the rate of caesarean was found to increase with the severity of the disease.25 In another study, out of 41 CS deliveries, 12 were for COVID-19 symptoms without other obstetrical indications (four with severe symptoms and eight with mild/moderate symptoms).65
In the largest study in the UK, the CS delivery was seen in 156 women and vaginal birth was seen in 106 women from a total of 262 births. The indications of CS were maternal compromise (27%), foetal compromise (24%), failed induction of labour or failure to progress (19%), other obstetric reasons (16%), prior CS (10%) and maternal request (4%).23 Maternal COVID-19 related conditions were predominant indications in another larger study reporting CS for COVID-19 pneumonia in (33 out of 85), previous CS (16 out of 85), foetal distress (9 out of 85) and failure to progress in 5 out of 85 patients.24 Many other studies similarly reported maternal condition requiring delivery as the most common indication for CS.25 28 81
Preterm delivery
In our study, the outcome of preterm delivery was reported in a total of 43 studies involving 1318 foetuses out of which 330 out of 1273 neonates in the case series and cohort (25.9%) and 19 out of 45 neonates in the case reports (42.2%) were delivered preterm. The pooled preterm birth was seen in 26.4% of total births (table 4). However, the majority of them were elective deliveries to improve maternal respiratory conditions related to COVID-19. Spontaneous preterm delivery was only seen in 1.8% of neonates. The other indications included the preterm prelabour rupture of membranes. In a substantial number of studies, data regarding the indications were not found. Few studies in our data compared the preterm delivery in the SARS-CoV-2 positive pregnant women to negative controls comprising 52 preterm deliveries in the positive group out of 220 and 267 preterm deliveries in the control group out of 1520 in the pooled data. OR for preterm delivery in SARS-CoV-2 positive mothers is 1.4526 (95% CI 1.0360 to 2.0366) and p=0.0304.26 60 66
In a study involving 134 deliveries in COVID-19 patients, preterm delivery was reported in 38 pregnancies with positive SARS-CoV-2 and 239 out of 836 SARS-CoV-2 negative deliveries, which was not significantly different.26 A similar report was seen in another study where 4 preterm deliveries were seen out of 17 SARS-CoV-2 confirmed group as compared with 7 out of 121 in the control group.66 In another study, out of a total of 25 preterm deliveries, iatrogenic preterm delivery was done in 12 and 13 were spontaneous preterm deliveries.65
Furthermore, comparing the outcomes of COVID-19 pregnancies with different disease severity involving 181 pregnant women, preterm delivery was seen in 13 out of 123 (10.6%), 14 out of 29 (48.3%) and 23 out of 29 (79.3%) in women with non-severe, oxygen-requiring and critical COVID-19, respectively. Delivery before 32 weeks was highest in 48.3% of women in the critical COVID-19 group. In severe disease, urgent delivery is required to stabilise the maternal condition, even when it results in iatrogenic preterm delivery.25
Birth weight
In our review, birth weight was missing in many studies and only the mean weight of the babies was mentioned in some of the series. IUGR was reported in 4 studies in 11 babies.24 63 71 72 Also, SGA was found in two studies in five babies.41 57 A maximum of six babies had IUGR in one study but they were described as mild.71
Miscarriage and stillbirth
Stillbirth was seen in 13 foetuses in 8 studies in our review and seven were second-trimester miscarriages23 25 26 31 40 60 69 75 (table 4). Three intrauterine deaths were observed in one of the studies which reported maternal deaths due to COVID-19.75 Similarly, we found 15 spontaneous miscarriages, and 4 induced miscarriages reported in 5 studies.23 25 26 46 68 Induced miscarriages were done on maternal request in both studies.46 68 Among the spontaneous miscarriages, 6 were seen in 141 pregnancies in one study and 5 in 181 pregnancies in another study.25 26 In one of the studies, there were three stillbirths. However, the causes of these three stillbirths reported, were not related to COVID-19 in the mother.23
Neonatal outcomes
Neonatal symptoms
The most common neonatal symptoms were respiratory problems reported as respiratory distress, shortness of breath, respiratory difficulty, dyspnoea and breathing problems.28 41 52 57–59 65 70 76 78 81 82 84 Respiratory distress was the most common symptom reported in 14 neonates but the test for SARS-CoV-2 was positive in only 4 neonates and negative in 8.28 41 59 65 81 82 84 Pneumonia was seen in five neonates who were positive for SARS-CoV-2 and four neonates who were negative.41 48 61 64 75 Although usually respiratory symptoms are seen more in preterm babies due to pulmonary immaturity, in a single case report there were no neonatal complications in a SARS-CoV-2 positive mother who delivered a preterm baby at 29 weeks 5 days by emergency CS for maternal indications.88
Diffuse bilateral granular and hazy opacities in chest radiograph and thickened lungs on X-ray were found in two neonates but the neonatal test for SARS-CoV-2 was negative in both of them.51 84 In another SARS-CoV-2 positive, newborn chest X-ray was consistent with pulmonary infection, 53 hours after birth.68 In another study, neonatal symptoms are extensively described. The most common first clinical symptom in the neonates of SARS-CoV-2 positive women was shortness of breath (n=6), followed by gastrointestinal symptoms like feeding intolerance, bloating, refusing milk and gastric bleeding (n=4). Other symptoms included fever, rapid heart rate and vomiting. Chest radiographic abnormalities included infections (n=4), neonatal respiratory distress syndrome (n=2) and pneumothorax (n=1). Another preterm baby suffered from frequent oxygenation fluctuations and thrombocytopenia and was cured 15 days later.57 It was reported in yet another study that most of the complications in neonates were a result of prematurity (often iatrogenic) rather than SARS-CoV-2 infection. 41 Other presentations in SARS-CoV-2 positive neonates included fever, cyanosis, lethargy, irritability, poor feeding, axial hypertonia, opisthotonus and feeding difficulties.29 39 41
APGAR score
In our review, a total of nine studies have reported a low APGAR score among babies born to SARS-CoV-2 positive mothers.26 28 29 41 61 78 82–84 Seven of the neonates were very preterm or preterm and were SARS-CoV-2 negative. The APGAR score in these is likely to be due to pulmonary immaturity.26 28 29 78 82–84 Two other babies were term deliveries and tested positive for SARS-CoV-2 .41 61 However, another study reported low APGAR scores of 0–3 in 2 babies of COVID-19 positive mothers and 15 babies in COVID-19 negative mothers, indicating no statistically significant difference.26
ICU admissions
Admission to the neonatal ICU was done for various reasons. The majority of admissions were for observation and isolation. Neonates admitted due to complications of prematurity constitute another higher portion of the neonates. In a study, out of a total of 24 ICU admissions, it was found that 16 babies were admitted due to low birth weight, 2 for low APGAR score and 6 others for other uncommon reasons like ABO blood group incompatibility.26 In another study, it was found that rates of admission to ICU increased with the severity of the disease in the mother.25 In our review, ICU admissions for suspected or confirmed neonatal sepsis was reported in six neonates out of which enterobacter and respiratory syncytial virus was found in two neonates. The culture was negative for four others.35 41 51 52 59 70
Neonatal death
Neonatal death was reported among seven neonates in five studies.23–25 57 75 It was unclear whether COVID-19 in mothers contributed to the deaths in two neonates in one of the studies.23 In another study, neonatal death occurred in a preterm baby on the ninth day of life who was admitted with shortness of breath and moaning and later developed refractory shock, multiple organ failure and disseminated intravascular coagulation.57 The calculated neonatal death rate is 5.47 per 1000 live births (table 5).
Neonatal outcome
Congenital anomaly
We could not find any studies describing structural anomalies in the foetus associated with COVID-19. Due to an evolving pandemic, the teratogenicity of the virus has not yet been explored adequately. However, in few of the studies, the findings of anomaly scans during pregnancy were included and they did not show any difference between foetuses of SARS-CoV-2 positive and negative women. 46 57 In two case reports, a multicystic dysplastic kidney was detected by antenatal ultrasound in one and after delivery in the other. 36 59 In another study bilateral gliosis of the deep white periventricular and subcortical matter was detected in an 11 days old neonate born to SARS-CoV-2 positive mother by MRI. 29 However, these cannot be attributed to SARS-CoV-2. Furthermore, autopsy finding in a stillborn baby born to COVID-19 mother did not show any abnormality in another report. 40
Discussion and conclusion
We wanted to analyse the published evidence on the foetal perspective of COVID-19 infection concerning mother to child transmission, perinatal outcome and congenital anomalies through a systematic review.
The present available data do not provide a clear conclusion into the foetal outcomes and its clinical implications. Few other reviews have explored the evidence of vertical transmission. There is varied positivity rate of different samples. The positivity of NP swab in this study is 3.67% which is in accordance with other reviews reporting 3.2% (22/936), 2% (9/493) and 3.48% (3/86), respectively. 89–91 In a couple of other reviews, however, the NP samples were negative ((0/113) and (0/9)). 92 93 No evidence of vertical transmission was found in other reviews. 2 94 95
The placental sample was positive in our review in 11.7% of pregnancies. It is similar to the review by Kotlyar et al reporting 9.7% (3/31) sample positivity.89 The placenta was extensively studied in another review where it was shown that there is a low likelihood of placental infection and vertical transmission of SARS-CoV-2 since the receptors and proteases, are only minimally expressed by the human placenta throughout pregnancy.96 Placenta was also negative for 54 samples in another review.90
Amniotic fluid collected before the rupture of membranes was positive in 6.8% of pregnancies in our review, in contrast to the review by Kotlyar et al (0/51) and Ashraf et al (1/16). 89 91
The serological analysis was found in some studies within our review showing IgM positive results at birth indicating possible congenital transmission. Using the criteria by Shah et al, we found that there is confirmed congenital transmission in five live-born neonates and two DCDA twins expelled at 24 weeks.14. Similarly, the possible congenital transmission was found in five neonates and probable in two neonates. These analyses were not reported in earlier reviews involving more than 1300 pregnancies in total.
The chance for CS is more in women with COVID-19 and in most instances for maternal indications. Preterm delivery is also high (26.4%) most commonly due to adverse maternal condition, although spontaneous preterm labour is low (1.8%). This is in accordance with another systematic review with regards to the indication but they found a trend towards spontaneous preterm labour. 97 In contrast, an earlier review reported 6.4% of preterm deliveries as spontaneous. 98
FD (6.63%) was the most common complication seen in the foetus followed by PROM and PPROM (4.27%) in our review. Similar findings were seen in other reviews. 91 94 One earlier review did not report any foetal complications. 92 PPROM was reported in 14 pregnancies in our review. While PROM and PPROM are unlikely to contribute to mother to child transmission as the SARS-CoV-2 has not been positive in the vaginal swab, PPROM is a significant cause of preterm labour. Through our review, it was not possible to ascertain whether COVID-19 in mothers increases the risk for PROM. IUGR was reported in 12 foetuses in 5 studies (0.9%). IUGR can be multifactorial and need to be analysed with the presence of maternal risk factors. SARS-CoV-2 has not been associated with IUGR and it was not possible to ascertain whether COVID-19 in mother increases the risk for IUGR in our study.
The rates of stillbirth and neonatal death in our study were 9.9 and 5.46, respectively. In another study, it was found that stillbirth was significantly higher during the pandemic compared with the non-pandemic period due to reasons non-associated with COVID-19 (difference, 6.93 (95% CI 1.83 to 12.0) per 1000 births; p=0.01). 99 So it is unlikely that the stillbirth and neonatal death rate are increased in COVID-19 mothers. The symptoms when present in the infected neonates were most often mild and neonatal outcomes were found to be good. 100 101 There is no reported teratogenicity or congenital anomalies associated with SARS-CoV-2 infection. Although maternal parameters were reported in previous studies,maternal outcomes were not included in our review.102–115
The outcome so far is favourable for the foetus despite the risks to the mother for ICU admissions and mechanical ventilation seen in other studies. 3 116 There is no significant increase in preterm birth but there is a significantly increased risk of CS in mothers with COVID-19.
Though the foetal perspective seems good in the case of maternal COVID-19, it will be reasonable to consider these findings with caution. Prospective studies and randomised control trials were missing from the evidence due to the recent nature of the infection. Therefore, larger and better quality studies are required to address the knowledge gaps and to reach at a definite guideline for management.
There are many strengths to this study. The studies included in the review contained only confirmed maternal cases by RT-PCR and not the suspected cases or clinically diagnosed cases. The studies contained the results of neonatal testing. Studies included in this review were from countries across the world and not restricted to a specific region, making the findings from the study globally applicable. The case series/cohorts were chosen only when the total number of cases was more than four. Moreover, various aspects of vertical transmission as well as foetal and neonatal outcomes were analysed from the chosen studies.
Nonetheless, there are many limitations to our study. Only a limited number of available case series and cohorts were included in this review as high-quality evidence involving a higher number of subjects is lacking dues to the new kind of infection and still evolving nature of the pandemic. In our review, studies in languages other than English were excluded due to unavailability of English translation. Almost all of the reports are retrospective reviews showing incomplete data with significant heterogeneity within the included studies with a chance of selection or recall bias. Different types of samples were used for the diagnosis of SARS-CoV-2 in different studies. Though nasopharyngeal swab was used for diagnosis in most studies, there were different types of kits used. Again the same kit may have different sensitivity and specificity in different types of samples. Universal testing of pregnant women was not done in many studies, resulting in missing foetal and perinatal effects in asymptomatic women. As maternal outcomes were not studied, the effects of the severity of maternal disease on the foetal outcomes could not be looked into.
Future implications
Whether there is an intrauterine infection of the foetus with respect to SARS-CoV-2 needs to be studied. What are the effects of intrauterine infection, whether there is different susceptibility at different stages of pregnancy, and whether susceptibility depends on disease severity in the mother, needs to be explored. Follow-up studies are required to see long-term effects of neonatal infection with SARS-CoV-2.
References
Footnotes
Collaborators NA.
Contributors Conception and design of the study: RD, SSK. Acquisition of data: SSK, RD. Analysis and/or interpretation of data: SSK, RD. Drafting the manuscript: RD, SSK. Revising the manuscript critically for important intellectual content: RD, SSK. Approval of the version of the manuscript to be published (the names of all authors must be listed): SSK, RD.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.