Article Text

Abstract
Objectives To determine a 10-year trend of survival, morbidities and care practices, and predictors of in-hospital mortality in very preterm neonates (VPTN, gestation 22 to <32 weeks) in the Malaysian National Neonatal Registry.
Design Retrospective cohort study.
Setting 43 Malaysian neonatal intensive care units.
Patients 29 010 VPTN (without major malformations) admitted between 1 January 2009 and 31 December 2018.
Main outcome measures Care practices, survival, admission hypothermia (AH, <36.5°C), late-onset sepsis (LOS), pneumothorax, necrotising enterocolitis grade 2 or 3 (NEC), severe intraventricular haemorrhage (sIVH, grade 3 or 4) and bronchopulmonary dysplasia (BPD).
Results During this 10-year period, there was increased use of antenatal steroid (ANS), lower segment caesarean section (LSCS) and early continuous positive airway pressure (eCPAP); but decreased use of surfactant therapy. Survival had increased from 72% to -83.9%. The following morbidities had decreased: LOS (from 27.9% to 7.1%), pneumothorax (from 6.0% to 2.7%), NEC (from 8.1% to 4.7%) and sIVH (from 12.2% to 7.5%). However, moderately severe AH (32.0°C–35.9°C) and BPD had increased. Multiple logistic regression analyses showed that lower birth weight, no ANS, no LSCS, admission to neonatal intensive care unit with <100 VPTN admissions/year, no surfactant therapy, no eCPAP, moderate and severe AH, LOS, pneumothorax, NEC and sIVH were significant predictors of mortality.
Conclusion Survival and major morbidities had improved modestly. Failure to use ANS, LSCS, eCPAP and surfactant therapy, and failure to prevent AH and LOS increased risk of mortality.
- neonatology
- epidemiology
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplemental information. The data are obtained from the database of the Malaysian National Neonatal Registry.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Trends of survival of very preterm neonates have been reported from high-income countries.
In-hospital mortality in most high-income countries is below 10%.
Late-onset sepsis remains a significant predictor of mortality in very preterm neonates in high-income countries.
What this study adds?
A 10-year trend of survival of very preterm neonates from a middle-income country national neonatal network.
Survival of very preterm neonates in this network shows similar trend in improvement as in high-income countries.
Use of antenatal steroids, early continuous positive airway pressure, prevention of admission hypothermia and prevention of late-onset sepsis are the low-cost modifiable care practices which have been identified to improve survival of very preterm neonates in middle-income countries.
Introduction
In recent decades, neonatal networks in high-income countries (HICs) reported improved trends in early outcome of very preterm neonates (VPTN, <32 weeks’ gestation) in their neonatal intensive care units (NICUs).1–7 Report of such trends are lacking in low-income and middle-income countries (LMICs).
In Malaysia, healthcare is provided mainly by a government-funded universal healthcare system, and to a lesser extent by a private healthcare system. Government healthcare centres are located all over Malaysia providing services in antenatal and postnatal care, childhood immunisation and treatment of common illnesses to Malaysian citizens at nominal charges. Public hospitals are sited in all states providing nominally charged emergency and in-hospital care, including NICU services, to Malaysians. The main drawbacks of government healthcare facilities are overcrowdedness, and longer waiting times than private healthcare system. However, when there is a high-risk delivery such as preterm birth, government NICUs are the preferred choice as they have better facilities and expertise than private hospitals which charge full fees and have very few NICU beds.
The Malaysian National Neonatal Registry (MNNR) was established with the objective to improve outcome of sick neonates in the NICUs by prospectively collecting patient data, annually analysing outcomes and recommending improvement strategies to participating centres. Participation in the MNNR was totally voluntary. Since its inception, the number of participating NICUs have increased progressively. By year 2009, all major government hospitals and some smaller ones had become members. The objectives of the present study were to investigate whether there was an improved trend of care practices, survival and major morbidities among VPTN in the MNNR over a 10-year period (2009–2018); and to identify predictors of mortality during epoch-1 (2009–2013) and epoch-2 (2014–2018).
Methods
This was a retrospective cohort study of prospectively collected data of all VPTN (gestation between 22 and <32 weeks) born between 1 January 2009 and 31 December 2018 and admitted to the participating NICUs. Their data were anonymised and submitted in a standardised format. Exclusion criteria were gestation <22 or ≥32 weeks, major congenital anomalies or readmission after 28 days of life. Data of neonates admitted multiple times or to more than one centre were merged.
Definitions
Gestation was reported in completed weeks based on antenatal ultrasound findings when available, or maternal last menstrual period in those with regular menses, or the New Ballard scores after birth.8 Antenatal steroids (ANS) were any administration of steroids before birth. Outborns were neonates transferred-in to a participating centre after birth. Early continuous positive airway pressure (eCPAP) therapy was defined as receiving CPAP in delivery rooms shortly after birth. Sepsis was diagnosed in symptomatic neonates with one positive blood culture. Clinical sepsis was not counted. Early-onset sepsis (EOS) was sepsis developed at ≤72 hours, and late-onset sepsis (LOS) as sepsis developed after 72 hours of life. Necrotising enterocolitis (NEC) was diagnosed based on presence of Bell’s stage 2 or 3 changes.9 Pneumothorax was diagnosed by chest radiographs. Bronchopulmonary dysplasia (BPD) was diagnosed in neonates on continuous oxygen therapy during first 28 days of life and still oxygen- or ventilator-dependent at 36 weeks’ gestation.10 Intraventricular haemorrhage (IVH) was diagnosed by cranial ultrasonography. Severe IVH (sIVH) was those with ≥grade 3 changes of Papile’s criteria.11 Based on the number of VPTN admitted, NICUs were categorised as ‘small’ with <50 VPTN admitted a year, ‘intermediate-sized’ with 50 to <100 VPTN admitted a year, and ‘large’ with ≥100 VPTN admitted a year.
Outcome measures
Outcome measures were care practices, survival, and major morbidities (admission hypothermia (AH, temperature <36.5°C), EOS, LOS, pneumothorax, NEC, sIVH and BPD).
Patient and public involvement
Patients and the public were not involved in the design and conduct of this study.
Statistical analysis
Neonatal data between the two epochs were compared using χ2 test and t-test, where appropriate. Simple and multiple logistic regression analyses were employed to identify predictors of in-hospital mortality. The dependent variable used was ‘outcome (dead or alive)’, and independent variables were birth weight, gestation, outborns, ANS therapy, modes of delivery, eCPAP, surfactant therapy, mechanical ventilation (MCV), types of NICU admitted, AH, pneumothorax, LOS, NEC and sIVH. Gestation and MCV were variables subsequently excluded from the final logistic regression analysis because of collinearity with birth weight, modes of delivery and surfactant therapy. All tests were two sided. Values of p<0.05 were considered statistically significant. SPSS (V.24.0, IBM) was used for analyses.
Results
Demographic data
A total of 29 010 neonates were recruited (figure 1). The number of NICUs increased from 32 in 2009 to 43 in 2018 (table 1); 17 were small, 18 were intermediate-sized and 9 were large NICUs. There was no marked increase in the number of neonates over the years because two NICUs did not submit data since 2016, three did not submit data between 2014 and 2016, and five newer members were small NICUs. Twenty-eight centres participated in all 10 years contributing to 86.2% (n=25 078) of the total number of neonates recruited, three centres for 9 years (2.3%, n=670), three centres for 8 years (5.9%, n=1706), four centres for 7 years (2.6%, n=759), four centres for 5 years (2.5%, n=726), one centre for 3 years (0.2%, n=56) and one centre for 2 years (0.05%, n=15). Table 1 shows the demographic characteristics of the neonates recruited.

Flow diagram of enrolment of very preterm neonates, 2009–2018. NICU, neonatal intensive care unit.
Annual demographic, clinical and outcome data of very preterm neonates, between 2009 and 2018
Perinatal care and major morbidities
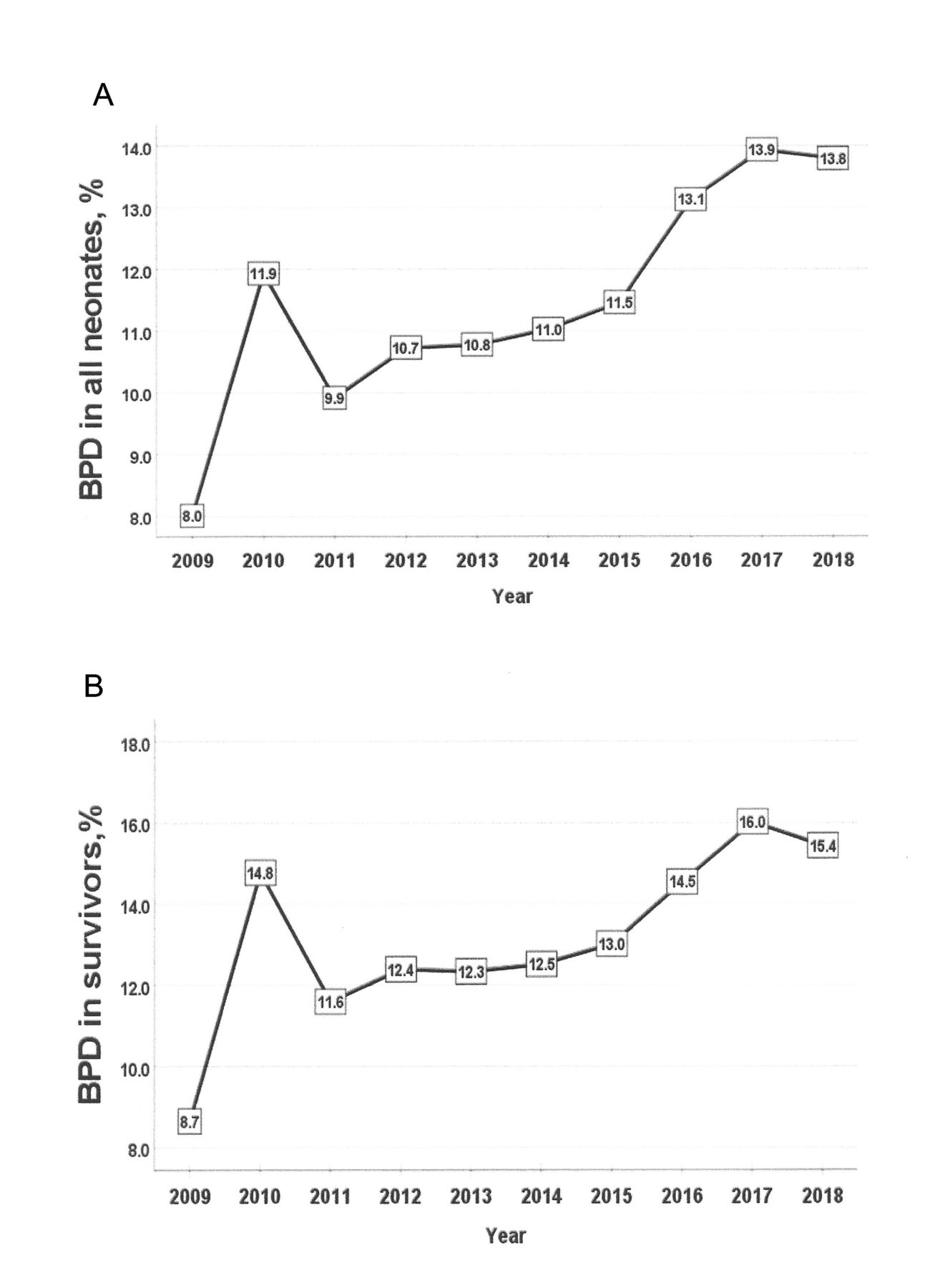
During this period (figure 2), use of ANS, lower segment caesarean section (LSCS) and eCPAP had increased. Use of surfactant therapy for respiratory distress syndrome had decreased. The median admission temperature remained static at 36.0°C. Incidences of mild AH (36.0°C–36.4°C) decreased from 26.6% in 2009 to 22.6% in 2018, moderately severe AH (MSAH, 32.0°C–35.9°C) increased from 36.3% to 44.6% and severe hypothermia (<32.0°C) remained static (figure 3). Incidences of LOS, pneumothorax, NEC and sIVH had decreased, but BPD had increased (figure 4).

Trend of perinatal care in very preterm neonates, 2009–2018. CPAP, continuous positive airway pressure; LSCS, lower segment caesarean section.
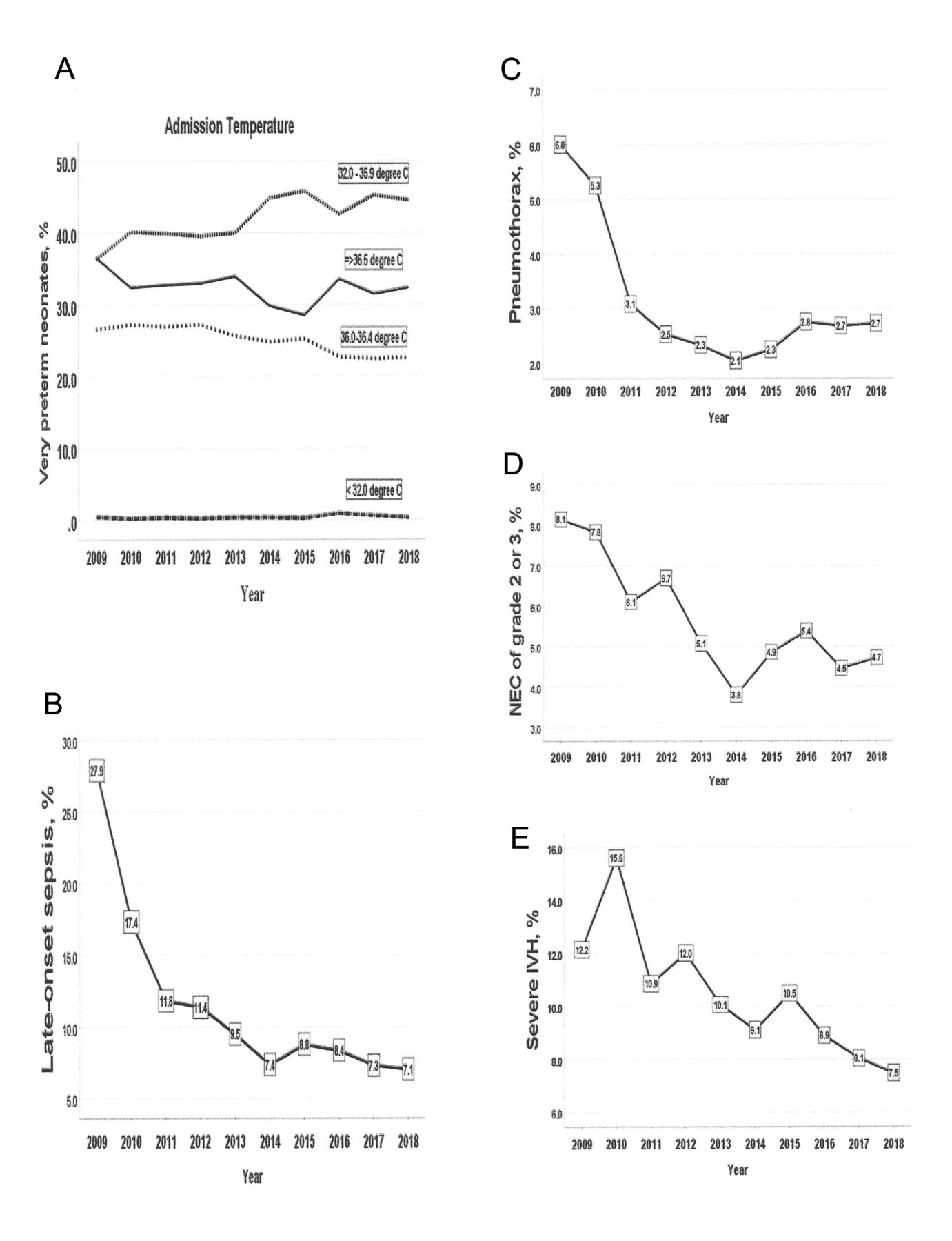
Trend of early morbidities in very preterm neonates in MNNR, 2009–2018. IVH, intraventricular haemorrhage; MNNR, Malaysian National Neonatal Registry; NEC, necrotising enterocolitis.

Trend of bronchopulmonary dysplasia (BPD) in very preterm neonates in MNNR, 2009–2018. MNNR, Malaysian National Neonatal Registry.
Survival trend
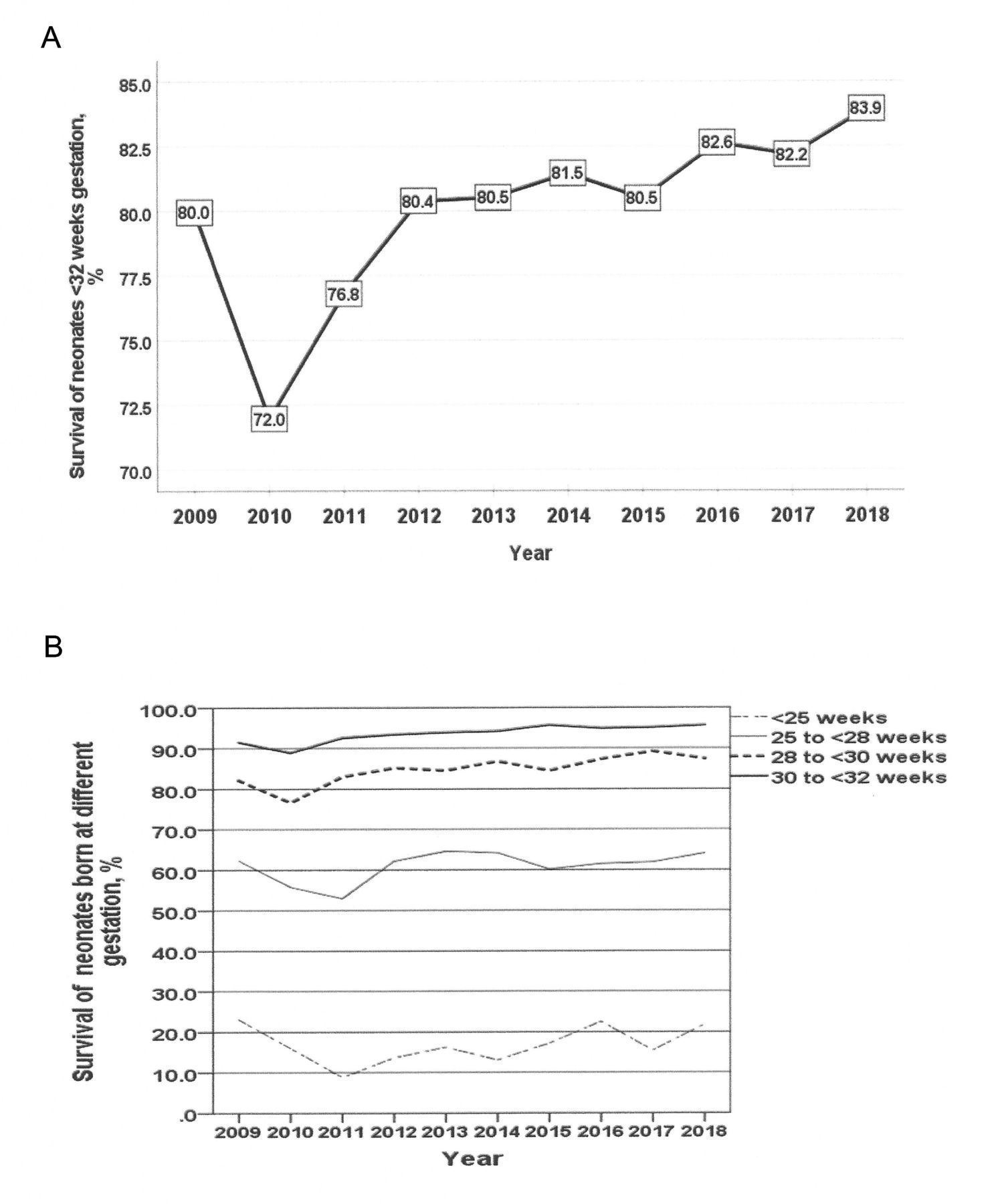
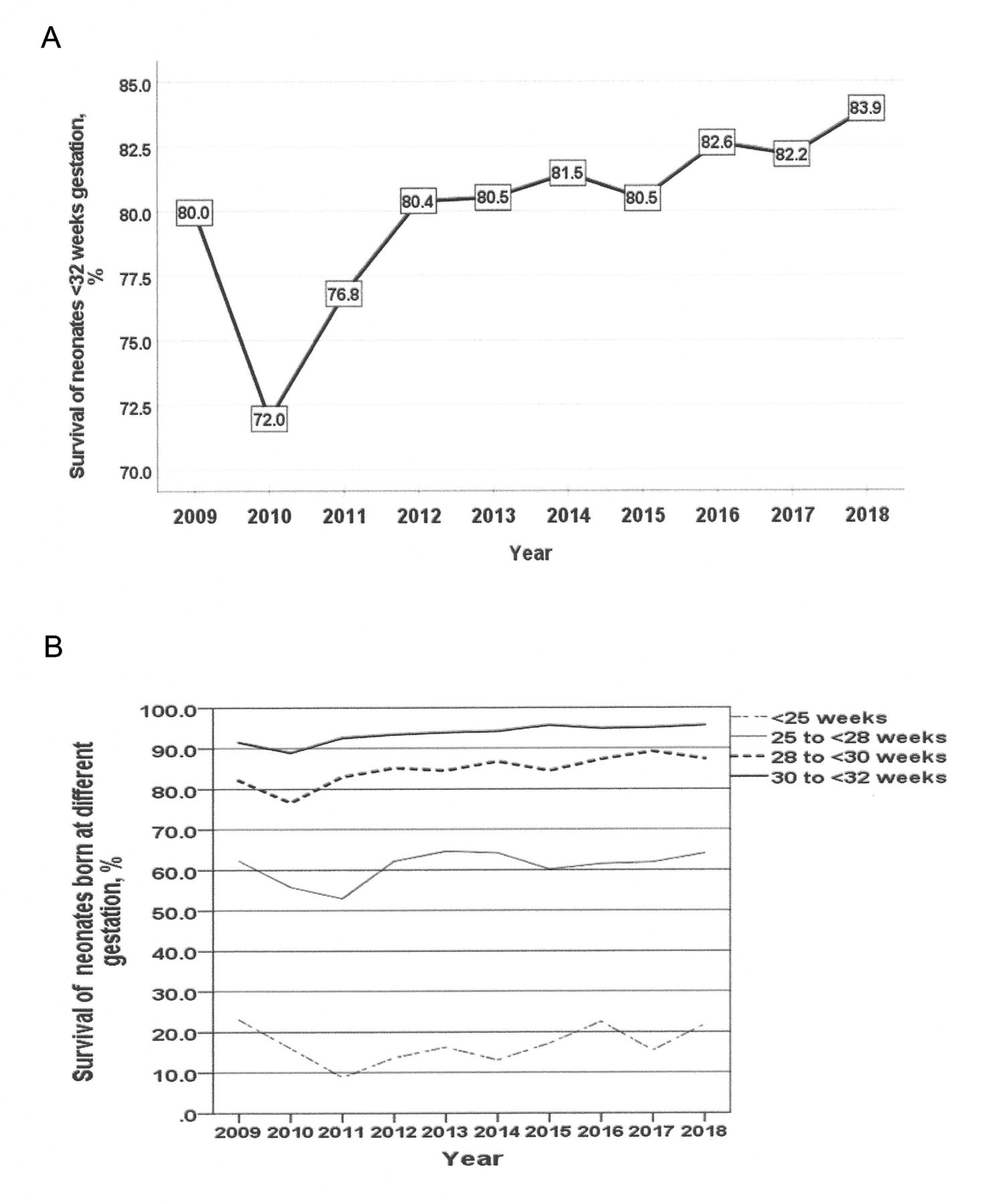
Survival of all neonates decreased from 80.0% in 2009 to 72% in 2010, then increased gradually over the years to 83.9% in 2018 (figure 5A). Survival of <25 week-gestation neonates remained static (figure 5B), those of 25 to <28 week gestation increased slightly by about 2% point, and those of gestation ≥28 increased by about 4% point. When compared with neonates in epoch-1 (table 2), those in epoch-2 had significantly higher survival rates.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Trend of survival of very preterm neonates in the MNNR, 2009–2018. MNNR, Malaysian National Neonatal Registry.
Comparison of demographic, clinical and early outcome characteristics of very preterm neonates (<32 weeks gestation) between two epochs
Risk factors associated with mortality
Multiple logistic regression analysis was carried out on 11 277 (alive: n=9218, dead: n=2059) neonates with complete data in epoch-1 (table 3). The significant predictors of mortality were lower birth weight, admission to NICUs with <100 VPTN admissions/year, MSAH, no ANS, breech delivery, LOS, pneumothorax, NEC and sIVH. The Nagelkerke R2 of the model was 0.391, Hosmer and Lemeshow test p=0.003; 95.6% of survivors and 42.1% of deaths were correctly predicted by the model. Area under receiver operating characteristic curve (ROC) was 0.852 (95% CI 0.842, 0.861). Outborns and surfactant therapy were not significant predictors.
Logistic regression analysis of potential predictors of in-hospital mortality in the two epochs
Multiple logistic regression analysis was carried out on 13 326 (alive: n=11 308, dead: n=2018) neonates with complete data in epoch-2 (table 3). Lower birth weight, admission to NICUs with <100 VPTN admission/year, moderate and severe AH, no ANS, vertex and breech deliveries, no surfactant therapy, no eCPAP, LOS, pneumothorax, NEC and sIVH were significant predictors of in-hospital mortality. Outborn was not a significant predictor. The Nagelkerke R2 for the model was 0.417, Hosmer and Lemeshow test p=0.024; 96.6% of survivors and 44.0% of deaths were correctly predicted by this model; ROC=0.871 (95% CI 0.862 to 0.880).
Discussion
During this 10-year period in the MNNR, there was an increased trend in the use of ANS, LSCS and eCPAP; a decreased trend of major morbidities (LOS, NEC, sIVH, pneumothorax) and mortality; and an increase in MSAH and BPD. Since its inception, the MNNR has been collecting data on mortality, morbidity and care practices to evaluate the relationship of these care practices on morbidities and mortality. Unlike NICUs in HICs, resource limited Malaysian NICUs did not have full-time personnel to collect data for the MNNR. To avoid overloading designated nurses who collected these data as part of their duty, we included only care practices that previous studies had reported to be beneficial in HICs. Thus, data on ANS was included because studies in HICs reported reduced neonatal death and RDS, and probably reduced risk of IVH.12 13 Use of eCPAP therapy was associated with better survival in spontaneously breathing preterm neonates.14 15 Use of plastic wrap/bag on VPTN in delivery rooms was a crucial step in preventing hypothermia and stabilising tiny neonates.16 Numerous trials showed surfactant therapy improved oxygenation, and decreased ventilator support, air leak and death.17
Despite increased use of ANS in the MNNR, our highest rate (78.7% in 2018) was still lower than those in many HICs where rates were >85%.1–4 Our highest eCPAP rate in 2018 (58.4%) was still lower than that (64.8%) reported by the South American multinational network.18 Our highest LSCS rate by 2018 was comparable with most HICs networks.1–5 During the first 8 years of this study period, only data on admission temperature was collected to monitor AH. When our annual review showed increasing trend of AH, we included ‘use of plastic wrap/bags’ in our database since 2016. Our results showed dismally low rates of use of plastic wrap, which probably accounted for the high MSAH incidence.
Like studies elsewhere19 20 we found NICUs with low volume VPTN admissions (<100 neonates/year) were significant predictors of mortality. In Malaysia, regionalisation of care for VPTN has not been implemented successfully during this period because of limited number of NICU beds in larger centres. The findings of this study reinforce the importance of regionalisation of care because big NICUs have more experience and expertise in the care of these very high-risk neonates. Our study also concurs with other investigators that neonates born by vertex21 22 and breech deliveries23 had significantly higher risk of mortality than LSCS. Our result confirms a recent WHO study24 that ANS improves mortality of VPTN in LMICs like those in HICs.12 13 Similarly, we found the use of eCPAP14 and surfactant therapy25 26 were associated with better survival. MSAH16 was a predictor of mortality
The most marked improvement in morbidities in the MNNR was LOS during this 10-year period (figure 3). By 2014, our LOS incidence (7.0%) was lower than those of many HIC NICUs.27 28 However, since 2014 our LOS incidence had plateaued, and continued to be a significant predictor of mortality as reported elsewhere,28 indicating more efforts are needed to reduce this problem. Although our NEC incidence had decreased to lower levels than the Spanish network, which reported a persistent incidence of 8.8% over 13 years,29 it was higher than the Swiss network which maintained an incidence of 2.5% over 13 years.5 Recently a UK centre30 reported marked reduction in NEC incidence from 7.5% in 2008–2012 to 3.1% during 2013–2017 following introduction of probiotics. In Malaysia, only two centres used probiotics (one since 2011 and a second centre since 2016). We attributed the reduction of NEC in the MNNR to our efforts in improving handling of breast milk from the time of expression of breast milk by the mothers, during transport, to storage and administration of expressed breast milk to the neonates in the NICUs.
Like other HIC networks, the survival of our VPTN had increased. However, our highest survival rate attained by 2018 (83.9%) was still lower than those of many HICs where rates were ≥90%.1 2 4 5 Our improved survival was most marked in higher gestation groups, unlike those in HICs where lower gestation groups had the most marked improvement in recent years. One reason for this difference is that the survival of higher gestation VPTN in these HIC had already achieved ≥90% since previous decade.1 3–5 7 A second reason is the limited resources led many of our NICUs to focus their care more on higher gestation VPTN.
There were several factors contributing to improved survival in the MNNR over these 10 years (table 2). In epoch-2, there were more mature and heavier VPTN born; moderately higher rates of use of ANS, LSCS, and eCPAP; and lower proportions of outborns, LOS, pneumothorax, NEC and sIVH than in epoch-1. However, in epoch-2, there were more VPTN admitted to smaller NICUs, less use of surfactant and higher rates of moderate and severe AH. These two sets of opposing factors most likely accounted for the modest magnitude of improved survival, as multivariate logistic regression analysis showed that failure to use these care practices and presence of major morbidities were significant predictors of mortality. To improve survival further, we need to increase the use of these care practices and reduce major morbidities further, with particular focus on decreasing incidence of AH. A quality-improvement study in Canada over a 14-year period (2004–2017) demonstrated that increased use of ANS, and increased rates of admission normothermia resulted in significant increase in survival without major morbidity in their VPTN.23
Like reports from HICs networks,1 the incidence of BPD in MNNR had increased during these 10 years. This means the quality of life of surviving VPTN in the MNNR would be compromised. While efforts are needed to improve survival further, there is an urgent need to investigate and prevent factors associated with increasing BPD. Furthermore, as all major morbidities (LOS, NEC, BPD and sIVH) adversely affect neurodevelopment outcomes of VPTN, we need to identify and implement effective strategies to further reduce these morbidities. By doing so, this will also help to reduce in-hospital mortality.
In this study, we have identified four relatively low-cost modifiable care practices with potential to further improve survival and morbidities in Malaysian NICUs. They are (A) use of ANS, (B) prevention of MSAH, (C) use of eCPAP and (D) prevention of LOS. Given our country’s limited resources, our priorities to further improve outcome should be (A) increasing use of ANS for impending premature delivery and (B) allocating more funding for facilities and training on use of eCPAP, prevention of hypothermia in delivery rooms and during transport, and prevention of LOS in NICUs.
The following are the strength of this study: (A) 10-year outcome trend of VPTN from a middle income country’s neonatal network, (B) a standardised format was employed to collect data prospectively, (C) more than 90% of the tertiary Malaysian NICUs participated; (D) high proportion of the data were from 28 large centres participating in all 10 years, (E) association of care practices and major morbidities with in-hospital mortality were evaluated and (F) various low-cost modifiable factors for future improvement were identified. The main limitation of this study is not having all NICUs participated during all 10 years.
In conclusion, there was a modest improvement in survival, major morbidities, and use of care practices during this 10-year period in the MNNR.
Data availability statement
Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as online supplemental information. The data are obtained from the database of the Malaysian National Neonatal Registry.
Ethics statements
Patient consent for publication
Ethics approval
Parental consent was not obtained as the database was anonymised. Ethical clearance for the MNNR was granted by the Malaysian Ministry of Health and registered under the National Medical Research Registry (NMRR-05-04-168).
Acknowledgments
We would like to thank the Director General of Ministry of Health of Malaysia for permitting us to publish this paper and the site coordinators of participating hospitals: Zuraidah Abdul Latif (Ampang Hospital), Zainah Shaikh Hedra (Sultanah Nora Ismail Hospital, Batu Pahat), Anand Mohana Mohana Lal (Bintulu Hospital), Baizura Jamaluddin (Kajang Hospital), Shiva Rubini Thambirajoo (Keningau Hospital), Irene Guat-Sim Cheah (Tunku Azizah Hospital), Hasri Hafidz (Tuanku Ampuan Najihah Hospital, Kuala Pilah), Zainab Ishak (Kulim Hospital), Poy-Lee Leow (Melaka Hospital), Siao-Hean Teh (Miri Hospital), Mehala Devi Baskaran (Pulau Pinang Hospital), Maslina Mohamad (Putrajaya Hospital), Noor Khatijah Nuraini (Raja Permaisuri Bainun Hospital, Ipoh), Hasmawati Hassan (Raja Perempuan Zainab II Hospital, Kota Bharu), Thian-Lian Soo (Sabah Women and Children’s Hospital), Lee-Gaik Chan (Sarawak General Hospital), Choo-Hau Lim (Seberang Jaya Hospital), Rohaizah Borhan (Serdang Hospital), Seok-Chiong Chee (Selayang Hospital), Sheila Gopal Krishnan (Seri Manjung Hospital), Pei -Ying Kwan (Duchess of Kent Hospital, Sandakan), Intan Nor Chahaya Shukor (Segamat Hospital), Chae-Hee Chieng (Sibu Hospital), Chong-Meng Choo (Sultan Abdul Halim Hospital, Sungai Petani),Yun-Yun Ng (Sultanah Bahiyah Hospital, Alor Setar), Hooi-Kheng Tan (Sultan Haji Ahmad Shah Hospital, Temerloh), Mohd Nizam Mat Bah (Sultanah Aminah Hospital, Johor Bahru), Angeline Seng- Lian Wan (Sultanah Fatimah Specialist Hospital, Muar), Jimmy Kok-Foo Lee (Sultanah Nur Zahirah Hospital, Kuala Terengganu), Kwee-Ching See (Sungai Buloh Hospital), Rohani Abdul Jalil (Taiping Hospital), Hui-Sui Tan (Teluk Intan Hospital), Choy-Nyok Chin (Tengku Ampuan Afzan Hospital, Kuantan), Yogeswary Sithamparanathan (Tengku Ampuan Rahimah Hospital, Klang), Abdul Nasir Mohamed Abdul Kadher (Tuanku Fauziah Hospital, Kangar), Umathevi Paramasivam (Tuanku Ja'afar Hospital, Seremban), Lee- Ser Chia (Sultan Ismail Hospital, Johor Bharu), Noraida Ramli (Universiti Sains Malaysia Hospital, Kubang Kerian), Alice Man-Mooi Ho (University of Malaya Medical Center), Ananda Dharmalingam (Gleneagles Hospital Kuala Lumpur), Ismail Haron (KPJ Puteri Specialist Hospital), Elaine Ee-Lane Wong (Kluang Hospital), Mohd Hanifah Mohd Jamil (Kuala Krai Hospital).
References
Footnotes
Contributors Conceptualisation, NYB; data cleaning, NYB, SHN, SCC, EBKA, ELA, PC, FIS-A, ACW and AAK; data analysis, NYB; manuscript preparation, NYB; review and editing manuscript, NYB, SCC, SHN, EBKA, ELA, PC, AAK, FIS-A and ACW.
Funding This work was supported by the Perinatal Society of Malaysia.
Competing interests No, there are no competing interests.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.