Article Text

Abstract
Background Following a finding of alcohol use among children aged 5–8 years old in Mbale, Uganda, this project investigates the magnitude of alcohol and substance use among children ged 6–13 years old and related household, community, school, health system and clinical factors.
Methods The project includes four larger work packages (WPs). WP1 comprises management, WP2 and 3 include the scientific components and WP4 includes integration of results, dissemination, policy and implementation advice. This protocol presents the planned research work in WP 2 and 3. WP2 comprises the adaptation and validation of the alcohol use screening tool Car-Relax-Alone-Forget-Family and Friends-Trouble (CRAFFT) to the age group and setting. WP3 comprises four substudies (SS). SS1 is a cross-sectional community household survey with an estimated sample size of 3500 children aged 6–13 years and their caregivers. We apply cluster sampling and systematic sampling within the clusters. Data collection includes a structured questionnaire for caregiver and child, measuring social and demographic factors, mental health status, alcohol and substance use, nutrition history and anthropometry. Urine samples from children will be collected to measure ethyl glucuronide (EtG), a biological marker of alcohol intake. Further, facilitators, barriers and response mechanisms in the health system (SS2) and the school system (SS3) is explored with surveys and qualitative assessments. SS4 includes qualitative interviews with children. Analysis will apply descriptive statistics for the primary outcome of establishing the magnitude of alcohol drinking and substance use, and associated factors will be assessed using appropriate regression models. The substudies will be analysed independently, as well as inform each other through mixed methods strategies at the stages of design, analysis, and dissemination.
Ethics and dissemination Data protection and ethical approvals have been obtained in Uganda and Norway, and referral procedures developed. Dissemination comprises peer-reviewed, open access research papers, policy recommendations and intersectoral dialogues.
Trial registration number
Clinicaltrials.gov 29.10.2020 (#NCT04743024).
- adolescent health
- child psychiatry
- epidemiology
- qualitative research
- health services research
Data availability statement
Data sharing not applicable as no complete datasets are generated and/or analysed for this study. Data collection is not yet completed, and there are no available data to share from this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Uganda has a relatively high consumption of alcohol, estimated to 12.2 (10.1–14.6) litres of pure alcohol, according to the 2019 Global Health Observatory data.
Any level of alcohol consumption, regardless of the amount, leads to loss of healthy life and children are at greatest risk of harm.
In Uganda, regional and demographic patterns vary, and for some alcohol production and consumption is widely practised part of their culture.
What this study hopes to add?
This research aims to describe the prevalence of alcohol consumption and substance use among children aged 6–13 years old in Mbale District, Eastern Uganda.
Substudies investigate the health and school system’s approaches to management of children that have challenges with substance use.
The study explores risk and protective factors for childhood alcohol use to inform screening, policy formulation and implementation of prevention and intervention programmes.
Introduction
Harmful use of alcohol is an important public health issue.1 Limited attention has been given to preadolescence or childhood alcohol drinking,2 and existing research mainly come from high income countries.2 In sub-Saharan Africa, there has been limited research about child mental health in general, and alcohol and substance use in particular.3 However, some reports on early substance use do exist. In 2018, a study with data from the Global School-Based Student Health Survey (GSHS) showed that among participants in African countries, 13.4%–15.5% reported alcohol intake before age 11.4 The most recent Ugandan GSHS from 2003 reported that 15.2% of 13–15 years had been ‘really drunk’ and 8.5% had used other drugs.5 These high rates of adolescent drinking suggest an early initiation of alcohol use, although more recent data are lacking.
Early-onset alcohol and substance use is an important predictor for developing alcohol and substance use disorders and mental health conditions later in life.6 Neurological, psychological and social child development7 may be disturbed by alcohol and substance use. It is also associated with a variety of negative mental and somatic health outcomes in addition to social risky behaviour including violence, crime and school drop-out.2 8 If drinking starts before the age of 10 years, structures in the child’s developing brain involved in functions sentinel for social and academic achievements such as planning, learning, attention, appetite, reward and emotional and behavioural control may be affected.7
Uganda is a low-income country in East Africa with more than 42 million inhabitants, equivalent to almost 180 people per square km, ranking among the top ten most densely populated African countries. Almost half the population is younger than 15 years of age. It ranks 159/189 on the human development index report from 2020 and has an average of 6 years of formal schooling.9 Like many other sub-Saharan countries, Uganda has a comparably high alcohol consumption per capita,10 and traditions of home brewing are common.11 In 2014, we identified a prevalence of 8.4% clinically defined harmful alcohol use or dependence in a sample of children aged 5–8 years (n=119) with a high mental health symptom load.12 This prompted further qualitative investigation, which corroborated our finding.
The research project: TREAT Child Alcohol Use Disorder (C-AUD) in Eastern Uganda: screening, diagnostics, risk factors and management of children drinking alcohol, funded by the Norwegian Research Council (TREAT C-AUD) (#285489), is a 5-year project initiated in 2019 to answer questions regarding alcohol and other substance use in childhood. ‘'Alcohol use disorder’ (AUD) is a diagnostic term from the Diagnostic and Statistical Manual of Mental Disorders (DSM–5), classified into mild, moderate and severe disorder. Our project has adapted this term to childhood and preadolescence and constructed the term C-AUD. In our study, we will investigate both the prevalence and associated factors of childhood substance and alcohol use (beyond sipping and tasting), as well as evaluate screening and diagnostic criteria for the term C-AUD. The project’s objectives are to investigate the magnitude of substance use, alcohol use and C-AUD in children, and related household factors, its management in the school and health sector and improve contextual understanding, and to engage in the public health dialogue and policy recommendations in Uganda.
Methods
Site description
The study site is Mbale District in Eastern Uganda, 245 km from the capital Kampala. Situated close to the Kenyan border, Mbale City is the main urban trading area in the district, which is predominantly rural and dominated by peasant farming. The staple crops include millet and maize grain which are also commonly used for home brewing. The urban area has a regional referral hospital with a psychiatric department.
Study design
The TREAT C-AUD project will use both qualitative and quantitative methods (table 1). The project includes four larger work packages (WPs) (figure 1). WP1 comprises management, WP2 and 3 include the scientific components and WP4 includes integration of results, dissemination, policy and implementation advice. This protocol presents the planned research work in WP 2 and 3. WP2 comprises the adaptation and validation of a screening tool for childhood alcohol and substance use. WP3 has four substudies, and it includes quantitative and qualitative data collection methods on epidemiological and contextual data from the community households, health system, school system and children’s perspectives.

TREAT C-AUD Protocol: work packages (WP) and substudies (SS)*. *The mixed-methods diagram illustrates how we apply interlinked qualitative and quantitative research methods in the design and the analysis of the TREAT C-AUD research project. C-AUD, Child Alcohol Use Disorder; CRAFFT, Car-Relax-Alone-Forget-Family and Friends-Trouble.
The work packages and substudies in TREAT C-AUD
Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the 'Patient and Public Involvement' section for further details.
Separate data collection from the substudies will be analysed independently, as well as inform each other through mixed-methods strategies at the stages of design, analysis and dissemination. There are many ways to mix methods and procedures at the design, analysis and interpretation stages.13 Thus, according to Zhang and Creswell, 2013, our project qualifies as a mixed methods project having both concurrent and sequential elements of mixing qualitative and quantitative methods at the design, conduct and interpretation stages.
WP2: screening tool adaption and validation
We will adapt the Car-Relax-Alone-Forget-Family and Friends-Trouble (CRAFFT) screening tool to the age group and setting by multidisciplinary committee review, as recommended by WHO.14 This includes forward and backward translations of tools by bilingual independent translators; rereview of translated versions and conciliation with authors; pilot testing with qualitative assessment and quantitative reliability and validity assessment. We will conduct psychiatric interviews using the MINI International Neuropsychiatric Interview for Children and Adolescents (MINI-KID)15 diagnostic tool (adapted for DSM-5 based on the English V.7.0.2)16 as the gold standard for validation. We will evaluate the use of the screening tool and diagnostic criteria for C-AUD in synergy with the WP3 health systems component, where we investigate the clinical practice related to substance and alcohol use, and possible C-AUD in children.
WP3: community household, health system, school system and children’s perspectives
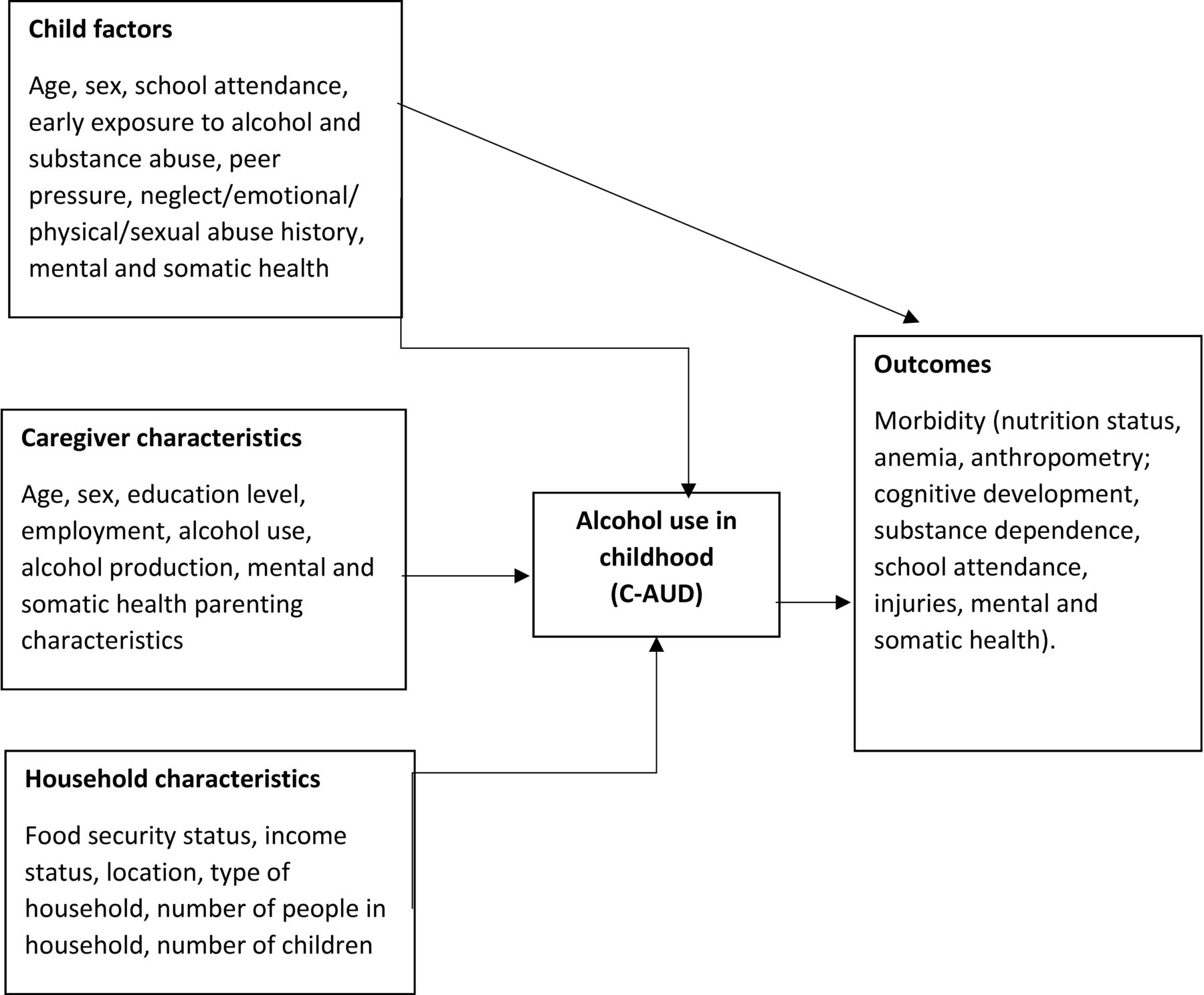
WP3 builds on a conceptual framework (figure 2) where the development of C-AUD and its effect is influenced by factors related to the child, caregiver and household. The WP includes four substudies: a community household survey, a health system study, a school study and qualitative studies of children’s perspectives. The health system and school studies use mixed methodologies.
{kind=link}
{kind=link}
Conceptual framework of the interplay between C-AUD, risk factors and outcomes. C-AUD, Child Alcohol Use Disorder.
Community household survey
A two-stage stratified cluster survey as recommended by the 2018 WHO coverage survey reference manual will be used17 since the district does not have a registration system for the household or household members.
A sample size of 3500 children is estimated with the following assumptions: prevalence of alcohol consumption of 4%, a precision of 3.6%, a 95% confidence level and a design effect (DEFF) of 2.18 The number of households to visit is estimated at 2982, computed from the effective sample size multiplied by ‘DEFF‘, the proportion of households with eligible children and the nonresponse rate (10%) as demonstrated in table 2. Non-response is considered if caregivers are absent from the household, refusal to provide consent to study participation, uninhabited households among other reasons.
Sample size estimates for the target group (6–13 years), TREAT C-AUD study
A two-stage sampling procedure will be used. In the first stage, 99 clusters (villages) will be selected based on probability proportionate to population size. The second stage of selection will be based on the household listing, which shall be done by the research teams in the selected clusters. Serial numbers shall be allocated for unique identification for each household along with their respective GPS coordinates. It is from this stage that systematic sampling without replacement shall be done using Open Data Kit app (ODK) (https://opendatakit.org/) predesigned template for the selection of the 30 households in each cluster. The starting point for each cluster will be randomly selected by the ODK. All selected households will then be visited irrespective of having an eligible child. Household visits will be attempted on three consecutive visits to the household on three separate days before the attempted interview is labelled void. The WHO reference manual for Cluster Surveys17 recommends interviewing every eligible child in the household which we will adhere to. Survey data will be collected using the ODK platform.
The survey questionnaire includes several scales, as well as questions designed by the TREAT C-AUD research team. We address mental health, somatic health and social factors associated with the main objective: alcohol and substance use in children. A schematic list of the tools is provided in table 3. We shall assess caregiver mental health status using the WHO Self-Reporting Questionnaire-20,19 which has been validated in Uganda.20 Children’s mental health status will be measured by child and caregiver response of the Paediatric Symptom Checklist-35,21 which has been validated in Batswana.22 We measure caregiver traumatic experiences with the Stressful Life Events Screening Questionnaire,23 using the revised version developed to improve cross cultural validity.24 Traumatic experiences in the children are assessed with the Child and Adolescent Trauma Screen, with good psychometric properties in international validation,25 and previous use in Uganda.26 For both child and caregiver, we assess post-traumatic stress symptoms using a 2-item abbreviated version of the PTSD Checklist-Civilian version.27 The Alabama Parenting Questionnaire (APQ) has a parent and a child form, and measures parenting practices.28 We will use a short version (APQ-15), which has been used in cross cultural settings and has been validated for the age group.29 30 Both the child and caregiver will answer the Conflict Tactics Scale-Parent-Child version,31 which has been validated for the age range 6–13 years32 and has demonstrated good cross-cultural reliability and validity, including in East Africa.33 We assess caregiver alcohol use with the WHO Alcohol Use Disorders Identification Test (AUDIT), which has been cross-culturally validated.34 To assess child alcohol and substance use, we include the adapted CRAFFT screening tool. Further, we have included questions from the GSHS35 to explore the extent and consequences of alcohol and substance use, and questions from the US National Survey of Parents and Youth to explore caregiver–child communication about substance use,36 and the National Longitudinal Study of Adolescent to Adult Health (Add Health study) to explore peer-use.37 Disability will be assessed using the Washington Group/UNICEF Child Functioning Module.38 Child nutrition status will be assessed by asking the caregiver about food diversity, frequency and food security.39 We will take anthropometric measurements and collect urine from children to measure Etylglucoronate, which is a metabolite of ethanol, reflecting recent alcohol consumption.40
List of tools and measures in the community household survey in the TREAT C-AUD project
Analysis will include standard descriptive statistics, using frequencies and percentages for categorical variables, and medians with ranges and means with 95% CIs for continuous variables. To establish the magnitude of alcohol drinking and substance use among all children in the survey, prevalence will be given as cluster-adjusted percentage. A positive screen on the CRAFFT tool is defined as a score ≥1 on the 6 CRAFFT items. Age group (6–9 and 10–13 years old) and sex stratified prevalence will be provided. Assessments of associated risk factors will include multiple dimensions of care and parenting, socio-economic status and education, and mental health symptoms of the child and carer.
Health system study
In the health system study, we adopt the WHO framework for health systems service delivery to explore the readiness of the health system in Mbale district to screen, diagnose and manage children with C-AUD. We apply a mixed-methods approach, including a review of patient and government records, as well as key informant interviews with health workers and caregivers of children aged 6–13 years. We will explore five main domains; service delivery, human resources, health financing, pharmaceuticals and other medical products, health management information system (HMIS). In broad terms, we seek to investigate the referral pathways, estimate the proportion of detected and treated C-AUD in the health system, assess the health system capacity and competence for managing C-AUD, explore the functionality of the Ugandan HMIS for C-AUD and evaluate existing health financing mechanisms for prevention and treatment of C-AUD. An item topic guide for each domain has been developed and is given in table 4. Data collection for these objectives is yet to commence.
Item topic guide for the health system substudy
School study
In the school study, we aim to understand how childhood alcohol and substance use is viewed and managed within the education sector, including the degree of awareness, formal and informal response mechanisms, and the schools’ interaction with the health sector.
First, we will conduct a survey among teachers of 148 public and private primary schools, representative for Mbale district. We will investigate their awareness of childhood alcohol and substance and their use of formal and informal response mechanisms. Moreover, we aim to estimate to what degree teachers understand childhood substance and alcohol use, herein C-AUD, as a developmental challenge that requires their response. These data will be analysed using both descriptive and analytical statistics.
Second, two qualitative components of the school study will explore the perceptions on childhood alcohol and substance among school heads and school health personnel from the health sector. This inquiry includes a section on current bottlenecks and untapped response potentials between the sectors. These components will be recoded, transcribed, and analysed using framework analysis. Further, we aim to triangulate these results against the quantitative results to obtain a more robust and integrated picture of their views and existing school-based response mechanisms. We also probe for suggestions on better management of childhood alcohol and substance in schools and between the sectors. The tools for data collection are not yet pretested and data collection is scheduled for 2022.
Children’s perspectives
We will conduct qualitative interviews with children to gain a more context specific and in depth understanding of childhood alcohol and substance. Children will be involved at various stages during the project period. They will be asked to express their thoughts during qualitative interviews on general questions related to what alcohol and substance use are, what they are taught about it and who they rely on if they need it. We aim to understand children’s understanding and perceptions on the topic. Further, they will be interviewed to give their views on the various elements of the adapted CRAFFT tool. Both qualitative interviews and focus group discussions will be used.
Analysis, interpretation and integration
Quantitative descriptive analysis will include proportions, prevalence estimates and 95% CIs. The cluster design will be adjusted for, and sampling weights considered. The cross-sectional study designs have an inbuilt dilemma with reverse causalities, and only associated factors can be given. However, we plan for the binary substance use outcome to assess in logistical analysis, which factors that have a higher odd of being associated with the practice.
Qualitative analysis will include content analysis. All substudies will be analysed and presented separately, and integration of results will only happen after each substudy is individually analysed and interpreted. Mixing of results will happen at the level of synthesis, dissemination and policy advice.
Patient and public involvement
Patient (child) and public (stakeholders and experts) involvement will be sought on multiple levels. The Ugandan Ministry of Health was consulted regarding the design of the protocol and will be invited for dissemination meetings. Children and experts will be involved in adapting the screening tool for alcohol use detection at the stage of development (translate, discuss and adjust) and testing (quality assurance and epidemiological study). Moreover, patients and public stakeholers will be involved in the reporting and dissemination plans of this research.
Ethics and dissemination
Ethical approval was obtained from the Regional Committees for Medical Research Ethics-South East Norway 6 March 2020, reference number 50 146 and Makerere University College of Health sciences, School of Public Health, Higher degrees, Research and Ethics Committee 7 February 2020, reference number 745. In Uganda, the research project was registered at the Uganda National Council for Science and Technology, reference number SS 5245. Dissemination comprises peer-reviewed, open access, English language research papers, and policy recommendations and intersectoral dialogues relevant for public health policy. Data will be stored and kept in Uganda, controlled by Makerere School of Public health, and transferred abroad based on data transfer and storage agreements. Only officially acknowledged secure data management and analysis systems will be used in line with General Data Protection Regulations in both Norway and Uganda.
Status of progress
The adaptation of the CRAFFT tool was done between September 2019 and March 2020. This included consultations with experts and insight from qualitative interviews with 56 children. Analysis and write up for this are ongoing. Validation of the CRAFFT tool was conducted between September 2020 and March 2021 with 470 primary school age children and data entry is on-going. Data collection for the community household survey commenced on the 12th of November 2021 and data cleaning is on-going. Preliminary numbers show that a total of 4648 households were visited in 99 enumeration areas. 2575 of the visited households had eligible children and 3887 children were eligible for study participation. A total of 3594 children were enrolled into the study. We collected urine samples and anthropometric measurements for each enrolled child. Data collection for the health system and school study has not yet commenced. Further qualitative data collection with children exploring explanatory factors and context are planned and has not yet commenced.
Data availability statement
Data sharing not applicable as no complete datasets are generated and/or analysed for this study. Data collection is not yet completed, and there are no available data to share from this study.
Ethics statements
References
Footnotes
VS and HA are joint first authors.
IMSE and JNB are joint senior authors.
Twitter @ingunnengebret1
Collaborators The TREAT C-AUD consortium. Principal investigators: Uganda: Juliet Ndimwibo Babirye, MD, MPH, PhD, Senior Lecturer, and Norway: Ingunn Marie S. Engebretsen, MD, PhD, Professor (made the first manuscript draft). Participating countries, institutions, investigators (alphabetical) and roles: Uganda: Makerere University, College of Health Sciences, School of Public Health: Harriet Aber, BSc food Science and technology, MA Public Health Nutrition, Public health nutrition. Esther Kisaakye, BSc Nursing, MA Public Health, implementation. Henry Wamani, MD, PhD, Public health nutrition. Deogratious Sebuwufu, MA Statistics, MA Business Administration, Diploma in Law, Diploma in Systems Engeneering, data management and statistics, Makerere University, College of Health Sciences, School of Public Health and School of Medicine, Department of Psychiatry, Mulago National Referral Hospital. Joyce Sserunjogi Nalugya, MD specialized in Child and Adolescent Psychiatry. Norway: University of Bergen, Faculty of Medicine, Department of Global Health and Primary Care, Centre for International health. Melf-Jacob Kühl, MA Public Policy, MA Laws. Vilde Skylstad, MD, PhD candidate (corresponding author). Neda Valeckaite, Medical Student. University of Bergen, Faculty of Medicine, Department Clinical Medicine, Centre for Nutrition, Mohn Nutrition Research Laboratory: Jutta Dierkes, PhD. Professor, Nutrition. University of Bergen, Department of Global Health and Primary Care, Centre for International Health and Norwegian Centre for Violence and Traumatic Stress Studies (NKVTS). Ane-Marthe Solheim Skar, MA Psychology, PhD. Norwegian University of Science and Technology (NTNU), Department of Mental Health, Faculty of Medicine and Health Sciences, Regional Centre for Child and Youth Mental Health and Child Welfare: Norbert Skokauskas, MD, PhD Professor, Child and Adolescent Psychiatry. Victoria Bakken, MSc Health Psychology. Norwegian University of Science and Technology (NTNU), Faculty of Medicine and Health Sciences: Silje Akselberg Iversen, Medical Student. Divya Rayamajhi, Stud. MA Public Health.
Contributors JNB and IMSE are co-principal investigators. VS, HA, VB, JD, M-JK, JSN, DS, AMSS, NS, HW, IMSE and JNB contributed to the original protocol which formed the basis for this manuscript. HA, JN, EK, DS, JNB organised the data collection to date. VS, HA, IMSE and JNB led the writing of the manuscript for publication. VS and HA have shared first authorship and IMSE and JNB have shared last authorship. All authors contributed to the review of the manuscript for publication.
Funding This work was supported by The Norwegian Research Council, the GLOBVAC-programme with the project grant number 285 489.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.