Article Text

Abstract
Objectives This systematic review aims to identify the secondary attack rates (SAR) to adults and other children when children are the index cases within household settings.
Methods This literature review assessed European-based studies published in Medline and Embase between January 2020 and January 2022 that assessed the secondary transmission of SARS-CoV-2 within household settings. The inclusion criteria were based on the Population, Exposure, Outcome framework for systematic reviews. Thus, the study population was restricted to humans within the household setting in Europe (population), in contact with paediatric index cases 1–17 years old (exposure) that led to the transmission of SARS-CoV-2 reported as either an SAR or the probability of onward infection (outcome).
Results Of 1819 studies originally identified, 19 met the inclusion criteria. Overall, the SAR ranged from 13% to 75% in 15 studies, while there was no evidence of secondary transmission from children to other household members in one study. Evidence indicated that asymptomatic SARS-CoV-2 index cases also have a lower SAR than those with symptoms and that younger children may have a lower SAR than adolescents (>12 years old) within household settings.
Conclusions SARS-CoV-2 secondary transmission from paediatric index cases ranged from 0% to 75%, within household settings between January 2020 and January 2022, with differences noted by age and by symptomatic/asymptomatic status of the index case. Given the anticipated endemic circulation of SARS-CoV-2, continued monitoring and assessment of household transmission is necessary.
- COVID-19
- epidemiology
- virology
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Previous research suggests that children are less frequently the index cases and are more likely to get infected by an adult.
WHAT THIS STUDY ADDS
Overall, the secondary attack rate (SAR) ranged from 13% to 75%. Asymptomatic SARS-CoV-2 index cases had a lower SAR than symptomatic and younger children may have a lower SAR than adolescents (>12 years old).
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our results may facilitate policy decision-making on possible future pandemics.
Introduction
At the time of this review, Epidemiological data on SARS-CoV-2 indicate that children are less prone to get infected by COVID-19 and, when infected, the clinical characteristics are less severe than those in adults.1 Virological studies of SARS-CoV-2, Middle East respiratory syndrome-CoV and SARS-CoV also suggest that children are less likely to develop serious illness following infection compared with adults.1 A significant area of respiratory research relates to the ability of infected children to infect others.2 3 Previous research suggests that children are less frequently the index cases in both the household and school setting and are more likely to get infected by an adult.4 Higher rates of transmission have also been previously observed in older children (10–19 years old) in comparison to younger children (<10 years old).5
To prevent the spread of COVID-19, social distancing policies within the first waves of the pandemic were instated, leading to the closure of educational settings within some countries and the requirement that children remain within households. In order to better understand the role of children in the transmission of SARS-CoV-2 outside the school setting, it is important to understand how SARS-CoV-2 was transferred within households during the COVID-19 pandemic. This would then be able to build the evidence for public health emergency preparedness actions for future pandemics in Europe.6
The aim of this systematic review is to identify the secondary attack rates (SAR) of adults and other children when children are the index cases within households in Europe up to January 2022.
Methods
Search strategy and selection criteria
A systematic literature review was performed in January 2022 according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.7 Relevant peer-reviewed studies were identified through systematic electronic searches using the OVID Medline and EMBASE databases. The complete search strategy and search terms are available in online supplemental table 1.
Supplemental material
The following set of inclusion criteria, based on adapted versions of the Population, Exposure, Outcome framework for systematic reviews,8 was used to identify relevant studies and determine their eligibility for inclusion and are:
Population: Humans, of any age within a household setting. The household setting includes cohabiting individuals, including family members, close relatives or housemates.
Exposure: Index cases, aged 0–17 years, defined as the first individual with laboratory-confirmed SARS-CoV-2 to develop symptoms or test positive within a household setting. Studies or reports that solely address non-household transmission were excluded.
Outcome: Transmission of SARS-CoV-2 reported as either SAR (probability of onward infection from an index case among a defined group of close contacts), or observed reproduction number (R, observed average number of secondary cases per index case).
Geographical Context: Europe, European Union (EU), UK and European Economic Area (EEA) countries.
Study designs: All study types were considered, including descriptive studies, outbreak-cluster investigation reports and contact tracing investigations. Systematic reviews and non-systematic reviews were identified, and references were screened for eligible studies. Opinion pieces and commentaries were excluded.
Time frame: 1 January 2020 to 20 January 2022.
Data analysis, extraction, tabulation and quality appraisal
Studies identified from the searches were uploaded into a bibliographic database, and duplicates were removed. Initially, a pilot training screening process was used, where a random sample of 100 titles was screened for eligibility independently by two reviewers (KA, AK) to enable consistency in screening and identify areas for amendments in the inclusion criteria. A high measure of inter-rater agreement was achieved (percentage agreement >80%), and hence the remaining titles were equally distributed between the two reviewers and screened independently. Any disagreements were thoroughly discussed with a third reviewer (CIV). For the full-text screening, a similar process was followed. Ten randomly selected studies were independently screened for eligibility by two reviewers (KA, AK) for the level of agreement to be estimated (percentage agreement >90%). The remaining full texts were equally distributed and screened by the two reviewers (KA and AK). A data extraction template was independently piloted by two reviewers on a random sample of five included studies to assess consistency in data extraction and identify where amendments need to be made to the template. The remaining studies were then data extracted independently by the two reviewers (KA and AK). Extracted data included study characteristics (first author’s name, year of publication), geographical context (country/area), methodology/study type, time frame, setting (where the measures were implemented), COVID-19 diagnosis, contact tracing, SARS-CoV-2 strain, the non-pharmaceutical interventions (NPIs) implemented, follow-up process, population characteristics (age, gender, geographical location) and objective and quantitative results with regard to transmission between children and/or transmission from children to adults, including SAR and ORs.
The Joanna Briggs Institute standardised critical appraisal tools were used for cohort studies, cross-sectional studies, case reports and case series.9
A narrative synthesis approach was followed, while where patterns in the data were identified through tabulation of results, an inductive approach (where concepts were derived from the data) was taken to translate the data to identify areas of commonality between studies. Where results are presented graphically, standard errors were either entered as reported or imputed based on the medians of the reported standard errors.
Patient and public involvement
This study was performed under contract for the European Center for Disease Prevention and Control (ECDC). Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
Results
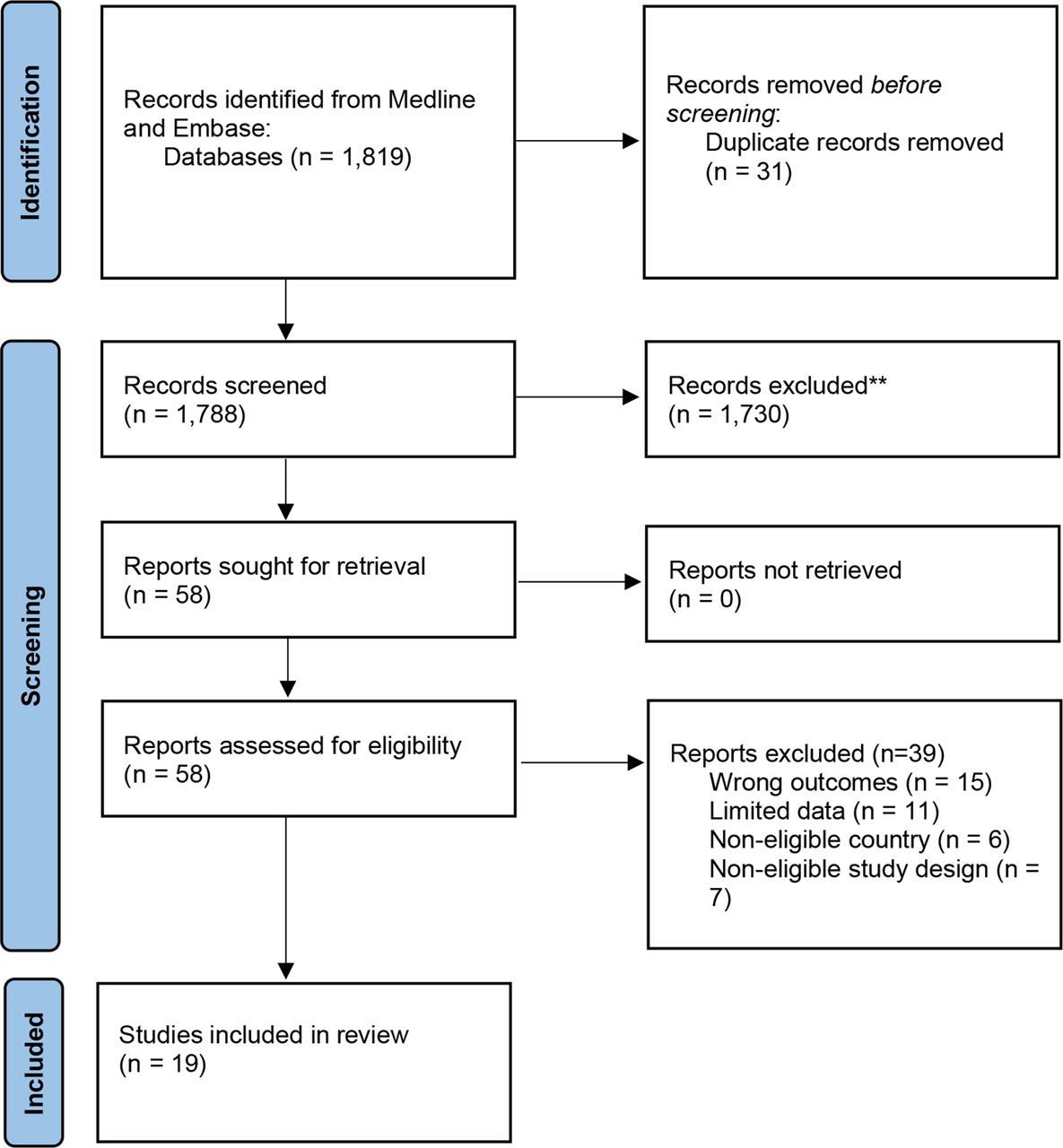
A total number of 1819 studies were identified according to the specified selection criteria from the two databases. After removing duplicates, 1788 were screened by title/abstract of which, 58 were assessed via full text. Of these 58 studies, 39 were excluded due to limited data, limited outcomes of interest, non-eligible geographical area and irrelevant study type (reviews, conference abstracts, opinion papers). Hence, 19 studies were eventually considered in our analysis. The flow chart of study selection is presented below in figure 1.
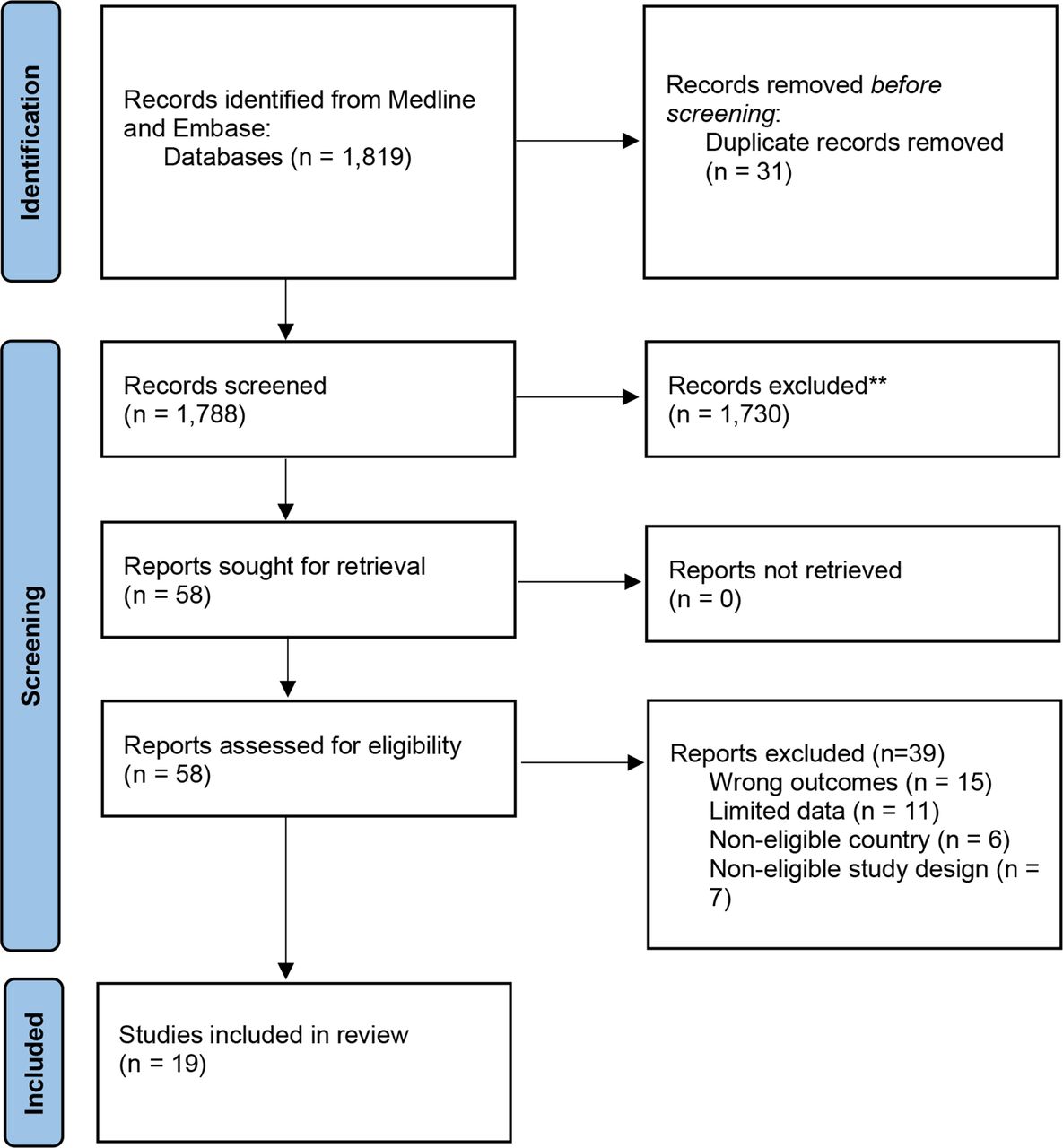
Flow chart of study selection.
Of the 19 studies, 11 were cohort studies,10–20 4 were cross-sectional,21–242 were case reports,25 26 1 was a case series27 and one was a case–control.28 Real-time PCR (RT-PCR) was used in 10 studies to diagnose COVID-19. In five studies, serology tests were performed in addition to or instead of RT-PCR,11 19 24 25 28 while in onestudy, nucleic acid amplification test was reported as the single diagnostic method for SARS-CoV-2 detection.21 Regarding NPIs, case isolation and quarantine of contacts were the most frequently reported measures and implemented in parallel with the contact tracing investigations for mitigating/suppressing SARS-CoV-2 transmission during the pandemic. These features along with the geographical area of the study are summarised in online supplemental table 2. The quality assessment of the included articles is available within online supplemental file 3, which in principle indicated that the vast majority of studies were of high quality with regard to the research question we assessed, with points predominantly lost due to the unclear reporting of follow-up time and strategies.
Child to adult/child SARS-CoV-2 transmission in the household setting
Of the 19 studies included in the analysis, 15 provided adequate contact tracing data for estimating the SAR from paediatric index cases to adult and/or child household contacts (table 1). Overall, SAR ranged from 13% to 75% in 14 studies, while only in one small study there was no evidence of secondary transmission from children to other household members.16 The highest SARs (67% and 75%) were found in studies examining single-family clusters with symptomatic paediatric index cases.25 26 In studies where an age stratification was performed (n=6 studies), higher SARs were mostly noted from adolescents (>12 years old)17 22 23 28 compared with younger ages, except for two studies, the results of which indicated higher SAR from children 0–11 years old.10 20
Assessment of secondary attack rates from paediatric index cases
The highest SAR was found in the study of Abbas and Törnhage,25 tracing one family cluster residing in Sweden. Among the four family contacts of the paediatric index case, three secondary infections occurred, with the SAR hence estimated at 75% within this family cluster. A high SAR was also found in a family cluster from Ireland, as described by Hare et al,26 where SARS-CoV-2 was transmitted from one symptomatic paediatric index case to six of nine household contacts, leading to an SAR of 67% (95% CI 35% to 88%). A slightly decreased SAR of 59.0% was presented by Soriano-Arandes et al19 in a study performed in Catalonia, Spain with 80 paediatric index cases, 67 of which were symptomatic and transmitted SARS-CoV-2 to 167 out of 283 household contacts.
A more meticulous approach for SAR based on age stratification was provided by six studies. Calvani et al28 performed a case–control study to investigate 70 paediatric cases, 28 of which were reported as index cases in their households. The overall SAR from children to household members was estimated at 30.6% (95% CI 20.2% to 42.5%), while the highest SAR was found in the ages of 0–5 (33.3%) and 11–19 years old (35.3%) compared with index cases aged 6–10 years old (23.1%). The study also showed that the 80% of symptomatic paediatric index cases spread the virus to their family members compared with 26.7% for asymptomatic paediatric index cases (SAR: 36.6% vs 22.6%, respectively).
The predicted SAR in 77 exposed household members was lower when the index case-patient was <12 years of age (SAR=12.0% (95% CI: 0.59% to 11.4%)) and higher with an index case-patient 12–17.9 years of age (SAR=30.8% (95% CI: 3.11% to 55.9%)).23 Compared with the previous findings, Bistaraki et al,10 who studied 1837 paediatric index cases, estimated a higher SAR from children at the age of 0–11 years (SAR=25% (95% CI: 22.2% to 28%)) compared with adolescents (SAR=15.4% (95% CI: 13.9% to 17.1%)). Likewise, in the study by Telle et al,20 SAR was 24% (95% CI: 20% to 28%) when the index was a child aged 0–6 years and declined with increasing age of the index child, with the lowest SAR (11%, 95% CI: 10% to 13%) found when a child aged 17–20 was the index case.
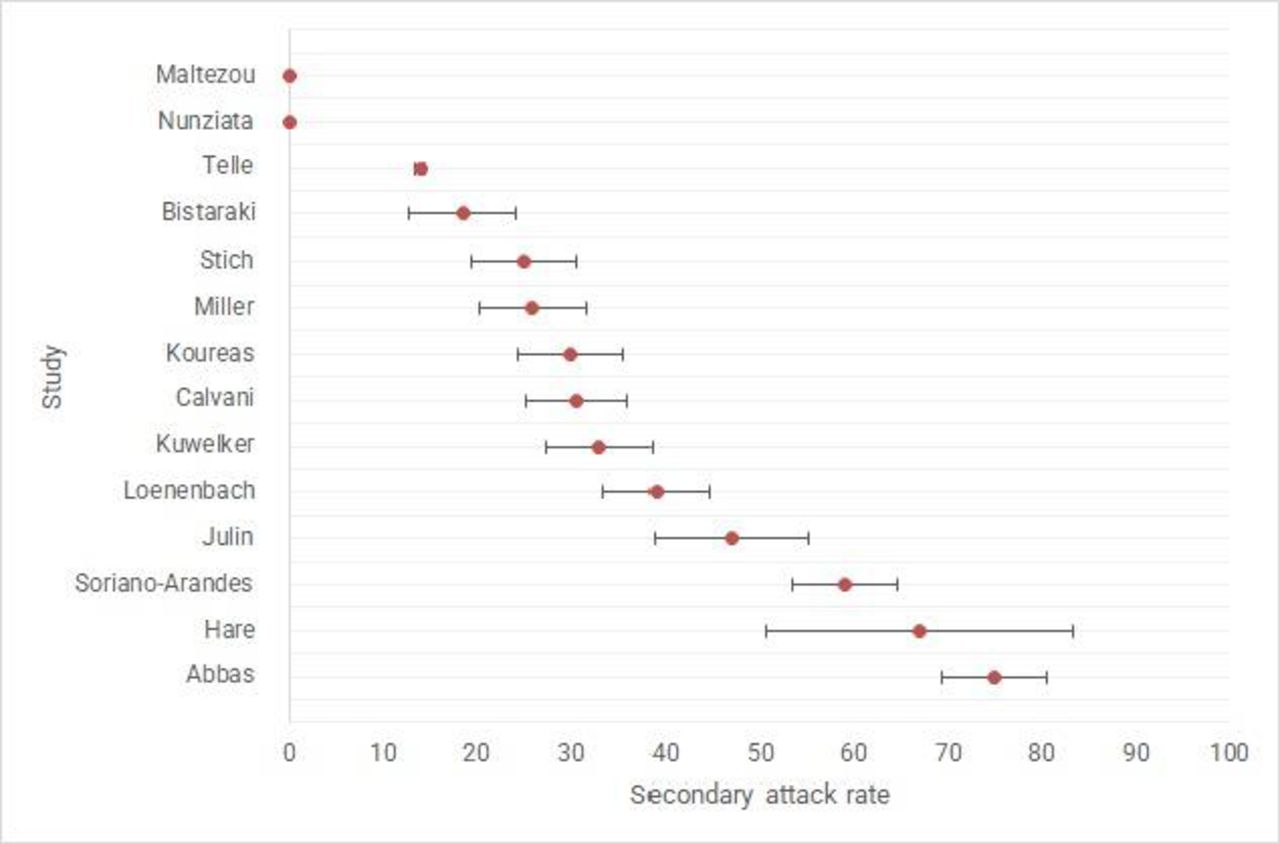
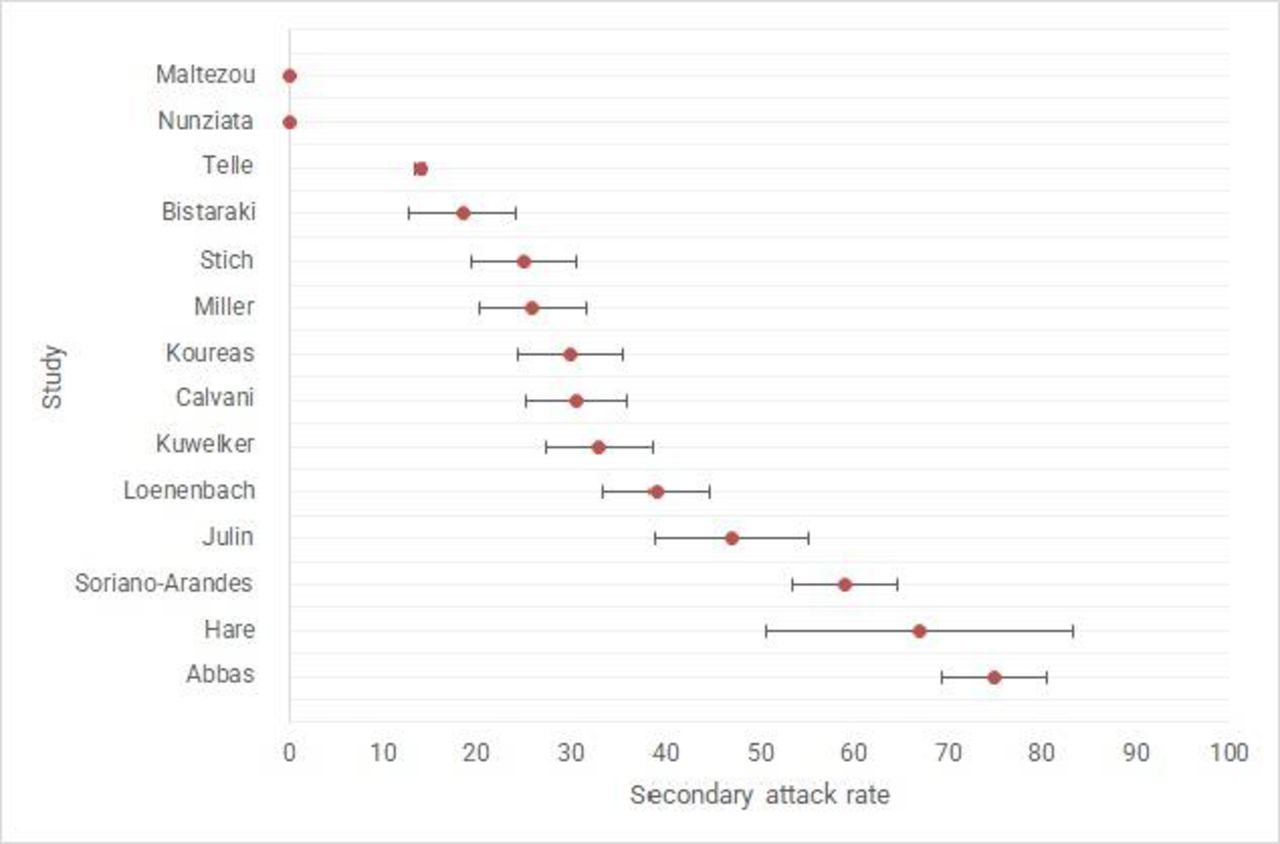
The lowest SARs, ranging from 13% to 15% were detected by Charbonnier et al11 and Galow et al,12 while Maltezou et al15 found no secondary SARS-CoV transmission from paediatric index cases. Similarly, in the study published by Maltezou et al16 none of the six paediatric index cases from 23 family clusters transmitted SARS-CoV-2 to any of the household contacts, while children were more likely to have an asymptomatic SARS-CoV-2 infection compared with adults (40% vs 10.5%; p=0.021) and were significantly more likely to have a low viral load. Figure 2 provides a graphical overview of the SAR when children are the index cases for studies which had available data reported as percentages and provided information on the SEs.
{kind=link}
{kind=link}
Graphical overview of the studies reporting a secondary attack rate (SAR) in European households when children are the index case.
Information on the frequency of pediatric index cases in household settings
The evidence on the frequency of paediatric index cases in household settings is detailed in table 2. The highest proportion of paediatric index cases was detected in the studies conducted by Chudasama et al,24 Loenenbach et al,13 Miller et al17 and Maltezoy et al,16 ranging from 47% to 59%. Chudasama et al24 found 13 215 paediatric index cases in a total number of 22 538 households, of whom 5476 were at the age of 5–11 years and 7739 at the age of 12–15 years. The authors reported that the proportion of household clusters where a child (aged 5–15 years) was identified as the index case remained similar over the summer of 2021. Similarly, Loenenbach et al13 conducted contact tracing among 38 households in which, 22 households had children who developed symptoms of COVID-19 and were assumed as the suspected index cases. Maltezou et al15 also investigated 187 index cases among 133 family clusters of which 62 were paediatric cases. Of these 62 children, 51 had no other family member with a SARS-CoV-2 infection, one child had an unknown family history and 10 children had at least one family member with a SARS-CoV-2 infection.
Study characteristics and results for studies with childrenas index cases
A lower proportion of paediatric index cases was found in the study of Telle et al,20 who included 7548 index cases, among which 4964 were parents (66%) and 2584 children (34%). From those 2584 children, the number of index cases increased steeply with age, from 200 (8% of child index cases) among the youngest (aged 0–6) to 1086 (42% of child index cases) among the oldest (aged 17–20). An increasing number of index cases with age was also noted by Koureas et al,22 who reported three index cases younger than 12 years old and six at the age of 13–19 years. An estimated percentage of approximately 25% paediatric index cases was found in the samples of Maltezou et al15 in 23 family clusters. In the remaining eight studies children were less frequently reported as index cases. Lyngse et al14 investigated SARS-CoV-2 variant B.1.1.7 (Alpha variant) and other lineages and found among 8093 primary household cases, 1293 were children and adolescents of which 145 were diagnosed with the Alpha variant. The same variant was also detected in two out of three paediatric primary cases from 65 households in the study of Julin et al.29 Finally, among the lowest proportions of paediatric index cases were found by Stich et al23 (25/405 households) and by Kuwelker et al27 (2/112 index cases). In the study by Stich et al23 adolescents were more frequently reported as index cases compared with younger children, like in all other studies where an age stratification was performed.
Discussion
This systematic review provides an assessment of the peer-reviewed literature pertaining to SARS-CoV-2 transmission when children are the index case, within the household setting in the European context. The literature appraised in this review provides sufficient evidence that children less than 12 years old are less frequently reported as index cases in their households compared with adults, with adolescents showing a higher frequency of being the index case among the included studies than children under 11 years of age. This finding is corroborated by research published before the cut-off date of this review, estimating the overall weighted prevalence of parents being the index case of COVID-19 at 54%.30
Regarding the transmissibility of SARS-CoV-2 from children to other household members, the SARs detected in the studies of this review ranged between 13% and 75%. OOne smaller study showed no secondary transmission from child index cases—a result which may be partially attributable to the in-parallel implemented NPIs at the time of the study, while those with substantially higher SAR were predominantely small family cluster studies and hance may lack generalisability to larger populations.16 31 This high variability in the SAR is expected across studies as the different study design, geographical setting, implemented NPIs and circulating variants all effect transmission patterns and increase variability across studies hence limiting our confidence in the generalisability of the results if we were to perform a meta-analysis. However, our results are similar to a recent meta-analysis with a more global scope, which estimated the SAR of child index cases at 20% (95% CI 15% to 26%, I2=100%), and indicated that child index cases were significantly associated with a lower possibility to transmit SARS-CoV-2 to their family members (RR=0.64, 95% CI: 0.50 to 0.81, I2=96%) compared with the adult index cases.32 A previous review also presented pooled estimates of an overall SAR from children at 10% (95%: CI 3% to 25%), and identified a lower child-to-child transmission rate at 5.7%, whereas the child-to-adult transmission rate was 26.4%.33 With regard to the differences noted between the estimated SARs of these reviews, it should be taken into account that emerging SARS-CoV-2 variants of concern have increased transmissibility, population vaccination rates have increased,34 and NPIs can be implemented differently across countries, which may explain differences in the identified SARs by setting. It is further interesting to note that children under 12 have lower vaccination rates compared with adults, on average, according to the EU vaccine tracker—a fact which may further influence household transmission.35
There is evidence of differing transmission dynamics between younger versus older children, for example, index cases under 11 years of age lead to lower SARs than older children. Moreover, although children appear to be at lower risk for symptomatic disease, symptomatic index cases had significantly higher SAR compared with asymptomatic index cases. Our results align with those of Chen et al32 where symptomatic index cases were associated with a higher SAR than asymptomatic index cases.32
Apart from the role of the child’s age in the household transmission of SARS-CoV-2, there are also environmental and behavioural factors which might facilitate or prevent secondary infections, including, but not limited to, the number of household members, the number of people per room, non-compliance with isolation requirements, sharing of index case’s bedroom, sharing of meals, as well as the level of adherence to face mask wearing.36 37 Finally, the current review identified a higher SAR within households when compared with the results of our previous review that assessed the transmission in educational settings, which noted limited cases of extensive secondary transmission in schools, especially when social distancing measures, face masks and adequate ventilation were implemented.6 34
Strengths and limitations
There are limitations to this study that may impact the implications for decision-making. As we assessed peer-reviewed evidence published in two biomedical databases, it inherently reflects the status quo of the interim of the years (2020–2021) due to the lag time between study implementation, peer review and publication. Moreover, we report on studies that represent child-to-child/adult transmission within the context of initial SARS-CoV-2 strains and are not directly applicable to newer variants, such as the SARS-CoV-2 Delta or Omicron variant. Although we restricted studies to only those that were located within the EU/UK/EEA region so as to enhance comparability, the household transmission may also be influenced by other factors such as background levels of community SARS-CoV-2 transmission, the transmission of SARS-CoV-2 in educational settings6 and varying NPI policies. Another matter of inconsistency is the different definitions of primary and index cases used in the included studies, as well as the various methods used for the identification of index cases, the contact tracing process and the follow-up duration—mostly due to differences in study design, did not allow up to perform a meta-analysis. Supporting educators and parents in the implementation of NPIs may be important as population-based studies have indicated that adults concerned about the impact of COVID-19 on their children’s education may be more likely to practice personal protective measures and social distancing.38
Conclusion
According to the findings of studies that have been published up until January 2022, which in principle represent evidence from the first 2 years of the pandemic, the role of children in COVID-19 transmission within the household setting in the European region was notable, but higher than SARs noted in educational settings. Moreover, there was an indication that younger children may have a lower SAR than adolescents within household settings. Moreover, symptomatic paediatric index cases had significantly higher SAR than asymptomatic index cases. However, there were insufficient data to examine how the transmissibility of paediatric index cases is affected by different SARS-CoV-2 variants as well as the effect of vaccination on the spread of SARS-CoV-2 within the household setting. Given the potential endemic circulation of SARS-CoV-2, continued monitoring and assessment of household transmission is necessary.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to thank Katerina Papathanasaki (UoC), Chrysa Chatzopoulou (UoC) and Konstantinos Skouloudakis (UoC) for their assistance in data archiving.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors CIV, JL-B, RP and JES designed the study. KN, KA and AK undertook the literature review and extracted the data. JL-B and RP developed the search code. CIV, IA, KA, KN and NPR analysed and interpreted the data. IA created the figures, EF and ES participated in data evaluation and interpretation along with JL-B, JES, OC, FL and CD. CIV wrote the first draft of the manuscript with input from all authors. JES, CD, OC, RP and FL along with all other authors reviewed and revised subsequent drafts. CIV acts as the guarantor.
Funding This report was commissioned by the European Centre for Disease Prevention and Control (ECDC) to the PREP-EU Consortium, coordinated by CIV (School of Medicine, University of Crete) under Framework contract ECDC/2019/001 Lot 1B.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.