Article Text

Abstract
Background There is a lack of consensus regarding the definition and treatment threshold for neonatal hypoglycaemia. The American Academy of Pediatrics (AAP) has a published clinical report making recommendations on practice guidelines. There is limited literature discussing the impact of these guidelines. In this study, we evaluated the screening and diagnosis of neonatal hypoglycaemia following the AAP guidelines.
Methods Infants born ≥35 weeks gestational age and admitted to the well–baby nursery between January and December 2017 were included in this study. Our hypoglycaemia policy was based on the AAP clinical report for hypoglycaemia management in newborns. Chart review was done to obtain infant hypoglycaemia risk factors and blood glucose values in the first 24 hours. Data analysis was conducted using Stata V.14.2 (StataCorp).
Results Of 2873 infants born and admitted to the well–baby nursery, 32% had at least one hypoglycaemia risk factor and 96% of them were screened for hypoglycaemia. Screened infants were more likely to be born at a lower gestational age, via C-section, and to a multiparous older mother. Screened infants and hypoglycaemic infants had lower exclusive breastfeeding rates compared with those who were not screened or not hypoglycaemic, respectively. Sixteen per cent of screened infants were diagnosed with hypoglycaemia; 0.8% of at-risk screened infants and 5% of hypoglycaemic infants were admitted to the NICU for treatment of hypoglycaemia. Thirty-one per cent of preterm infants, 15% of large for gestational age infants, 13% of small for gestational age infants and 15% of infants of diabetic mothers were hypoglycaemic. Hypoglycaemic infants were more likely to be born preterm and via C-section.
Conclusion Using the AAP time-based definitional blood glucose cut-off values, our incidence of hypoglycaemia found in those who were screened for risk factors was lower compared with other studies. Future long-term follow-up studies will be important.
- Neonatology
Data availability statement
Data are available on reasonable request. Deidentified participant data as well as our institutional hypoglycaemia policy are available on request from the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Neonatal hypoglycaemia can lead to potential long-term neurodevelopmental sequelae. Many institutions have a hypoglycaemia guideline/policy. There is a lack of consensus regarding the definition and treatment threshold for neonatal hypoglycaemia, however, the American Academy of Pediatrics (AAP) has published its clinical report making recommendations on practice guidelines for the screening, diagnosis and treatment of hypoglycaemia.
WHAT THIS STUDY ADDS
This study showed that in our institution, following the AAP guidelines, the incidence of hypoglycaemia in screened at-risk infants was 16% and NICU admissions were <1%. This information is important to the paediatric community caring for newborns because our incidence of hypoglycaemia was lower than compared with other studies who used higher cut-off values, therefore, resulting in fewer babies being treated for hypoglycaemia and a lower mother–infant separation due to hypoglycaemia.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Using the AAP time-based definitional blood glucose cut-off values may result in a lower incidence of neonatal hypoglycaemia and lower mother–infant separation rate. Future long-term follow-up studies will be important.
Introduction
Transitional hypoglycaemia within 48 hours after birth is common in healthy newborns as the body’s metabolism adjusts postnatally.1 However, prolonged hypoglycaemia is associated with concerns for neurological morbidity.2 3 Controversy remains regarding the definition of hypoglycaemia and threshold for treatment in asymptomatic newborns.4 We published a survey in 2021 reporting notable variation among 84 participating US hospitals for the definition of hypoglycaemia, threshold for treatment and criteria for NICU admission.5 The American Academy of Pediatrics (AAP) published a clinical report in 2011 with guidelines for blood glucose screening and treatment.6 The AAP advocates screening babies with risk factors including small for gestational age (SGA), large for gestational age (LGA), infant of diabetic mothers (IDM), late preterm infants (LPI, gestational age <37 weeks) and newborns with symptoms (including jitteriness, cyanosis, seizures, apnoea, tachypnoea, weak or high-pitched cry, floppiness, lethargy and poor feeding). Moreover, AAP defines diagnosis of hypoglycaemia as glucose <40 mg/dL in the first 4 hours of life or <45 mg/dL 4–24 hours of life and recommends hypoglycaemia treatment intervention at <25 mg/dL in the first 4 hours of life or <35 mg/dL between 4 and 24 hours of life.6 However, many published studies use higher definitional values for hypoglycaemia (<47 mg/dL or<50 mg/dL).7–9
Repeated and potentially unnecessary blood glucose monitoring in asymptomatic newborns presents the risk of pain, risk for infection, interruption of breast feeding, increased parental anxiety and increased hospital costs.7 10 The definition of hypoglycaemia and threshold for treatment in asymptomatic newborns affects mother–infant separation (NICU admission) rates.10 The AAP guideline accounts for transient hypoglycaemia in newborns and includes a range of glucose levels at different times to specifically identify prolonged hypoglycaemia and recommends checking the first glucose value only after the first feed, taking into consideration the natural transient hypoglycaemia after birth, which supported by a published study measuring glucose values after feeds in IDM infants.11 However, there is limited evidence evaluating the implementation of the AAP guidelines6 for diagnosis and treatment of neonatal hypoglycaemia.9 12 Hypoglycaemia protocols based on risk factors, with time sensitive thresholds for diagnosis and treatment of neonatal hypoglycaemia, may decrease the number of infants being diagnosed with hypoglycaemia and requiring NICU admissions.
The objective of this study is to evaluate the characteristics associated with the screening and diagnosis of neonatal hypoglycaemia in asymptomatic at-risk newborns, using the AAP recommended guidelines.
Methods
Setting and study design
This was a single centre retrospective observational study at a public safety-net hospital with ~3000 deliveries per year and a 40-bed AAP Level IV NICU. Paediatric hospitalists or paediatricians care for well babies with neonatology oversight of policies and procedures. The hospital received Baby-Friendly Hospital Designation in January 2019.
Patient and public involvement
Patients were not involved in the design, recruitment to or conduct of the study.
Patient population
Infants born ≥35 weeks gestation and admitted to our Mother Infant Care Centre (MICC) well–baby nursery between January and December 2017 were included in this study. Infants were excluded if admitted directly to the NICU for reasons other than hypoglycaemia or neonatal death occurred.
Data collection
Charts were retrospectively reviewed for each infant that met inclusion criteria. Infants were determined to be SGA or LGA if their birth weight was less than 10th percentile or greater than 90th percentile for their gestational age based on 2013 Fenton growth chart, respectively. The number of blood glucose tests and the glucose values within the first 24 hours were recorded. All the data was collected as part of an initial quality improvement project and IRB approval was obtained to retrospectively analyze the data. Maternal diabetes status data were obtained from maternal information which flows into infants’ charts to determine IDM status. Birth weight, gestational age, method of birth and feeding type (breast milk or formula) were collected from a report from the electronic health record.
Definition and treatment of hypoglycaemia
Our hypoglycaemia policy was developed based on the AAP clinical report for hypoglycaemia management in newborns.6 Risk factors for hypoglycaemia included SGA, LGA, LPI and IDM. Infants were determined to be hypoglycaemic if glucose levels were <40 mg/dL in the first 4 hours of life or <45 mg/dL 4–24 hours of life. Treatment for hypoglycaemia was indicated if glucose levels were <25 mg/dL in the first 4 hours of life or <35 mg/dL 4–24 hours of life. Our initial intervention for treating hypoglycaemia included breast feeding, expressed breast milk or formula feeding prior to initiating dextrose containing intravenous fluids. If glucose levels were <15 mg/dL at any point, infants were fed and transferred to NICU to receive dextrose containing intravenous fluids. While the AAP guidelines recommend continue screening SGA and LPI infants for 24 hours and LGA and IDM infants for 12 hours, our hypoglycaemia policy stopped screening once three normal glucose values were obtained. Blood glucose was measured as point-of-care testing using Accu-Chek Inform II (Roche Diagnostics, Germany). Samples were sent to lab if they were outside the range listed according to the operations manual.
Data analysis
Data were summarised using descriptive statistics. We compared demographics and hypoglycaemia risk factors between infants who were screened and not screened and in infants who were diagnosed with hypoglycaemia with infants who were not. χ2 or Fisher’s exact test was used to compare categorical variables and t-test or ranksum was used to compare continuous variables. Data were adjusted for C-section or gestational age as appropriate. Data analysis was conducted using Stata V.14.2 (StataCorp).
Results
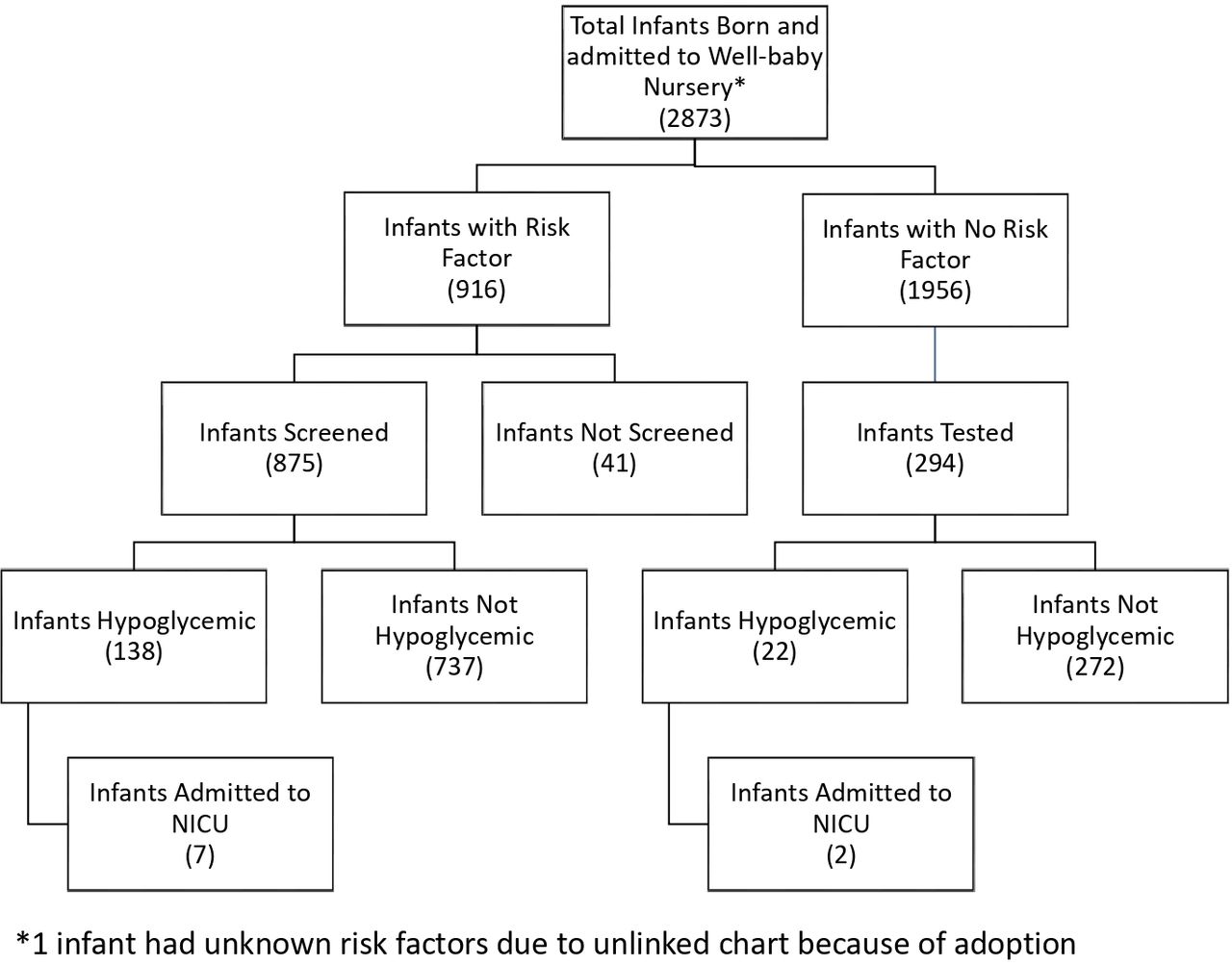
During the study period, 2873 infants were born and admitted to MICC. Flow chart of participants in the study is presented in figure 1. Maternal and infant characteristics are presented in table 1. Of the 2873 infants, 31.9% had at least one risk factor for hypoglycaemia (SGA, LGA, LPI or IDM) and 5% had more than one risk factor. Of those with at least one risk factor, 96% were screened for hypoglycaemia. Of the 4% of at-risk infants not screened for hypoglycaemia, 36 infants were SGA and 3 infants were both LGA and IDM. Screened infants were born at a lower gestational age, via C-section, and to a multiparous older mother. Infants who were screened had a lower percentage of delayed cord clamping >60 s (table 1). The median number of blood glucose screens per infant was 3. However, 18% (160/875) of at-risk infants were screened more than 3 times in the first 24 hours of life, 83% (132/160) of whom were diagnosed with hypoglycaemia and 4% (7/160) were admitted to the NICU (Neonatal Intensive Care Unit) for hypoglycaemia treatment.
Maternal and infant characteristics of all and screened infants
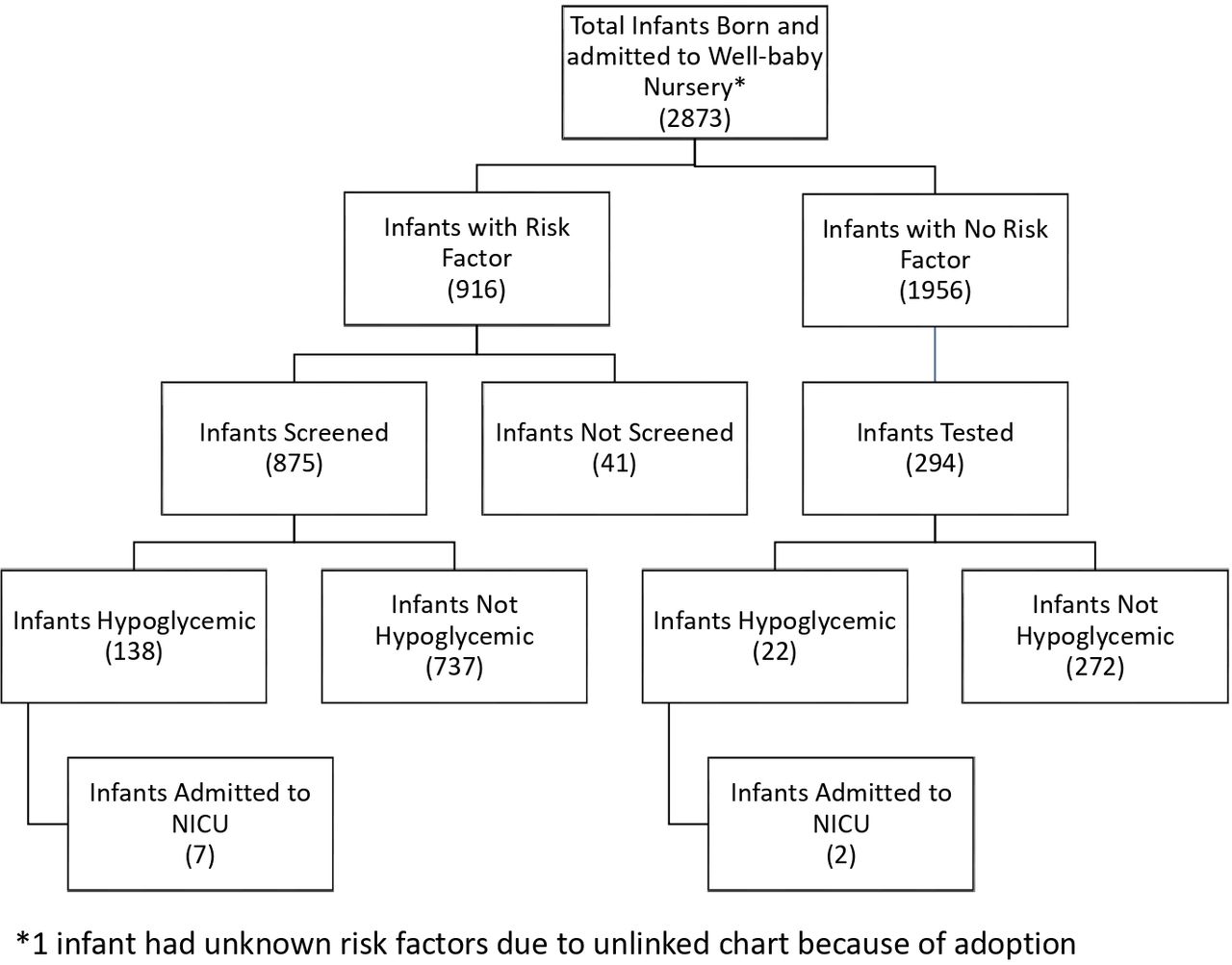
Study cohort flow diagram.
Sixteen per cent of at-risk screened infants were diagnosed with hypoglycaemia; 69% (95/138) of them were diagnosed with hypoglycaemia <4 hours of age. All 138 infants with hypoglycaemia were identified within the first 3 glucose measurements, with 64% (88/138) identified on the first glucose check and 84% (116/138) identified within the first 2 glucose checks. Thirty-one per cent (36/117) of preterm infants, 15% (30/202) of LGA infants, 13% (26/197) of SGA infants and 15% (81/553) of IDM infants were hypoglycaemic. There was no difference in the per cent of infants with hypoglycaemia when stratifying prematurity to 35 weeks (30%) or 36 weeks (31%). Thirty per cent (166/554) of diabetic mothers were on insulin and 20% (33/166) of their infants had hypoglycaemia compared with 12% (48/388) of infants born to diabetic mothers not on insulin (p=0.022). C-section births were associated with higher risk for hypoglycaemia, even after adjusting for gestational age. Prematurity and multiple hypoglycaemia risk factors were associated with higher risk of hypoglycaemia even after adjusting for C-section (table 2).
Maternal and infant characteristics of hypoglycaemic infants
Seven per cent of infants without risk factors were diagnosed with hypoglycaemia after being tested for various reasons, including 64% due to symptoms (jitteriness, respiratory distress, hypothermia) (figure 1). A total of 6% (161/2873) of all infants were diagnosed with hypoglycaemia.
Five per cent of hypoglycaemic infants were admitted to the NICU for hypoglycaemia treatment. In this study, 0.8% of screened at-risk infants and 0.3% of all infants in MICC were admitted to the NICU for hypoglycaemia treatment (table 2). Of the seven screened at-risk infants who were admitted to the NICU for hypoglycaemia, six infants were identified as having hypoglycaemia within the first two glucose measurements.
Screened infants had a lower exclusive breastfeeding rate (49%) compared with those who were not screened (65%) (table 1), which persisted even after adjusting for C-section, IDM and gestational age. Hypoglycaemic infants had lower exclusive breast feeding (33%) compared with non-hypoglycaemic infants (53%), even after adjusting for C-section (table 2).
The time of the first glucose check in screened at-risk infants was 1.4 hours of life (table 3). The time of first glucose check in LGA infants, IDM and infants born via C-section was lower compared with non-LGA infants, non-IDM and infants born vaginally, respectively. However, the time of first glucose check in SGA infants was higher than non-SGA infants. The time of first glucose check in hypoglycaemic infants was significantly lower compared with infants not diagnosed with hypoglycaemia.
First glucose age and value
The first median glucose value in those screened was 55 mg/dL (table 3). The first glucose value was similar between IDM and non-IDM infants and LGA and non-LGA infants but significantly lower in preterm infants and infants born via C-section. There was no significant difference in the first glucose values between IDM infants born to mothers on insulin and mothers not on insulin (54 vs 54 mg/dL). The first glucose value was higher in SGA infants (59 vs 54 mg/dL), although not clinically significant. The first glucose value in hypoglycaemic infants and non-hypoglycaemic infants was 38 vs 57 mg/dL.
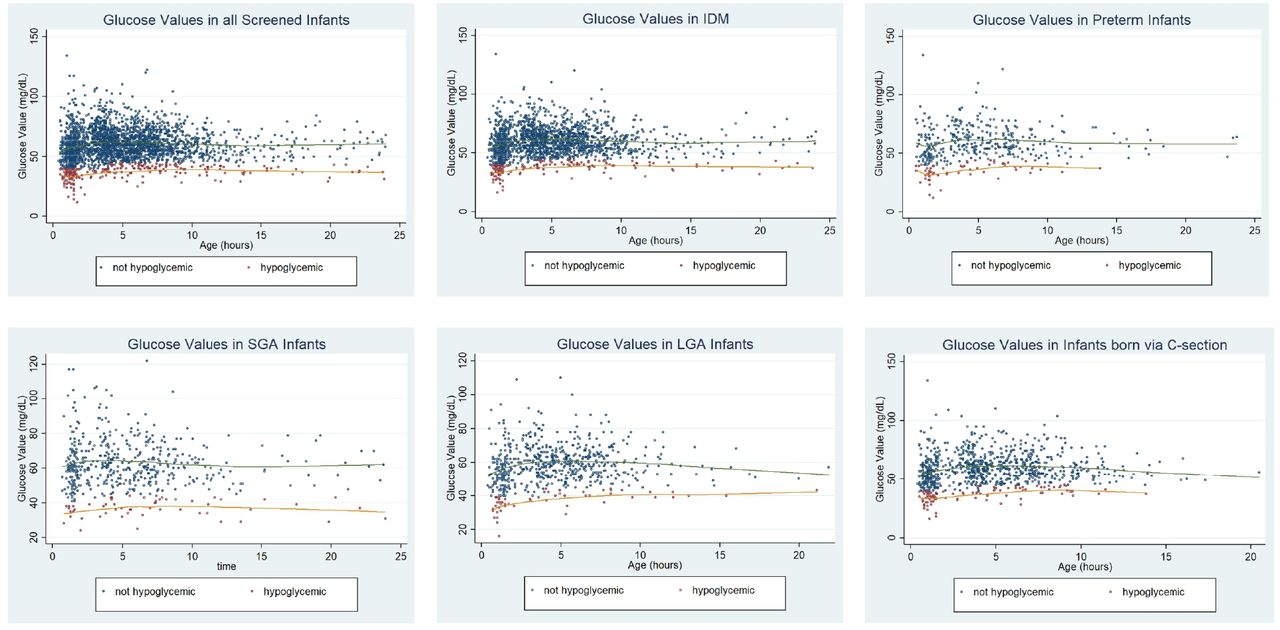
We collected 2856 glucose values from the charts of at-risk screened infants in the first 24 hours. The scatter plots of the glucose values are presented in figure 2. Of all the values collected, 8.6% were below threshold for hypoglycaemia (11% in SGA, 15% in preterm, 8.6% in LGA, 8.1% in IDM and 11% in C-section infants). Only five glucose values were below threshold after 12 hours of age originating from four infants (one IDM, two SGA, one LPI). All four infants except one SGA infant had a previous hypoglycaemic episode <4 hours of age. The one SGA infant who did not have a previous hypoglycaemic episode had two hypoglycaemic episodes at 22 and 23.9 hours of age (no screen done between 1.5 and 22 hours of age).

{kind=link}
{kind=link}
Scatter plots of glucose values in the first 24 hours. LOWESS (locally weighted Scatterplot smoothing) lines for not hypoglycaemic values are presented in green. LOWESS lines for hypoglycaemic values are presented in orange. IDM, infant of diabetic mothers; LGA, large for gestational age; SGA, small for gestational age.
Discussion
Our experience at a single centre shows that 32% of all infants ≥35 weeks GA admitted to the well–baby nursery had risk factors for neonatal hypoglycaemia. The incidence of hypoglycaemia in screened asymptomatic at-risk infants was 16% and 0.8% of screened at-risk infants were admitted to NICU for hypoglycaemia treatment. Hypoglycaemic infants were more likely to be born at lower gestational age, born via C-section, and had multiple risk factors for hypoglycaemia. The highest percentage of at-risk infants diagnosed with hypoglycaemia was found in the preterm group (31%).
Higher threshold values result in a higher incidence of diagnosis of hypoglycaemia. Our protocol follows the AAP guidelines using time based definitional blood glucose cut-off values of <40 mg/dL in the first 4 hours and <45 mg/dL 4–24 hours of life. The incidence of hypoglycaemia in at-risk infants (16%) in this study is lower than other studies (47%) which use <47 mg/dL (<2.6 mmol/L) as a definition for hypoglycaemia diagnosis and treatment.10 12 Of note, our incidence of hypoglycaemia would be 33% if we used the cut-off value of <47 mg/dL. Remarkably, our incidence in at-risk infants was lower than that reported by Stark et al (27%), even though they used a lower cut-off value (<40 mg/dL) consistently in the first 24 hours.13 Both the Stark study and our study are single centre studies, have small sample sizes and may have differences in the baseline population as well as maternity practices such as early breast feeding. The lower incidence of hypoglycaemia results in fewer babies being treated for hypoglycaemia and a lower mother–infant separation. Because of the AAP recommended blood glucose cut-off values used in this study, only 5% of hypoglycaemic infants required admission to the NICU, which is much lower than in the Sugar Babies trial (definitional threshold for hypoglycaemia was <47 mg/dL) where 25% of the placebo group and 14% of the dextrose gel group were admitted to the NICU.7 Interestingly, the HypoEXIT Study Group,14 a multicentre, randomised, noninferiority trial, reported no difference in psychomotor development at 18 months when comparing a lower treatment threshold value of 36 mg/dL and the traditional threshold of 47 mg/dL.
We identified that screened infants were more likely to be born via C-section compared with those not screened for hypoglycaemia. C-section has been noted as risk factor for decreased exclusive breast feeding likely due to decreased skin-to-skin and increased mother–infant separation immediately after birth.13 In our centre, even after adjusting for C-section, IDM and GA, the exclusive breastfeeding rate was significantly lower in those screened, findings similar to a previous report.9 Hypoglycaemia screening may introduce stressors of focusing on feeding volumes to maintain blood glucose levels, suggesting that breast feeding is inadequate and resulting in formula supplementation.
Different risk factor groups have different first glucose values and rates of hypoglycaemia. Prematurity, C-section births and multiple risk factors were associated with hypoglycaemia. Our study shows that infants born preterm or via C-section had a significant lower first glucose value, highlighting their risk for hypoglycaemia. Interestingly, LGA or IDM infants had similar first glucose levels to the non-LGA or non-IDM infants, yet SGA infants had a higher glucose value than non-SGA infants. Infants of diabetic mothers not on insulin had a lower incidence of hypoglycaemia than those infants with mothers on insulin. This is likely due to initiating insulin in diabetic mothers who are poorly controlled; therefore, being on insulin was a risk factor for hypoglycaemia in those infants. Overall, the median first glucose values were in the normoglycaemic range suggesting that following the AAP guidelines of feeding early before the first glucose check along with frequent feedings will decrease the incidence of hypoglycaemia.
The duration of screening is variable in practice. AAP recommends continuing glucose screens before each feed for the first 24 hours in LPI and SGA infant. Recent evidence supports that two blood glucose checks may be sufficient in identifying hypoglycaemia requiring intravenous dextrose.15 In their study, Cummings et al15 showed 97% of infants requiring IV dextrose for feeding-refractory hypoglycaemia were determined with the initial glucose measurement and all were identified within the first two glucose checks. Our protocol states to stop checking blood glucose levels after achieving three normal values. All infants in our cohort who were diagnosed with hypoglycaemia were found to be hypoglycaemic within the first three glucose checks. We found 18% of at-risk infants were screened more than 3 times in 24 hours, only 4% of whom were admitted to the NICU for treatment for hypoglycaemia. This highlights that our current protocol could lead to possibly unnecessary additional testing.
The strength of our study is that we were able to describe the characteristics of neonatal hypoglycaemia in our patient population using a hypoglycaemia screening protocol based on the AAP clinical report guideline. There are a limited number of studies evaluating the AAP guidelines that have been published. This report is a single centre study, which has its own set of limitations. Our study identified a few deviations from our hypoglycaemia policy. There was a small proportion (4%) of infants at risk for hypoglycaemia who were not screened, majority of whom were SGA. Another limitation of our study was that no long-term neurodevelopmental outcome data was available as these were all ‘healthy asymptomatic’ infants in well–baby nursery. In the future, it will be helpful to have long-term follow-up on these infants.
Transient hypoglycaemia is a natural occurrence in newborns. This study suggests by following the time dependent blood glucose screening based on the AAP guidelines may decrease the number of infants diagnosed with hypoglycaemia, thus reducing interventions interfering with breast feeding as well as admissions to NICU for hypoglycaemia treatment. Future research is still necessary to follow the long-term effects of using the time dependent cut-off values given by the AAP.
Data availability statement
Data are available on reasonable request. Deidentified participant data as well as our institutional hypoglycaemia policy are available on request from the corresponding author.
Ethics statements
Patient consent for publication
Ethics approval
The Institutional Review Board (IRB) at our institution approved this study (Reference #21-017) as a retrospective study, where patient information was deidentified and consent was not required.
References
Footnotes
JBAE and SRN are joint first authors.
Contributors JBAE and SRN contributed equally and are co-first authors. JBAE collected the data, carried out initial data analysis and drafted the initial manuscript. SRN conceptualised and designed the study, ensured valid data collection, carried out data analysis, edited the initial manuscript, critically reviewed and revised the manuscript, and acts as guarantor. AH provided the data collection tool, ensured valid data collection and critically reviewed the manuscript. PJ conceptualised and designed the study and critically reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests No, there are no competing interests.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.