Article Text

Abstract
Purpose Germinal matrix haemorrhage/intraventricular haemorrhage (GMH-IVH) is a multifactorial injury with both anatomic and haemodynamic involvement. Normal variants in preterm deep cerebral venous anatomy associated with GMH-IVH have been previously described using MRI susceptibility weighted imaging (SWI). The aims of this study were to use SWI to compare the deep venous systems of a cohort of preterm neonates with various grades of GMH-IVH to a group of age-matched controls without GMH-IVH and to present novel retrospective SWI imaging findings.
Methods A neuroradiologist retrospectively evaluated 3T MRI SWI and phase imaging of 56 preterm neonates with GMH-IVH (14 of each grade) and 27 controls without GMH-IVH, scoring the venous irregularities according to three variables: decreased venous patency, increased lumen susceptibility and the presence of collaterals. Eight different venous locations, including indicated bilateral components, were evaluated: straight sinus, vein of galen, internal cerebral, direct lateral, thalamostriate, atrial and the anterior septal veins. Variables were analysed for statistical significance. Inter-rater reliability was determined via subset evaluation by a second paediatric radiologist.
Results Deep venous abnormalities were significantly more common in patients with GMH-IVH, with Wilcoxon Rank Sum Test demonstrating significant increase with GMH-IVH for total decreased venous patency (W=0, p<0.0001), increased lumen susceptibility and collateral formation. Venous abnormalities were also positively correlated with an increase in GMH-IVH grade from I to IV (patency, ρ=0.782, p<0.01) (increased lumen susceptibility, ρ=0.739, p<0.01) (collaterals, ρ=0.649, p<0.01), not just GMH-IVH alone.
Conclusion Deep venous abnormalities are significantly correlated with GMH-IVH alone and an increase in GMH-IVH grade. Further study is needed to determine cause and effect.
- Neonatology
Data availability statement
Data are available upon reasonable request. Deidentified participant data for all participants is available by reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Germinal matrix haemorrhage/intraventricular haemorrhage (GMH-IVH) is a multifactorial injury of the preterm newborn with long-term neurological sequelae. Causative factors include the fragility of the preterm deep venous system and the fluctuating haemodynamic conditions immediately following birth. There is variability in the deep venous anatomy of preterm neonates.
WHAT THIS STUDY ADDS
Preterm neonates with GMH-IVH demonstrated increased deep venous abnormalities, including venous stenosis, collateral formation and blood product deposition, when compared with preterm neonates without GMH-IVH. These deep venous abnormalities could suggest rebounding effects of the venous haemorrhage on the veins themselves.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
These findings promote the need for future prospective research into deep cerebral venous thrombosis as a possible predisposing factor for GMH-IVH or a long-term effect of observed venous changes on the neonatal brain and neurodevelopmental outcomes.
Introduction
Germinal matrix haemorrhage/intraventricular haemorrhage (GMH-IVH) is a multifactorial injury of the premature newborn that is inversely correlated with gestational age (GA) and birth weight. Of premature neonates with GMH-IVH, 90% occur in the first 72 hours after birth.1 The severity of haemorrhage, according to Papile, is determined by a four level, escalating grading system,2 where grade I is confined to the germinal matrix. The later grades include, accumulatively, extension of blood into the lateral ventricles (grade II), severe IVH with acute ventricular dilatation (grade III) and parenchymal haemorrhage (grade IV). Grade IV GMH-IVH, or white matter haemorrhage, is now considered to be due to impaired venous drainage with venous infarction and arises indirectly from GMH-IVH.2 3 GMH-IVH occurs in approximately 25% of VLBW newborns and, despite improvements in neonatal care, its incidence has not changed for newborns born at less than 26 weeks’ GA.4 GMH-IVH results in long-term neurological sequelae such as developmental delay, which can occur in even mild GMH-IVH (grade I or II), cognitive deficits, cerebral palsy and posthaemorrhagic hydrocephalus.5 6
Beyond contributing clinical factors, such as fluctuations in haemodynamics or disruption of cerebral autoregulation,7–10 the germinal matrix has several anatomical characteristics increasing its susceptibility to ischaemia, vascular permeability, and therefore haemorrhage.11 Microscopically, the nascent vessels in the germinal matrix are weakened by a deficiency of several blood–brain barrier components, including pericytes, astrocyte end-feet glial fibrillary acidic protein, tight junctions and basal lamina fibronectin, as well as diminished extracellular matrix support including decreased collagen type VI fibres and an absent layer of muscularis.12–16 The germinal matrix has a unique ‘bamboo bush’-like vascular end zone composed of numerous small venules at the ventricular side of the terminal vein.17 The vascular complexity of this region is further complicated by a peculiar venous ‘U-turn’ or acute angle at the level of the foramen of Monro3 18 where a confluence of multiple veins, including the medullary, thalamostriate and choroidal, drain as the terminal vein into the internal cerebral veins.11 Finally, the termination of several arteries near the germinal matrix, including the lateral striate and the recurrent artery of Heubner, complete the region’s characterisation as a vascular watershed.19 20
Integrating neuropathology with neuroradiology has allowed the neuroradiologist to connect imaging findings in premature neonates with pathological findings.21 Pathology studies have demonstrated the venous origin of GMH-IVH,19 22 possible associated larger vessel diameter,23 24 as well as posthaemorrhagic venous consequences.19 25 Recently, related imaging findings have been documented using MRI and susceptibility weighted imaging (SWI), including medullary vein engorgement, increased venous curvature, thrombus location and other vascular malformations.26–29 We designed the present study with the main aim of describing novel germinal matrix venous abnormalities, including decreased venous patency, increased lumen susceptibility and collateral formation in a population of premature newborns with or without GMH-IVH. With insights from neuropathology and comparison to controls, we hypothesise that newborns with GMH-IVH will have increased incidence and severity of deep venous abnormalities.
Materials and methods
Study design
This was a retrospective, observational study in neonates who underwent MRI between 2011 and 2022 at our institution (department of radiology, University of Florida College of Medicine).
Subjects
Subjects were selected from a prior GMH-IVH study30 Excel document and Visage V.7 (Pro Medicus: Richmond, Australia), our electronic database, by a search for the keywords ‘germinal matrix haemorrhage’. The other patients were included by searching Visage with the study description search term ‘MR brain neonatal’ and cross-checking to prevent duplication. Inclusion criteria were as follows: (1) a history of GMH-IVH diagnosed on head ultrasound (HUS) within one week after birth, (2) the availability of at least one MRI with SWI and phase imaging study of diagnostic quality and (3) the use of a 3T scanner. Patients were excluded from the study if (1) motion, resolution or imaging technique prevented a clear evaluation of the deep venous system, (2) GA exceeded 32 weeks of pregnancy, (3) GMH-IVH was not detected on MRI even though it was noted on HUS or (4) a 1.5 T scanner was used. When selecting patients for our control group, all inclusion and exclusion criteria were followed except the first inclusion criterion of a history of diagnosed GMH-IVH. One additional patient was excluded due to a choroid plexus bleed, which prevented both normal or GMH-IVH categorisation. GMH-IVH grading was performed using acute phase HUS. If a patient had bilateral GMH-IVH with a left grade II and a right grade I, this was classified as grade II. The same was done for other grades. Additionally, GA, sex, birth weight and date of birth were collected on each subject (table 1). To account for inflammatory clinical factors that could affect the venous system independent of GMH-IVH, the control group was also evaluated for white matter injury via T2 MRI. All normal cases were found to be without any evidence of white matter injury with inter-rater reliability (IRR) of 100%.
Average patient characteristics with SD
Image acquisition
MRI, including axial SWI, was performed on a 3T scanner (Siemens Verio) between 2011 and 2022 with our radiology department’s multichannel head coil. While the extended study time provided a significant study sample size, which would have otherwise been limited due to the relatively few preterm babies born each year, it also meant that our study technique was not homogenous due to slight changes in technique including scanner replacement and sequence optimisation. Imaging protocol did not include sedation or general anaesthesia for the entirety of the study period. For our study patients, imaging was typically performed prior to discharge when neonates had reached term equivalent age. Image acquisition included magnetic, phase and SWI images with minimum intensity projection, which were automatically obtained from the scanner.
Analysis of SWI venography
Analysis of all images was performed by MA, a neuroradiology attending physician with 22 years of neuroimaging research experience. Each deidentified patient was sorted into normal or grade I-IV GMH-IVH groups, resulting in 27 normal patients and 14 patients for each respective grade. Following sorting, the deep venous system was evaluated for decreased venous patency, increased lumen susceptibility and the presence of collateral veins. For the evaluation of each image, a 2-series panel was created in Visage V.7 with SWI (top: minimal intensity projection at 6.0 mm) and phase images (bottom: maximum intensity projection at 6.0 mm). At times, to improve accuracy and detail, a range between 4.0 and 10.0 mm was used. The following veins were evaluated in sequence and bilaterally when indicated: straight sinus, vein of Galen, internal cerebral, direct lateral, thalamostriate, atrial and anterior septal. Descriptive, categorical variables were scored according to table 2. To validate the IRR of our developed scoring system, a second paediatric radiologist, EY, with 22 years of radiology experience, evaluated a random subset (25%) of the total sample. This subset was created using an online random number generator to select 21 cases, which resulted in the random selection of 6/27 normal, 5/14 GMH grade I, 3/14 GMH grade II, 4/14 GMH grade III and 3/14 GMH grade IV cases. IRR for the normal, GMH grade I, grade II, grade III and grade IV groups, were, 99%, 81.7%, 71.3%, 73.6% and 70.4%, respectively. These IRR percentages reflect the total, absolute agreement for the evaluation of every variable and vein component.
Venous abnormality scoring method
Statistical analysis
The data were recorded using Microsoft Excel and analysed using R Statistical Software (V.4.1.3; R Core Team 2021). The correlation between variables were assessed using Spearman rank correlation (also known as Spearman’s rho) and Wilcoxon Rank Sum (ie, Mann-Whitney U) tests. Statistical significance was established at p<0.05. These choices were made because the variables (eg, GMH levels) are at ordinal level, hence require non-parametric approaches. The correlation was also tested against lack of correlation (ie, zero correlation) in either positive or negative direction. First, variables were compared for normal (or GMH=0) versus combined GMH I–IV (or GMH alone) using Wilcoxon rank sum test, and when this was significant, to see which individual GMH levels are significantly different than normal level, a pairwise comparison of variables for all 10 possible pairs (which also included comparing variables for different levels of GMH from I–IV) was performed using pairwise Wilcoxon rank sum test. The p values for the pairwise comparisons were adjusted with Holm’s correction for multiple comparisons.31 The adjusted p values for pairwise comparisons indicate significance differences between GMH 0 level and GMH X levels, for each of X=I, II, III and IV, but no significant difference is observed between the GMH levels I, II, III and IV (for each pairwise comparison). Hence, in our results section, we only report the comparison of GMH 0 level with the combined GMH levels (ie, I–IV together).
Patient and public involvement
Neither patients nor the public were involved in the design or development of this study.
Results
Subjects
The deep venous anatomy of 99 preterm neonates with brain imaging conducted from 2011 to 2022 at our institution was retrospectively evaluated, following the exclusion of 232 patients due to 1.5T imaging or 3T imaging without SWI and phase imaging. Six patients were excluded due to motion artefacts or poor imaging technique, nine were excluded due to having a GA greater than 32 weeks which is beyond the typical range for GMH-IVH and one was excluded due to the presence of a choroid plexus bleed (figure 1).
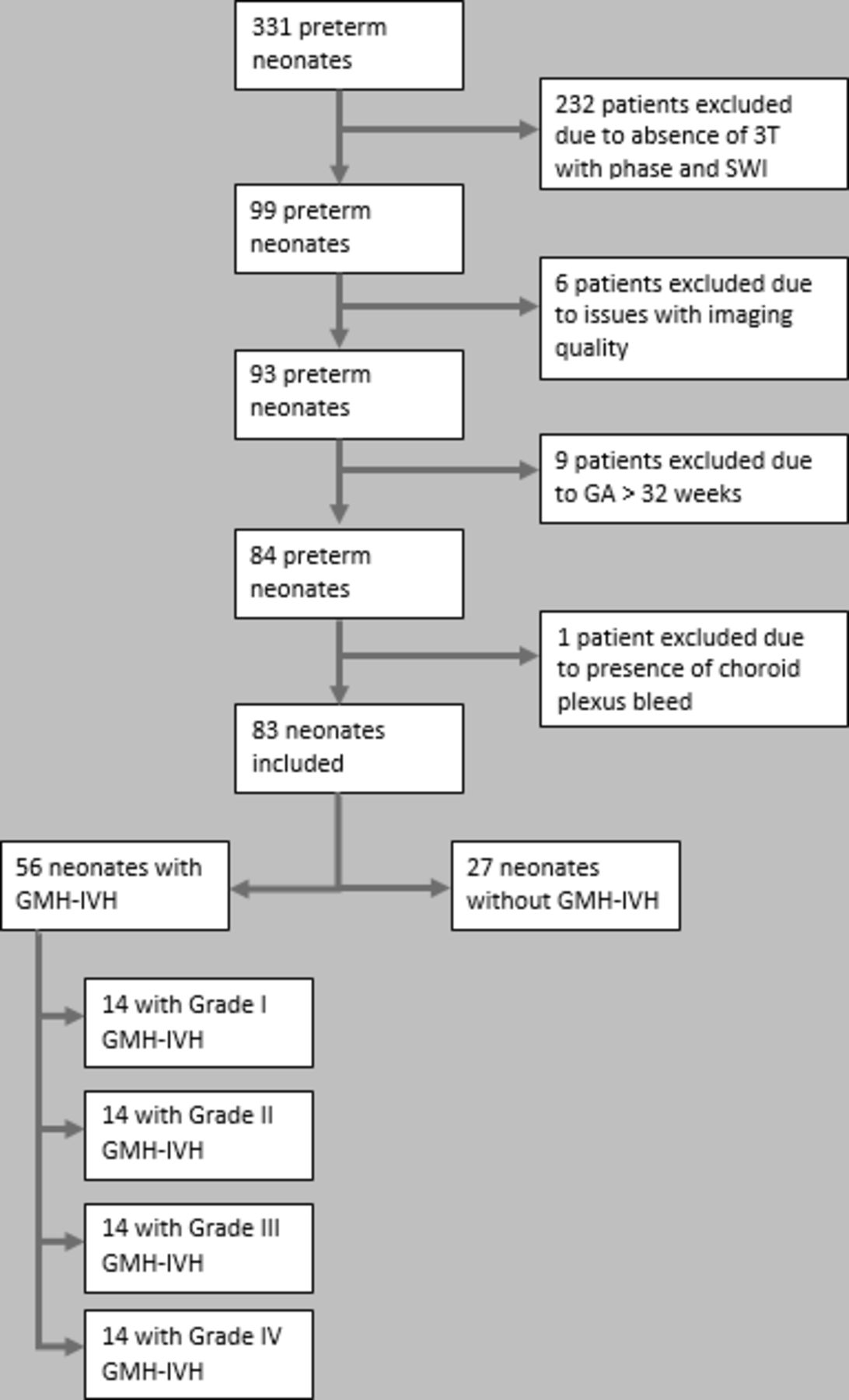
Study population selection flow chart. GA, gestational age; GMH-IVH; germinal matrix haemorrhage/intraventricular haemorrhage; SWI, susceptibility weighted imaging.
Total deep venous system abnormalities and GMH-IVH combined
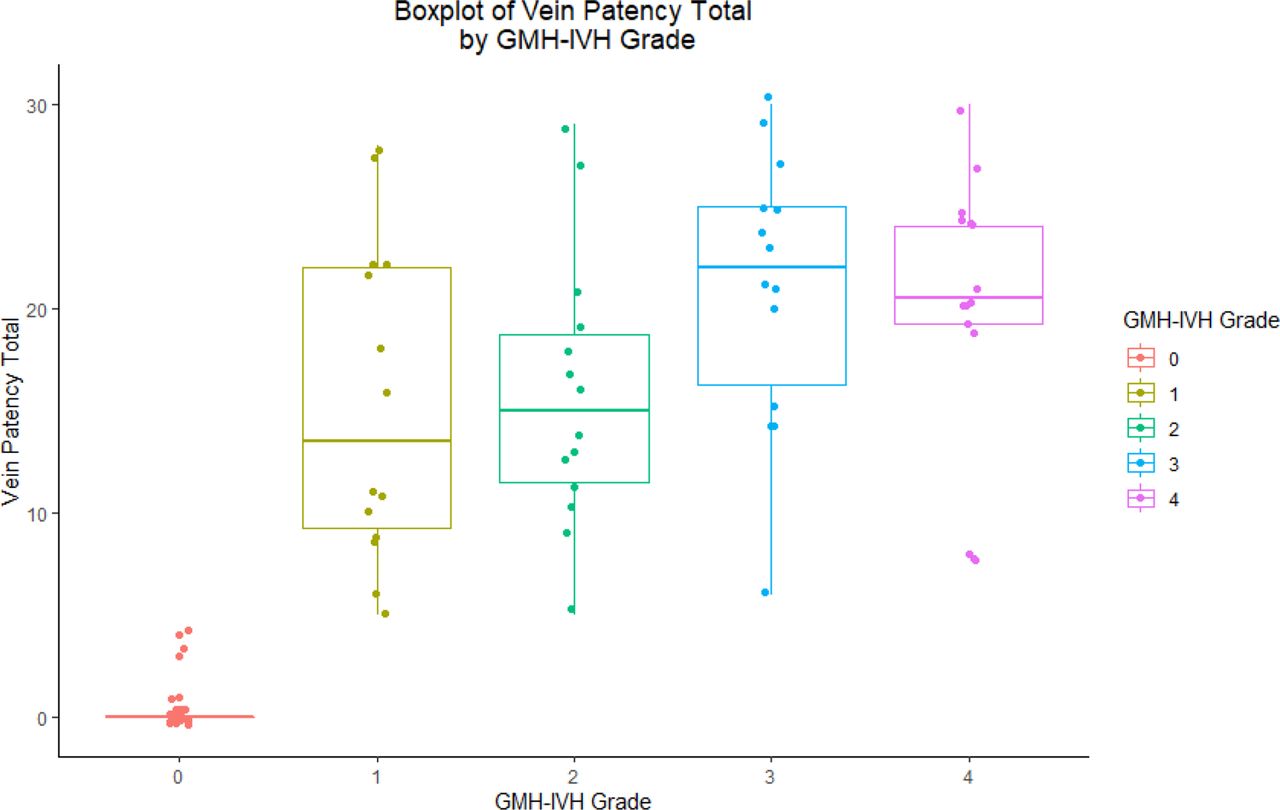
Venous abnormalities were significantly more common in patients with GMH-IVH (table 3). Using the Wilcoxon Rank Sum Test or Mann-Whitney U Test, comparing total decreased venous patency score between controls and GMH-IVH grades I–IV combined, all control values were found to be smaller than the combined GMH-IVH grades I–IV (figure 2). The results from the Wilcoxon analysis indicate the statistically significant, non-random chance of finding venous abnormalities associated with GMH-IVH, where all GMH-IVH grades are combined (figures 2–4). Table 4 also shows data averages per variable and grade for transparency, although these averages were not used for statistical analysis due to the non-parametric approach necessitated by ordinal data.
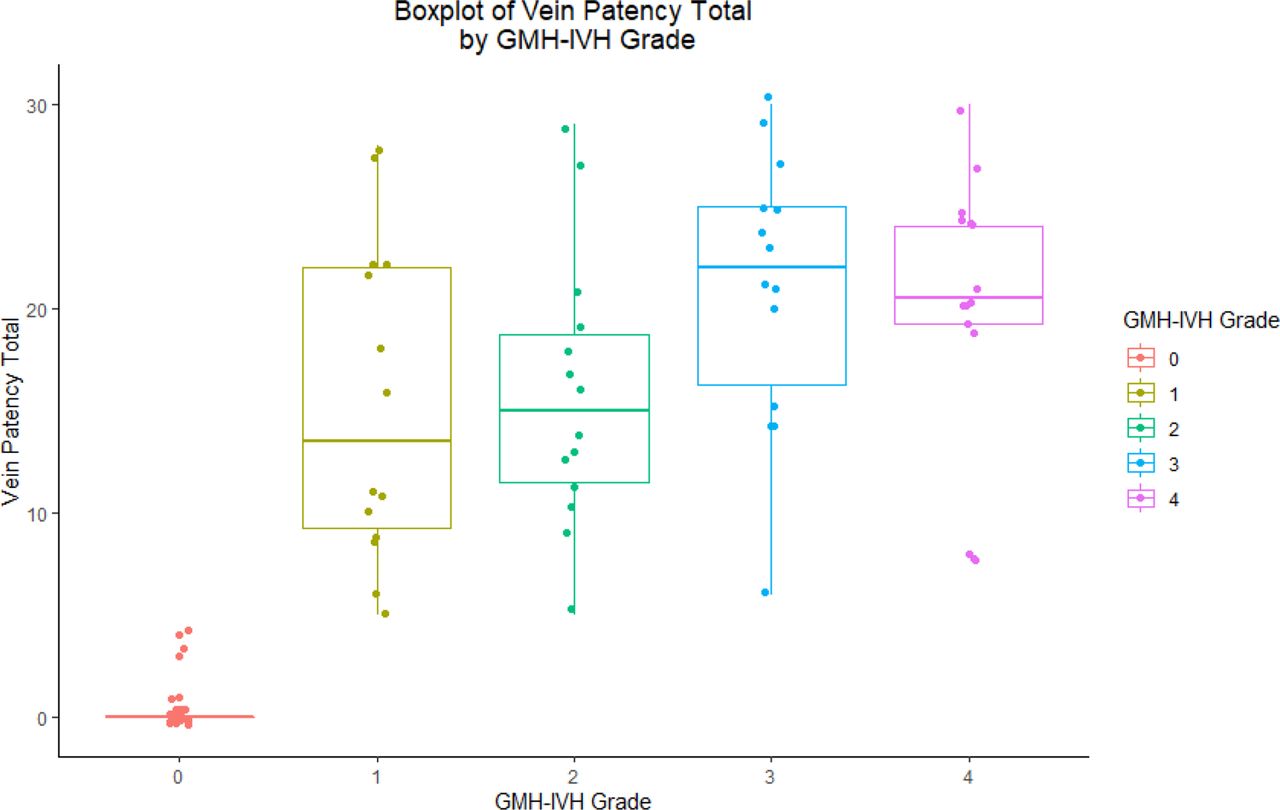
Boxplot of correlation between germinal matrix haemorrhage/intraventricular haemorrhage (GMH-IVH) grade and decreased venous patency total score, which serves as a composite value for vein patency changes in the entire deep cerebral venous system.
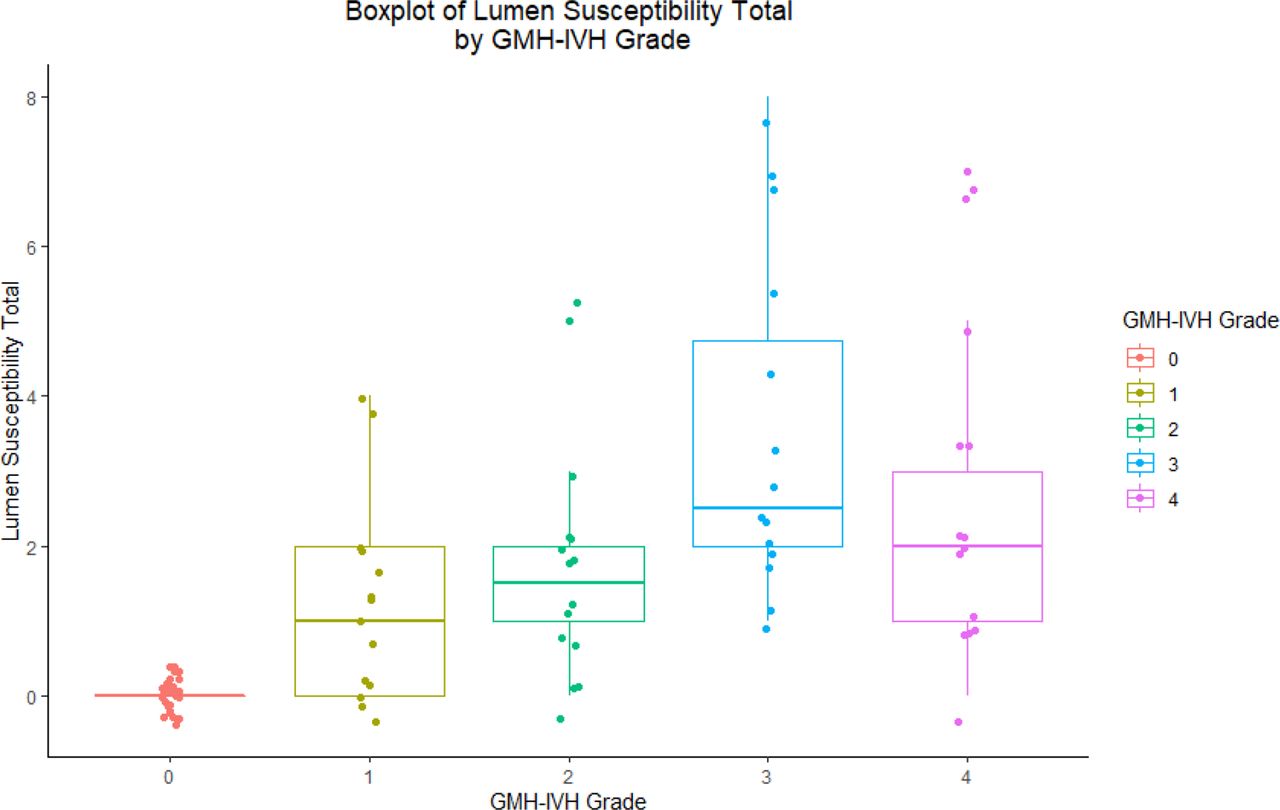
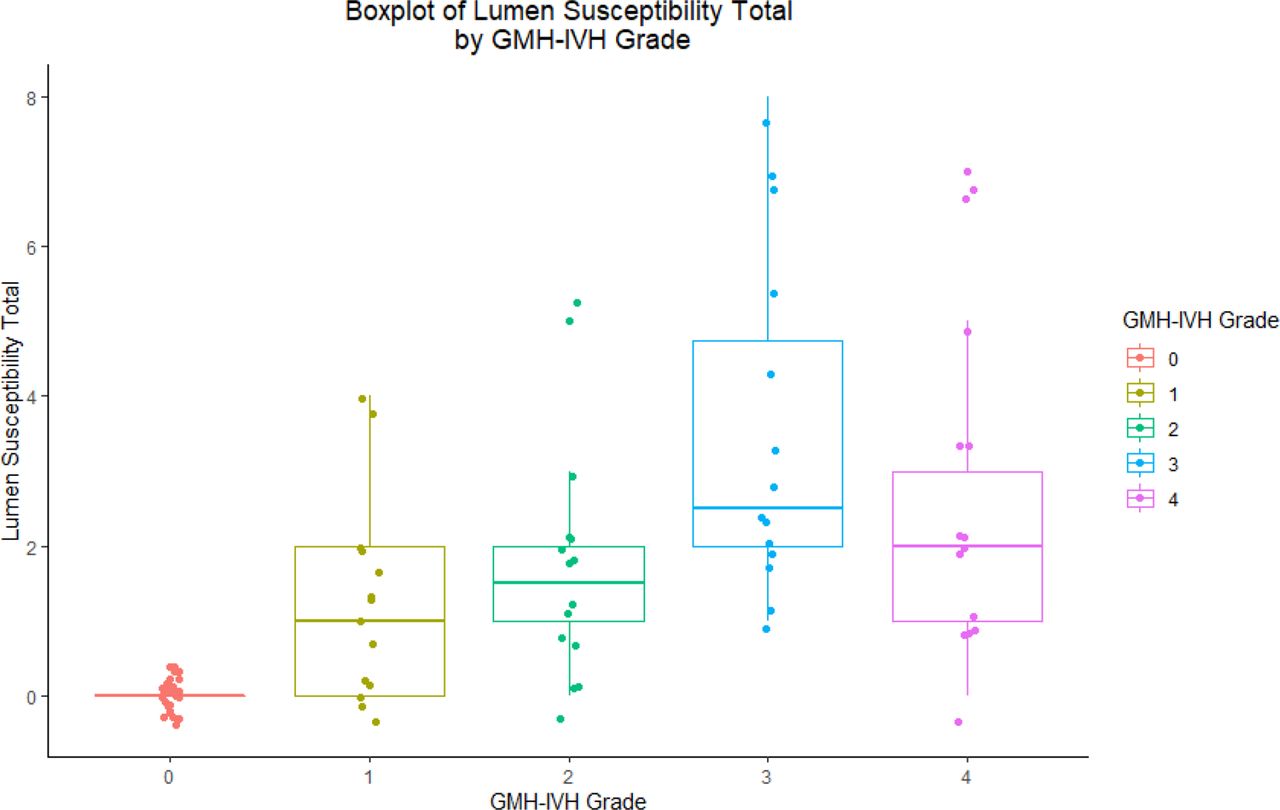
Boxplot of correlation between germinal matrix haemorrhage/intraventricular haemorrhage (GMH-IVH) grade and total lumen susceptibility score.

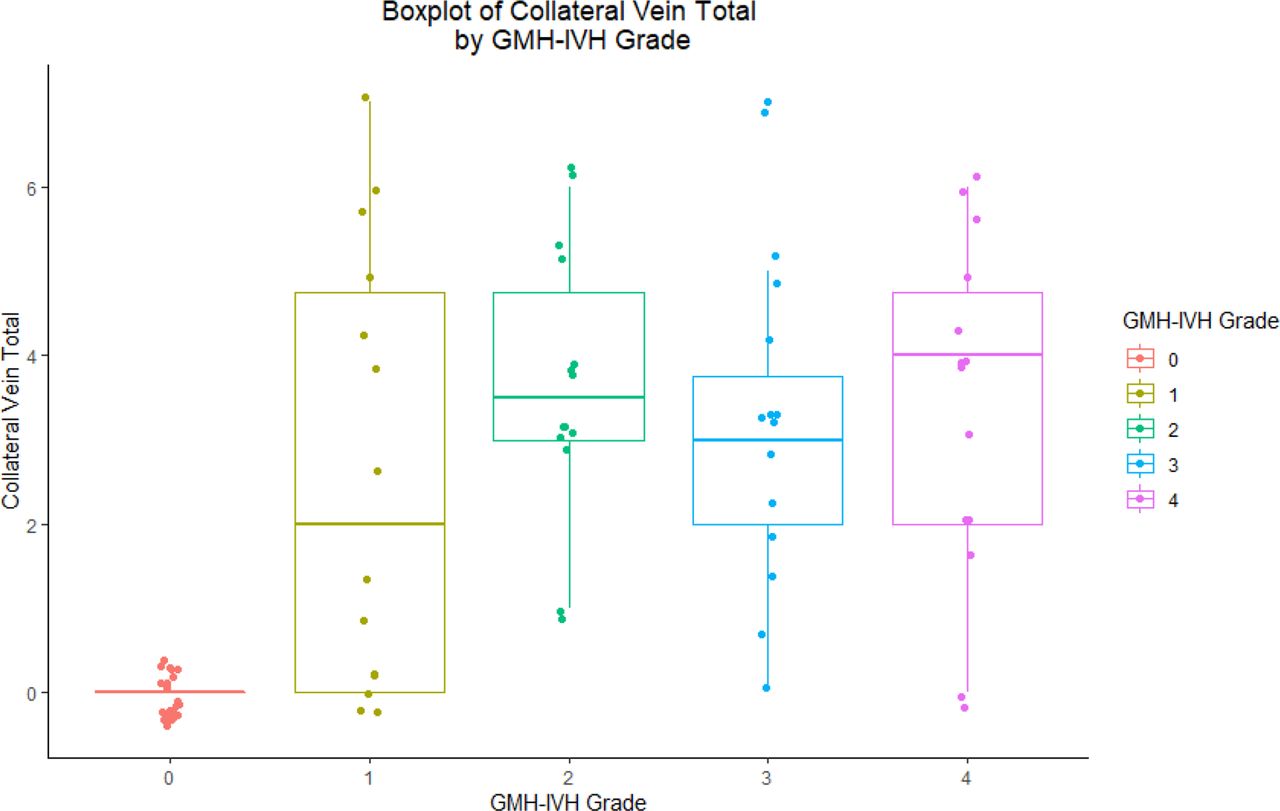
Boxplot of correlation between germinal matrix haemorrhage/intraventricular haemorrhage (GMH-IVH) grade and total collateral vein formation score.
Correlation between increasing GMH-IVH grade (0–IV) and venous abnormalities, with Spearman’s rho correlation coefficients and p values
Medians with IQRs for total venous abnormality scores, and wilcoxon W and p values
Total venous abnormalities and increase in GMH-IVH grade
Not only were venous abnormalities positively correlated with combined GMH-IVH I-IV, but venous abnormalities were also positively correlated with increase in GMH-IVH grade, both in total and per individual vein (table 3). Total decreased venous patency score, as a composite value of the entire deep venous system, was found to have a 0.782 positive correlation with increase in GMH-IVH grade (p<0.001). Similarly, increased lumen susceptibility was found to have a 0.739 correlation (p<0.001) and collaterals a 0.649 correlation (p<0.05).
Venous abnormalities for individual veins and increase in GMH-IVH grade
Positive correlations were also found for the majority of individual veins (table 3), but generally to less of an extent than the total scores. For example, the right and left thalamostriate vein (TSV) had 0.776 and 0.758 correlations between decreased vein patency and GMH-IVH grade, respectively, while the straight sinus and vein of Galen only had correlations of 0.48 and 0.37. In general, among the variables, decreased vein patency showed the highest correlations with GMH-IVH grade per individual vein. As an exception, the right TSV also showed a high correlation of 0.7 for collateral formation. The DLV shows ‘not applicable’ for some of the venous abnormalities because only a minority of our sample expressed this venous variant. The DLV (right and left) was present in 63% and 30% of normal neonates, respectively, but both right and left were present in 7% of neonates with GMH-IVH. Individual examples of normal deep venous anatomy and venous abnormalities can be seen in figures 5–10.

Axial maximum intensity projection phase imaging of the superior (A) and inferior (B) normal deep venous system with corresponding labelled schematic representations.

Axial phase MIP (left) and SWI MinIP (right) images of a grade I GMH-IVH patient with multifocal areas of vein patency (VP) score 1, 2, and 3 stenosis of the deep cerebral veins (A). Additional images demonstrate a grade II GMH-IVH patient with VP score 4 stenosis of the bilateral TSV with two haematomas on the left (B). Axial phase MIP and SWI MinIP images (C) of a grade III GMH-IVH patient demonstrate areas of venous abnormalities in the bilateral TSV with collateral vessels and areas of lumen susceptibility. VP score 0=normal. VP score 1=contour irregularities. VP score 2=stenosis <50%. VP score 3=stenosis >50%. VP score 4=occlusion. GMH-IVH, germinal matrix haemorrhage/intraventricular haemorrhage; L, left; MinIP, minimal intensity projection; MIP, maximum intensity projection; R, right; SWI, susceptibility weighted imaging; TSV, thalamostriate vein; VP, vein patency.
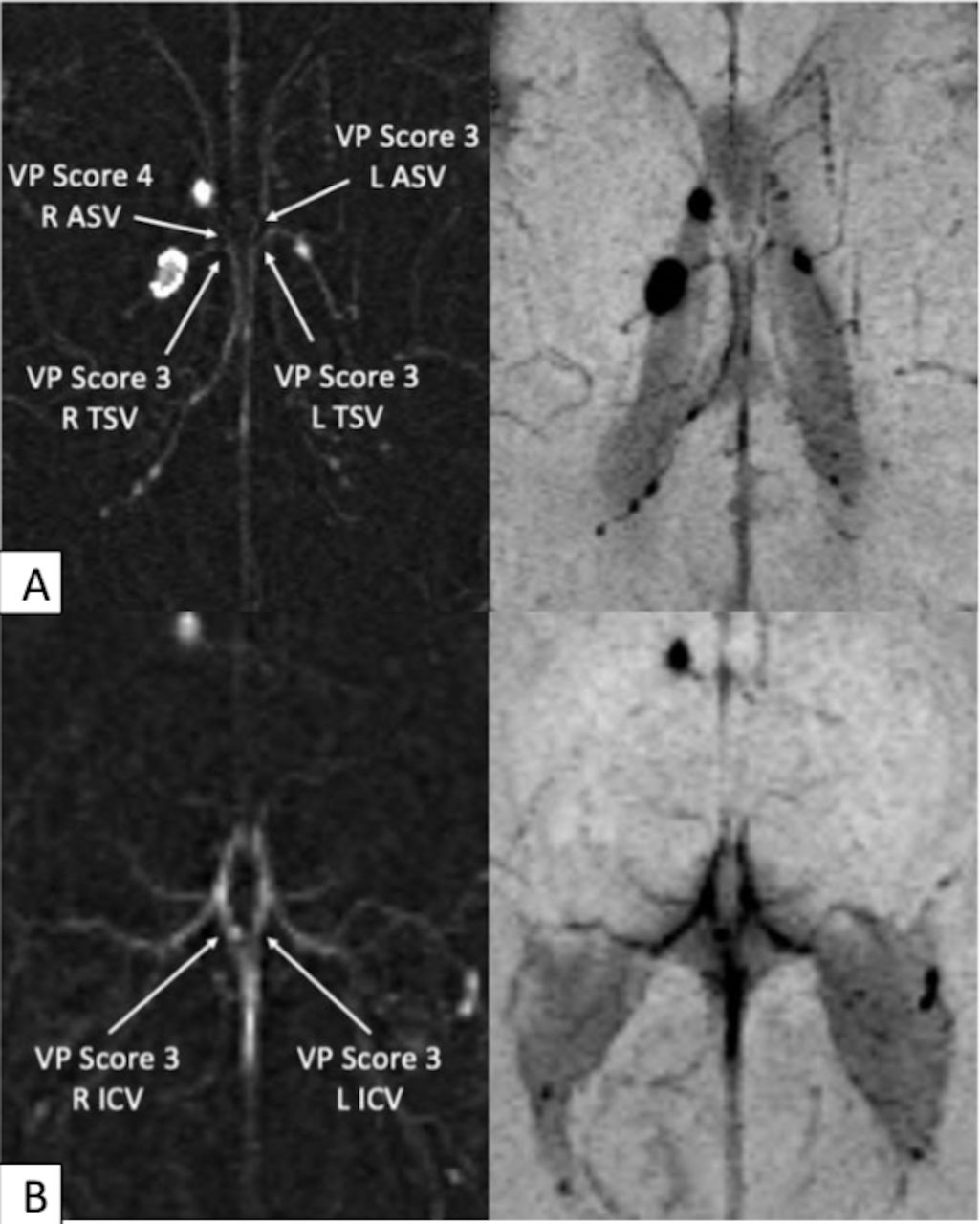
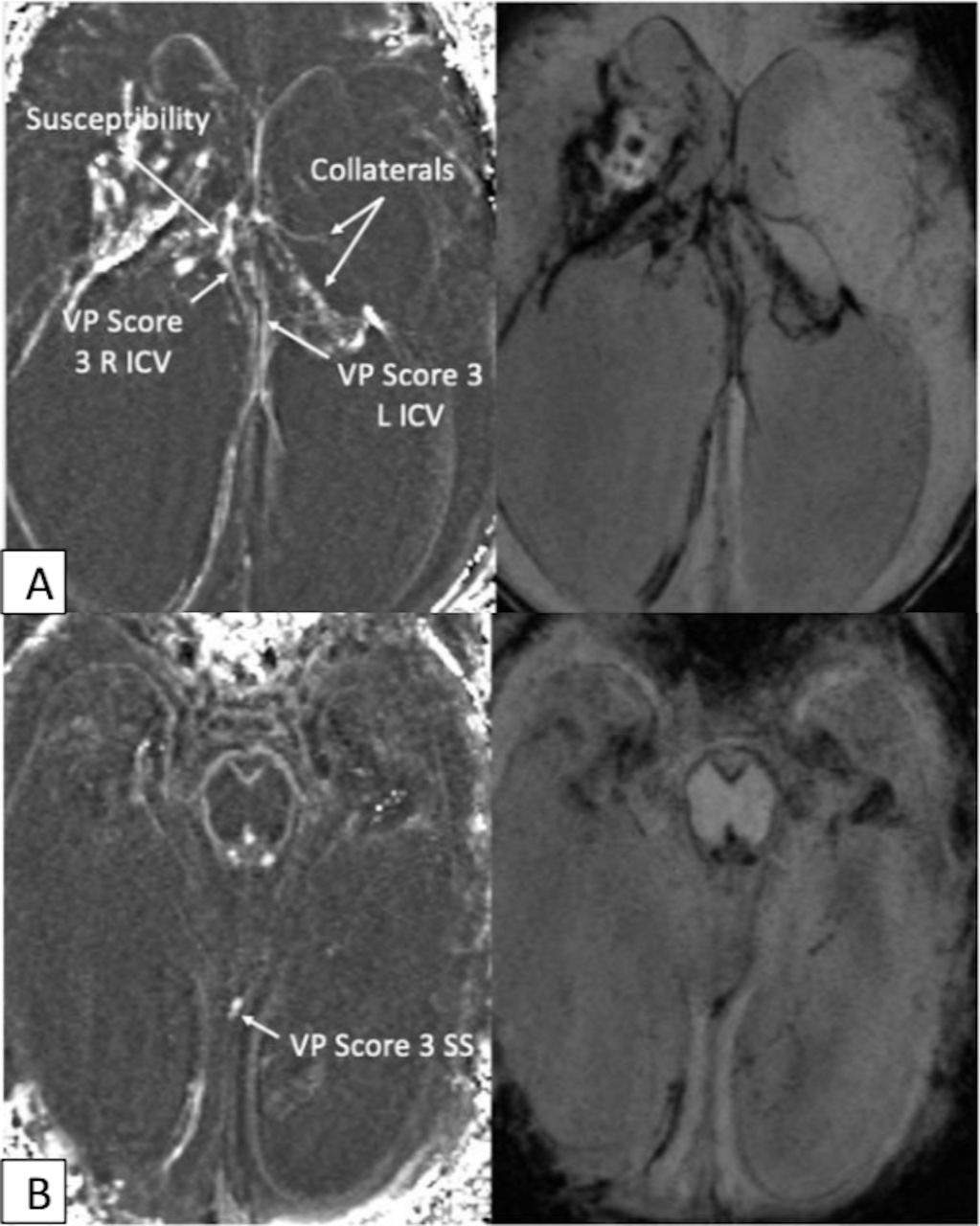
Axial phase maximum intensity projection (left) and susceptibility weighted imaging minimal intensity projection (right) images of a patient with grade I GMH-IVH demonstrating VP score 4 right ASV occlusion, VP score 3 left ASV stenosis and bilateral VP score 3 TSV stenosis (A). Additional images demonstrate VP score 3 bilateral proximal ICV stenosis (B). ASV, anterior septal vein; ICV, internal cerebral vein; TSV, thalamostriate vein; VP, vein patency.

Axial phase maximum intensity projection (left) and susceptibility weighted imaging minimal intensity projection (right) images of a patient with grade II GMH-IVH demonstrate multifocal areas of venous stenosis and occlusion with downstream collaterals in the right TSV territory and a haematoma in the left TSV territory with proximal luminal narrowing (A). Additional images demonstrate stenosis of the VoG and bilateral ICV occlusion (B). ASV, anterior septal vein; ICV, internal cerebral vein; TSV, thalamostriate vein; VoG, vein of Galen; VP, vein patency.

Axial phase maximum intensity projection (left) and susceptibility weighted imaging minimal intensity projection (right) images of a patient with grade III GMH-IVH. There are multifocal areas of severe venous stenosis and VP score 4 occlusion in the deep venous system (A–C). There is proximal occlusion of the left TSV (C), left ICV (B), and severe luminal narrowing of the right ICV (B) and right TSV (C). The straight sinus is normal (B). Venous collaterals can be seen in the left caudothalamic notch (A). ASV, anterior septal vein; ICV, internal cerebral vein; TSV, thalamostriate vein; VoG, vein of Galen; VP, vein patency.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Axial phase maximum intensity projection (left) and susceptibility weighted imaging minimal intensity projection (right) images from a patient with grade IV GMH-IVH demonstrate pronounced hydrocephalus with resultant distortion of the usual deep venous cerebral architecture. There is complete occlusion of the bilateral thalamostriate vein. There is VP score 3 stenosis of the bilateral ICV with large haematomas bilaterally and collaterals in the left thalamus (A). There is VP score 3 stenosis of the SS (B). ICV, internal cerebral vein; SS, straight sinus; VP, vein patency.
Discussion
In this study, MRI SWI with phase imaging, was used to visualise venous abnormalities in the deep venous system of the preterm infant brain. Comparing preterm infants without GMH-IVH to those with GMH-IVH, a significant difference was found supporting our original hypothesis that venous abnormalities would be associated with GMH-IVH (tables 3–4).
Recent SWI MRI studies have suggested that normal variants of venous anatomy are predisposing factors to GMH-IVH. In a series of retrospective studies by Tortora et al, deep venous variants were first classified and then found to be correlated with GMH-IVH,29 32 indicating a possible predisposition to GMH-IVH due to increased venous curvature and its theorised implications on flow dynamics such as shear stress. By contrast, in our study, we examined venous abnormalities such as occlusion or lumen susceptibility rather than normal variants.
One explanation for the presence of decreased vein patency, in some cases to the point of occlusion, would be a so-called rebounding effect, where the haemorrhage itself causes venous obstruction and other abnormalities. In Ghazi-Birri’s autopsy study,19 perivenous blood invasion caused by GMH-IVH was shown to ‘invariably distort’, compress and even occlude adjacent veins, which corresponds well with our decreased vein patency finding. A Doppler sonography study by Taylor25 demonstrated that GMH-IVH displaced terminal vein position and patency in 21/48, with no flow identified in 13 veins. Interestingly, an increase in haemorrhage size and complexity was associated with increased severity of terminal vein abnormality, concordant with our finding of increased venous abnormality severity with increasing GMH-IVH grade. This association suggests that the venous abnormalities examined in our study may at least partially develop in the post-GMH-IVH setting as increased haemorrhagic destruction could result in more venous disturbances.
Studies have also examined other changes that occur in the brain after GMH-IVH, including stages in the reaction of the haemorrhage, superficial siderosis (the deposition of haemosiderin in the central nervous system) and white matter changes, which can occur even in mild GMH-IVH.30 33–35 Collateral formation is likely the clearest example of a venous abnormality arising in the post-GMH-IVH setting. Collaterals represent a reaction to flow obstruction, which, such as the process of recanalisation, requires time. Collaterals can be distinguished from native vessels by their size and location. They can also usually be distinguished from variant anatomy using the same criteria, although some confusion between the two is possible. Additionally, while vasospasm is more commonly associated with arteries, blood products from GMH-IVH could also cause venous disturbances without could hypothetically worsen with increased haemorrhage.36
Finally, a decrease in cerebral saturations have also been noted after severe GMH-IVH possibly due to disturbance in intracranial blood flow.37
Recently, in a case report,38 Tanaka et al described a Doppler finding of blood flow reversal in the deep cerebral vein concurrent with GMH-IVH. In the two patients, blood flow improved sometime after development of GMH-IVH. The authors were unable to ascertain whether the blood reversal occurred just before, during, or after GMH-IVH, but concluded that venous flow is intricately connected to GMH-IVH pathogenesis. Our data, though limited by its retrospective nature, further adds to our understanding of venous involvement after GMH-IVH and demonstrates anatomic sequelae indicated by deep venous system abnormalities seen months after the initial haemorrhagic event on term corrected MRI imaging.
The major limitations of this study are its retrospective nature and a relatively small sample size due to our strict inclusion and exclusion criteria. Given the retrospective nature of our study, the MRI images were acquired over a 10-year period, which resulted in additional variables of sequence optimisation and scanner replacement during this time. The imaging protocols used during this study were not designed for the evaluation of the small deep venous structures examined. We suspect that IRR would improve with more advanced imaging techniques, such as thinner slice imaging, dedicated coils and higher magnetic field strength scanners. The images were also acquired around 36 weeks post corrected GA, well after the occurrence of the GMH-IVH. As a result, the presence of venous abnormalities before or after the haemorrhage cannot be timed. However, we provide data that suggests further prospective studies should be performed on patients with clinical predisposition to GMH-IVH to investigate the role of these deep venous findings and the role of occlusion in the pathophysiologic evolution of injury after a GMH-IVH.
Conclusion
In this paper, we have documented significant positive correlation between novel observations of venous abnormalities of the preterm infant deep venous system and GMH-IVH, including correlation with increasing GMH-IVH grade.
Data availability statement
Data are available upon reasonable request. Deidentified participant data for all participants is available by reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants. The University of Florida IRB approved IRB study ID: IRB201800263. Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The authors would like to thank Christina Bukata, DMD, for help with figure design.
References
Footnotes
Contributors TK is the author responsible as guarantor. TK and MA had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: MA, TK, MDW. Acquisition, analysis or interpretation of data: MA, EY, TK, EC. Drafting of the manuscript: TK. Critical revision of the manuscript for important intellectual content: MDW, MA, VS, EY. Statistical analysis: EC, TK. Obtained funding: TK, MDW. Administrative, technical or material support: LS, VS, EC. Supervision: MA, MDW. Figure design: VS.
Funding TK was supported by a grant from the National Institutes of Health (NIH T35HL007489). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. MDW was supported by an NIH Grant: R01HD105055-01A1.
Competing interests None.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.