Article Text

Abstract
Objective Therapeutic hypothermia (TH) for moderate-to-severe neonatal hypoxic ischaemic encephalopathy (HIE) is generally described as safe. We performed this study to determine the incidence of bilious vomiting or bilious drainage (BVD) attributable to TH in this population.
Design A single-centre, retrospective cohort study.
Setting Neonatal and paediatric intensive care units (NICU and PICU) of a single tertiary care centre.
Patients All newborns with HIE who met criteria for TH between 2009 and 2014.
Interventions Cases were matched 1:1 for unit of care (NICU vs PICU), gestational age, gender, and Sarnat score with historic controls who did not receive TH. Groups were compared with Pearson's Χ2 analysis. Relative risk was calculated, and ORs were used to allow regression analysis.
Results Forty-seven patients met all inclusion criteria. The incidence of BVD in patients who received TH was 26%. The group exposed to TH was more likely to experience BVD compared with the control group with a relative risk of 6.0(95% CI 1.4 to 25.4), even after accounting for improper or unchecked nasogastric position, opioids and muscle relaxant use, OR=7.8(95% CI 1.4 to 43.3), and when positive blood culture was included in the regression model, OR=11.6(95% CI 1.2 to 115.0). Three patients underwent investigation and no patients had surgical pathology.
Conclusion TH appears to be associated with non-pathological bilious vomiting or gastric drainage. Further prospective data are needed to identify the patients in whom investigation and intervention may be avoided.
- cooling
- bilious drainage
- newborn
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Therapeutic hypothermia improves neurological outcomes in neonatal patients with hypoxic ischaemic encephalopathy.
Bradycardia, decreased cardiac stroke volume, and renal impairment have been previously described as complications of this therapy.
Studies of adults receiving therapeutic hypothermia demonstrate decreased gut perfusion and motility.
What this study adds?
This is the first study describing bilious emesis or drainage as a complication of therapeutic hypothermia in neonatal patients.
We provide the risk attributable to therapeutic hypothermia in our sample. As bilious vomiting or drainage may herald clinically significant intestinal pathology requiring investigation and possibly surgery, the clinician should be aware of this risk.
Introduction
Hypoxic ischaemic encephalopathy (HIE) is estimated to affect between 1 and 6 per 1000 live births.1 It can be associated with significant long-term neurological sequelae and death. Therapeutic hypothermia (TH) is currently the standard of care for moderate-to-severe HIE in late preterm and term neonates. It involves whole body cooling, ideally within the first 6 hours of life, to an optimal core temperature of 34ºC±0.5ºC.2 3 This neuroprotective strategy has been described for over a decade and is generally described as a safe intervention that reduces death or disability in survivors.4 Although cooling may be done selectively to the head, modelling indicates that whole body cooling is necessary to achieve a deep brain temperature of 34ºC5 and there may be some benefit to whole body cooling in preventing neuromotor or developmental delay in survivors.4
In our centre, two recent patients had non-pathological bilious emesis requiring investigation while undergoing TH. In the general neonatal population with bilious vomiting, the incidence of true intestinal pathology, such as midgut volvulus or intestinal atresia, is as high as 46%.6–9 Bilious vomiting or drainage (BVD) has not previously been described as a side effect of TH and the incidence in this population is unknown.
The primary objective of this study is to describe the relative risk of non-pathological BVD between neonates who did and did not receive TH for HIE. Secondary objectives include describing the incidence of BVD in the neonatal population who received TH for HIE, and identifying patient characteristics that may be associated with bilious vomiting. We hypothesised that the incidence and relative risk of bilious vomiting/emesis was higher in the cooled cohort.
Methods
We conducted a single-centre, retrospective cohort study of all neonates aged <1 week who had a final diagnosis of HIE, met criteria for TH and underwent TH at St. Joseph’s Health Care London and the Children’s Hospital, London Health Sciences Centre (LHSC) between 2009 (initiation of TH protocol) and 2014. The study protocol has not been previously published.
Criteria for TH were defined in previously published guidelines1: gestational age (GA) ≥36 weeks; moderate-to-severe encephalopathy as defined by a Sarnat score II or III presenting before 6 hours of life; and two of Apgar score <5 at 10 min of age, continued need for ventilation and resuscitation at 10 min of age, and/or metabolic acidosis with pH <7 or base deficit >16 mmol/L in cord or arterial blood gases measured within 1 hour of birth. Infants were cooled to 33°C–34°C through active servo-controlled whole-body cooling using cooling blankets. Cooling continued for 72 hours, at which point infants were rewarmed by 0.5°C every hour as tolerated.
The neonatal intensive care unit (NICU) of St. Joseph’s Health Centre cared for approximately 850 neonatal patients annually until 2011, when it moved to LHSC and assumed care for all inborn and premature patients (900–1000 annually). The paediatric intensive care unit (PICU) of LHSC cared for approximately 150 neonatal patients annually until 2011, and 50–100 since.
A standard nasogastric or orogastric (collectively abbreviated as NG) tube insertion, maintenance, and feeding protocol was in place during the study periods in both units. The NG tube was first inserted as per current Neonatal Resuscitation Program recommendations.10 The position was checked by aspiration of stomach contents, auscultation for air entry ‘pop’, and confirmed by X-ray (two views in the NICU and one antero-posterior view in the PICU). Incorrectly positioned gastric tubes were repositioned to sit in the body of the stomach. Final insertion depth was noted at the nares and recorded on the daily nursing flow sheet. The position of the NG tube was checked once per nursing shift by confirming depth of insertion, auscultation for air entry, and aspiration of air/gastric contents. If concerned, X-ray confirmation was obtained. For purposes of the analysis, the NG tube was considered malpositioned any time that its position was not confirmed within the first day of therapy or its position was not confirmed by nursing.
Bilious NG aspirates were detected either by spontaneous drainage from an open NG or by manual aspiration of green bile at one of the regular position checks. Infants with HIE in the pre-TH era did not receive enteral feeds for at least the first 48 hours after birth, and those receiving TH did not receive enteral feeding until rewarming was complete. Thereafter, feeds for all infants followed a hospital-based protocol that included trophic feeding of 20 mL/kg/day continuously with checks for gastric residuals every 4 hours, and advancement of feeds by 15–20 mL/kg/day when gastric residuals were minimal.
The cohort was matched 1:1 for unit of care (NICU vs PICU), GA, and Sarnat score with historic controls who had HIE and did not receive TH. Matching proceeded in a retrograde fashion, such that the most recent patients with HIE from the precooling era were examined for a potential case match first, and we worked backward in time until all cases were matched. Historic controls were necessary as all patients meeting criteria for TH from 2009 received the therapy. Matching criteria were chosen to ensure that patients had a similar degree of illness (Sarnat score), similar baseline risk (GA within 7 days and in the same gestational week where possible), and received similar care practices (unit of care). We also attempted to match 1:1 for gender to ensure similar baseline characteristics and risk. It was agreed that this characteristic would be least likely to affect baseline risk of BVD and so when matching was not possible the requirement was eliminated rather than excluding a member of the interventional cohort, resulting in three pairs unmatched for gender.
Eligible subjects and controls were identified by computerised NICU database, PICU paper records, and the neurology clinic database. An electronic case report form was completed for all subjects and controls using data from both paper and electronic medical charts. Information collected included the year of birth, matching criteria, and cooling criteria (cord pH, cord base deficit and Apgar score at 10 min). The presence, time, and volume of BVD was documented for the precooling hours of life (hours 0–6 in the control group), during cooling in 12 hours intervals for 3 days (hours of life 7–78 for controls), rewarming (hours of life 79–86 for controls), and in 12 hours intervals for 48 hours after rewarming was complete (87–134 hours for controls). We also documented verification of NG positioning, use of opioids and muscle relaxants during each time period, and presence of positive blood culture results as a marker of sepsis, as these factors were all considered potential risks for increased BVD. Clinical, investigative, and surgical outcomes of patients who experienced BVD were recorded.
Cooled and non-cooled groups were compared with Pearson's Χ2 analysis, Fisher’s exact test, and t-test. Relative risk and attributable risk were calculated. The OR was reported in order to adjust for NG position, opioid use, muscle relaxant use, and presence of sepsis using logistic regression modelling. For purposes of analysis, an NG tube was considered improperly positioned if its position was not documented and sepsis was defined as positive blood culture.
Logistic regression model reliability was tested using the Hosmer-Lemeshow test. All analyses were completed using SPSS V.23 (IBM, Armonk, New York, USA). Statistical significance was claimed at 95% CI (p<0.05).
This study was approved by the Health Sciences Research Ethics Board of Western University.
Results
Study population
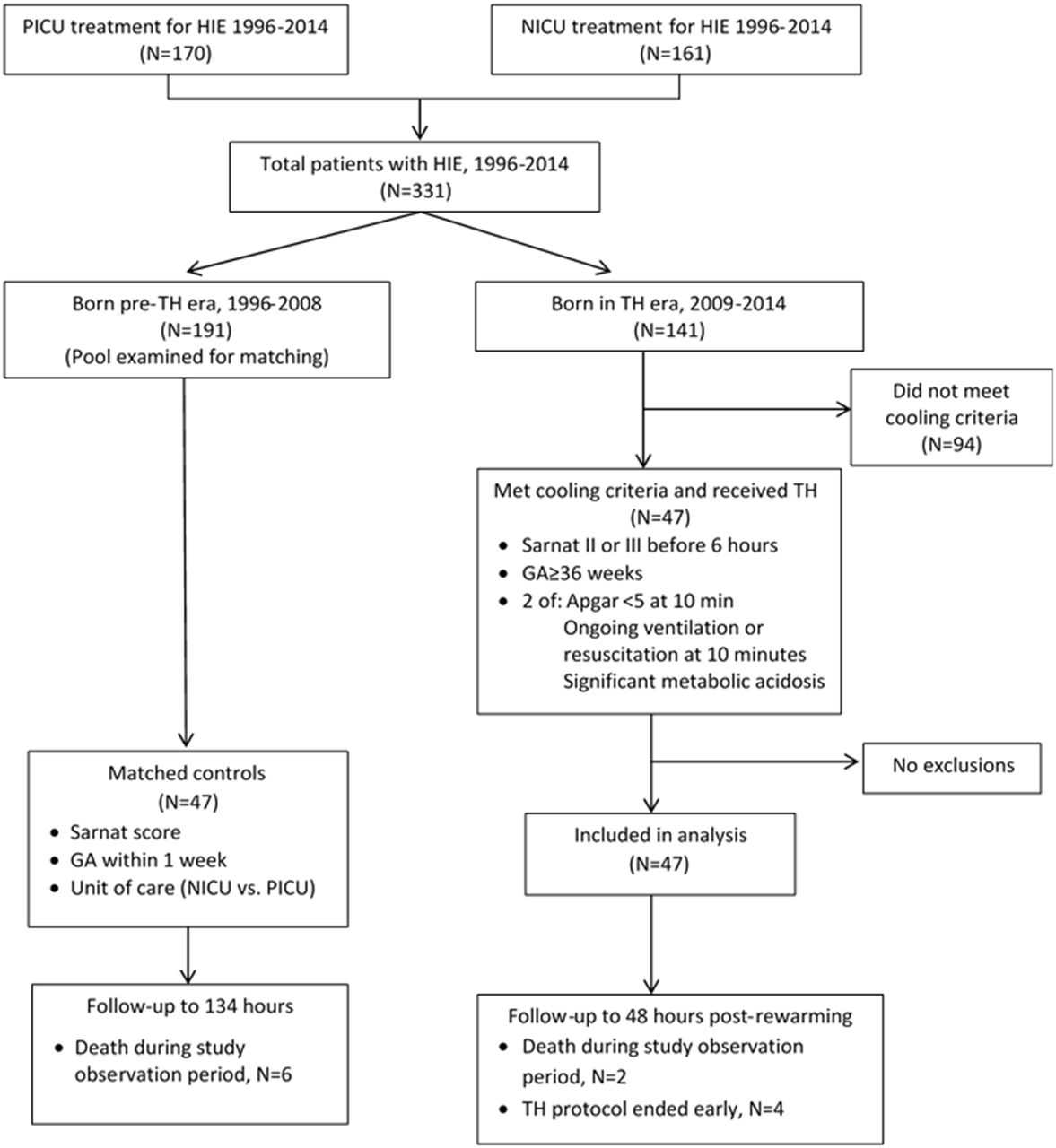
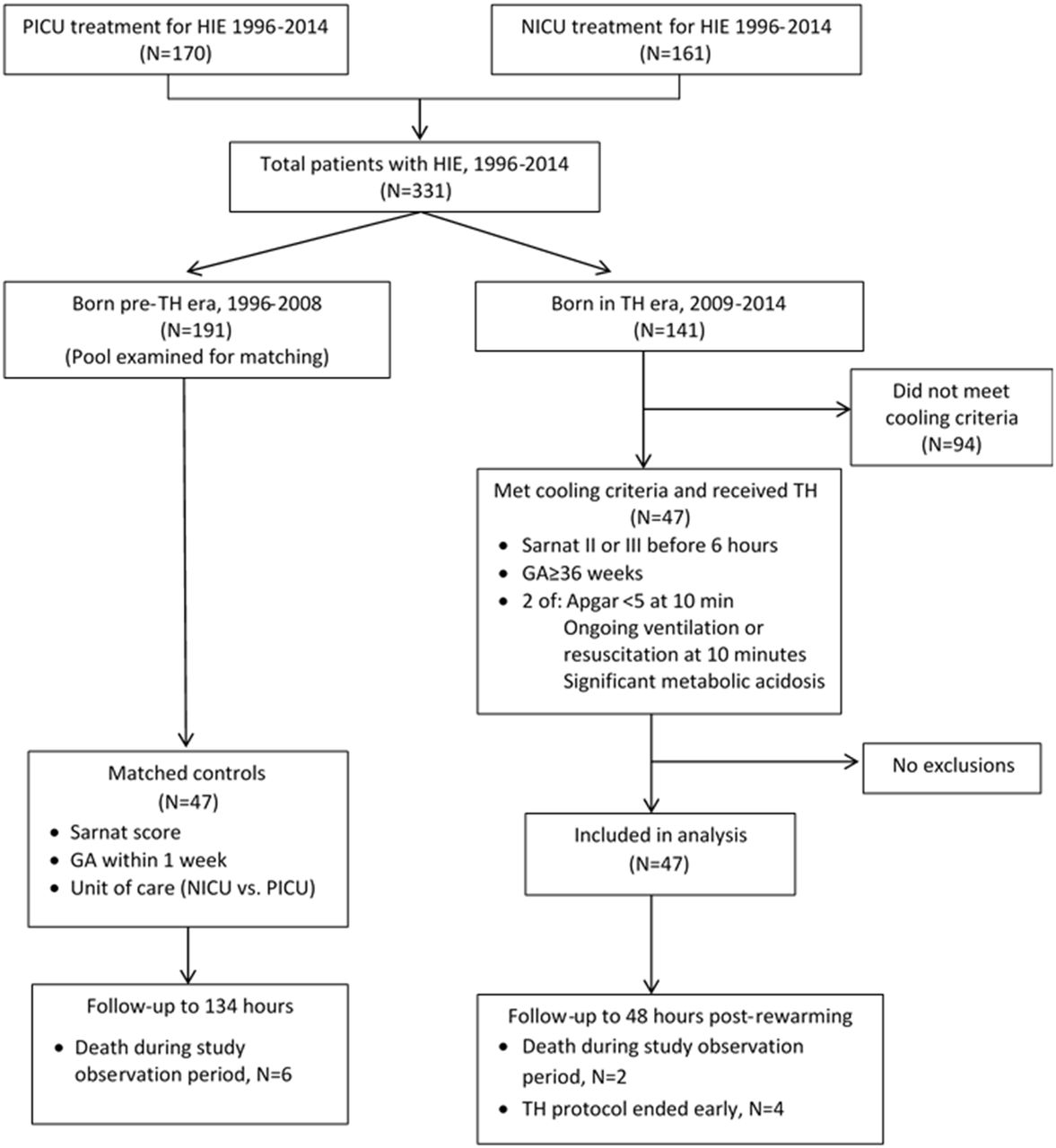
Forty-seven patients met all inclusion criteria. See figure 1 for patient inclusion and flow. Matched controls were identified for each of the study patients, from 2001 to 2008 for patients cared for in PICU and from 1996 to 2008 for patients cared for in NICU. Cases and controls were statistically similar for the observed variables representing baseline demographics and degree of illness (table 1).
{kind=link}
Patient inclusion and flow. TH, therapeutic hypothermia; HIE, hypoxic ischaemic encephalopathy; GA, gestational age; NICU, neonatal intensive care unit; PICU, paediatric intensive care unit.
Baseline characteristics of matched TH and control patients
Based on data availability, the mean (SD) observation time for patients was 129.8 (11.6) hours for the TH group and 125.5 (25.9) hours in the control group (p=0.3) (figure 1).
Patient outcomes
The incidence of bilious vomiting/drainage was significantly higher in patients who received TH (n=12, 26%) than in patients with HIE who were not cooled (n=2, 4%) (p=0.04) (table 2). The relative risk of bilious vomiting and drainage associated with TH was 6.0 (95% CI 1.4 to 25.4). The number needed to treat to create one episode of BVD attributable to TH (number needed to harm) was 5 (95% CI 3 to 14).
Incidence of BVD and presence of potential confounders in TH and control groups
All episodes of BVD occurred during cooling, rewarming, or within 24 hours postcooling. BVD was not associated with the phase of cooling or rewarming (p=0.27). Two patients in the TH group experienced emesis, while all other episodes consisted of bilious NG drainage in both the TH (median volume 15.5 mL, IQR 40 mL) and control (12 and 25 mL for two patients) groups. The unit of care (PICU vs NICU) was not significantly associated with the proportion of patients who experienced BVD (see table 2) in either the TH (p=0.33) or control (p=0.21) groups.
The odds of having bilious vomiting/drainage for patients with TH were increased, OR=7.71 (95% CI 1.62 to 36.74). Incorrect NG position past the pylorus (including NG position not documented within first day of admission), opioid use, muscle relaxant use, and presence of sepsis were all felt to be potential confounders that could increase the risk of BVD (table 2). Accounting for the first three of these potential confounders, the increased risk of BVD with TH persisted, OR=7.8 (95% CI 1.4 to 43.3). This model accounted for between 10.7% and 18.8% of the variance in the presence of any BVD and was found to be a reliable model (p=0.77, Hosmer-Lemeshow test of event rates observed vs rates predicted by the model, where p<0.05 indicates a significant difference) that accurately predicted 75.6% of cases.
Blood cultures were taken and results available in 75 patients (45 patients with TH, 30 control patients) as a surrogate for sepsis. Three patients who received TH and one in the control group had positive blood cultures. No patients with positive cultures experienced BVD (table 2). When including presence of positive blood cultures in the linear regression model, with only 75 patients in the model, the OR for BVD was 11.6 (95% CI 1.2 to 115.0). The model accounted for between 15.0% and 25.7% of the variance in the presence of BVD, and had good reliability in terms of the agreement between the outcome and the predictors (Hosmer-Lemeshow test, p=0.84).
There was no formal hospital protocol for clinical workup of patients experiencing BVD. Of patients with BVD, three patients in the TH group (both patients with vomiting, one patient with drainage) received surgical consult and subsequently had an upper gastrointestinal contrast series performed. One study patient who had concerning radiographic findings received an exploratory laparotomy with no pathology identified. None of the remaining 11 patients with BVD had investigations performed, and there were no notable sequelae during the birth admission to indicate missed pathology. Two study patients and six control patients died during the period of observation (p=0.3, Fisher’s exact two-tailed test), none of whom experienced BVD. Two study patients and three control patients died from non-gastrointestinal causes after the period of observation and prior to hospital discharge.
Discussion
Our study suggests that TH for moderate-to-severe HIE in the neonatal population is associated with an increased risk of non-pathological bilious vomiting and drainage. Therapeutic hypothermia is a widely used neuroprotective strategy for neonates with hypoxic-ischaemic encephalopathy and is associated with improved neurological outcomes.4 11 It should ideally be done with an understanding of the potential complications, including alterations in the extrauterine transition and limitations to normal patient assessment.
Infants with HIE may be at increased baseline risk of BVD. Perinatal asphyxia and the resulting reperfusion period results in abnormal peripheral microcirculation and decreased gastrointestinal perfusion.12 13 Ultrasonography demonstrates a direct correlation between the severity of asphyxia and increased superior mesenteric artery resistive indices lasting up to the third day of life.14 Clinically, this has been seen as decreased feeding tolerance in term infants with HIE compared with controls.15 Vomiting, diarrhoea, gastrointestinal bleeding and necrotising enterocolitis have all been described as complications in neonates following HIE.16 17
The effects of TH on the gut are not well described. Hypothermia decreases cellular metabolic activity (allowing conservation of ATP stores and blunting the effects of anaerobic metabolism), decreases production of pro-inflammatory mediators, and decreases production of free radicals.18–21 In animal models of ischaemia-reperfusion injury focused on gut health, application of TH improved survival, decreased tissue injury to and permeability of the reperfused gut, decreased production of pro-inflammatory modulators, and decreased multiorgan adverse effects.18 19 In humans, improved post-rewarming tolerance of feeding and decreased requirement for tube feedings suggest a theoretical benefit of TH to the gut.22 23 Of note, these outcomes may also be a function of neurological status and not solely related to gut function.
Despite potential long-term benefits, TH may negatively impact gut functioning during active therapy and rewarming. This was first suggested in a case report of intestinal ileus temporally associated with non-therapeutic hypothermia in an infant in 1978.24 Studies of adults undergoing TH for cardiac arrest25 and intracranial haemorrhage26 have demonstrated decreased gut motility. The mechanism for decreased gut function during cooling has been suggested by microcirculatory studies of infants with mild hypothermia during selective head cooling which demonstrate a marked decrease in microcirculatory flow as assessed in the axilla.27 Decreased splanchnic oxygenation and superior mesenteric arterial flow has been demonstrated during the rewarming phase,28 and may account for the BVD seen during rewarming in our cohort.
We have shown that the incidence of bilious emesis or drainage is increased with hypothermia provided by whole body cooling, although it does not appear to be pathological in our patient population, as no patients demonstrated an anatomic cause and we postulate that it improves after rewarming. The previously described complications of TH in the neonatal population—bradycardia and decreased stroke volume29 and renal impairment30 —tend to resolve with rewarming.
Bilious emesis in the neonate tends to be more clinically concerning than drainage from an enteric tube, although both indicate functional or anatomic intestinal obstruction and may herald a surgical emergency if the obstruction is associated with vascular compromise, as is found in midgut volvulus. The clinical conundrum lies in an inability to easily differentiate the underlying cause. The classical triad of bilious vomiting, failure to pass meconium, and abdominal distension is not reliably present in all cases of obstruction. Abdominal tenderness may be absent with volvulus or may be difficult to interpret in a child with neurological compromise or who is receiving pharmacotherapy to tolerate TH. Investigation of bilious emesis with an upper gastrointestinal contrast study to rule out malrotation and midgut volvulus is the standard of care.31 It is noteworthy that only three patients in this study were deemed concerning enough by the clinical service to warrant investigation, although no patients ultimately had surgical pathology.
Although this study was retrospective in nature, it was strengthened by effective case matching and adjusting for potential confounders that may affect bowel motility or might be expected to produce bile in the stomach. The use of historic controls was necessary for the non-TH group. It bears mentioning that the control population for the PICU was taken from 2001 to 2008, while we had to continue back an additional 5 years, to 1996, to find matching patients for the NICU control population. Although the management of feeding tubes was protocolised and consistent across the eras, differences may have existed in feeding practices, ventilation strategies, sedation and pain management, and numerous other care practices. Additionally, examining patients retrospectively from two different eras introduces the risk of detection bias. Patients in the later, TH, era may have been more closely observed both in general and in particular for the presence of BVD if this was unconsciously noted by nursing staff or other physicians prior to identifying the need for a study. Also, while we noted the time to death, it is possible that some of the patients who died either during observation or shortly after had been made palliative with no examination for gastric aspirates, which would represent missed cases of BVD. The study was a single-centre evaluation, which may limit its applicability to other centres, particularly if there are different protocols for managing feeding tubes and feeds. Finally, this evaluation only addressed infants who received whole body cooling, and the incidence and relative risks found may not apply to infants who receive selective head cooling, particularly if the core body temperature achieved in these patients is not as low.
Given the potential for heralding a surgical abdomen, bilious emesis and drainage in the newborn warrants a high index of suspicion, careful consideration, and potentially investigation, particularly if pharmacotherapy precludes an appropriate assessment for an acute, surgical abdomen. Increased bilious emesis and drainage may be an acceptable risk for this therapeutic intervention, but it behoves the clinician to understand common and expected complications.
Conclusion
Therapeutic hypothermia through whole body cooling appears to be associated with non-pathological bilious vomiting or gastric drainage, even when controlled for correct NG positioning, use of opioids and muscle relaxants , and presence of sepsis. Further prospective data are needed to identify the patients in whom investigation and intervention may be avoided.
Acknowledgments
The authors would like to thank Michael Miller and Jacob Davidson for their assistance with statistical analysis.
References
Footnotes
Handling editor Imti Choonara.
Contributors JH co-designed the case report form data collection instrument, completed the data collection, drafted the initial manuscript and approved the final manuscript as submitted. SJ conceptualised and designed the study, critically reviewed and revised the manuscript and approved the final manuscript as submitted. KC conceptualised and designed the study, critically reviewed and revised the manuscript and approved the final manuscript as submitted. SL assisted with non-database patient identification, critically reviewed and revised the manuscript and approved the final manuscript as submitted. JRF conceptualised and designed the study, co-designed the case report form data collection instrument, critically reviewed and revised the manuscript and approved the final manuscript as submitted.
Competing interests None declared.
Ethics approval Western University Health Sciences Research Ethics Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no unpublished data from the study that are available to any other parties.