Article Text

Abstract
Background Training of birth attendants in neonatal resuscitation is likely to reduce birth asphyxia and neonatal mortality. We performed a systematic review and meta-analysis to assess the impact of neonatal resuscitation training (NRT) programme in reducing stillbirths, neonatal mortality, and perinatal mortality
Methods We considered studies where any NRT was provided to healthcare personnel involved in delivery process and handling of newborns. We searched MEDLINE, CENTRAL, ERIC and other electronic databases. We also searched ongoing trials and bibliographies of the retrieved articles, and contacted experts for unpublished work. We undertook screening of studies and assessment of risk of bias in duplicates. We performed review according to Cochrane Handbook. We assessed the quality of evidence using the GRADE approach.
Results We included 20 trials with 1 653 805 births in this meta-analysis. The meta-analysis of NRT versus control shows that NRT decreases the risk of all stillbirths by 21% (RR 0.79, 95% CI 0.44 to 1.41), 7-day neonatal mortality by 47% (RR 0.53, 95% CI 0.38 to 0.73), 28-day neonatal mortality by 50% (RR 0.50, 95% CI 0.37 to 0.68) and perinatal mortality by 37% (RR 0.63, 95% CI 0.42 to 0.94). The meta-analysis of pre-NRT versus post-NRT showed that post-NRT decreased the risk of all stillbirths by 12% (RR 0.88, 95% CI 0.83 to 0.94), fresh stillbirths by 26% (RR 0.74, 95% CI 0.61 to 0.90), 1-day neonatal mortality by 42% (RR 0.58, 95% CI 0.42 to 0.82), 7-day neonatal mortality by 18% (RR 0.82, 95% CI 0.73 to 0.93), 28-day neonatal mortality by 14% (RR 0.86, 95% CI 0.65 to 1.13) and perinatal mortality by 18% (RR 0.82, 95% CI 0.74 to 0.91).
Conclusions Findings of this review show that implementation of NRT improves neonatal and perinatal mortality. Further good quality randomised controlled trials addressing the role of NRT for improving neonatal and perinatal outcomes may be warranted.
Trial registration number PROSPERO 2016:CRD42016043668
- health services research
- mortality
- multidisciplinary team-care
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
What is already known?
A quarter of global neonatal deaths are due to birth asphyxia. The majority of these deaths occur in low-resource settings and are preventable.
Neonatal resuscitation training (NRT) of birth attendants using mannequins result in improved knowledge and skills needed for resuscitation.
Translation of NRT into improved neonatal outcomes and the effect estimates of improvements need to be re-evaluated and updated.
What this study adds?
This meta-analysis assessed the impact of NRT on stillbirths, 1-day neonatal mortality, 7-day neonatal mortality, 28-day neonatal mortality and perinatal mortality.
NRT resulted in significant reduction in stillbirths and early neonatal mortality. However, continuum of care is needed for mortality reduction from day 7 to 28.
Future studies also need to establish the best combination of settings, trainee characteristics and training frequency to sustain the existing effect on perinatal mortality reduction.
Introduction
Approximately a quarter of f million neonatal deaths worldwide are as a result of birth asphyxia.1 A large majority of these deaths occur in low-resource settings and are preventable. Approximately 5%–10% of newborns require some support to adapt to the extrauterine environment and to establish regular respiration.1 2 Simple resuscitative measures are often enough to resuscitate newborns that may even appear to be lifeless at birth. Studies have shown that essential newborn care has been effective in reducing stillbirths (SB).3
In developing countries, measures to improve resuscitative efforts through training of basic steps of neonatal resuscitation are expected to reduce birth asphyxia and neonatal mortality. Numerous studies have suggested that imparting neonatal resuscitation training (NRT) to healthcare providers involved in delivery process and handling of newborns has the potential to save newborn lives in low-income and middle-income settings4–10
Improvements in knowledge and skills of trainees following training programme in resource-limited settings have been reviewed. However, the impact on perinatal mortality outcomes has not been updated in last 5 years.9 The effect estimates of mortality reduction as a result of training of healthcare providers involved in delivery process and handling of newborns needs to be updated to inform hospital administrators and policy-makers the importance of investing in NRT to sustain and improve neonatal survival. A previous systematic review and meta-analysis11 assessed knowledge, skills, neonatal morbidity, neonatal mortality in first 7 days after birth and from day 8 to 28. However, it did not include outcomes of stlillbirth, 1-day neonatal mortality or perinatal mortality which has been included in our review.
The objective of this review is to assess the impact of NRT programme in reducing stillbirths, 1-day neonatal mortality, 7-day neonatal mortality, 28-day neonatal mortality and perinatal mortality.
Materials and methods
Inclusion criteria
Types of studies
We included relevant randomised, quasi-randomised controlled trials, interrupted time series studies and before–after studies regardless of language or publication status.
Types of participants (population) trained
We considered studies where NRT was provided to healthcare providers (including neonatologists, physicians, nurses, interns, midwives, traditional/community birth attendants, auxillary nurse midwives, village health workers, paramedics) involved in delivery process and handling of newborns in a community (home-based, rural and village clusters) or a hospital (including district hospitals, health centres, dispensaries, teaching/university hospitals, regional hospital, delivery/health centres, local hospitals and tertiary care hospital) setting.
Types of interventions and comparison
Studies in which any NRT was compared with a control group (that received no NRT) or compared with data before the study (pre-NRT vs post-NRT) were included. For this purpose, we considered any NRT programme of healthcare professionals, including the American Academy of Pediatrics’ (AAP) Neonatal Resuscitation Program (NRP), Helping Babies Breathe (HBB) or any other training programme that had NRP or HBB as a clearly mentioned component of training methodology.
Types of outcomes measures
We included following outcomes in the review:
Stillbirths: defined as number of deaths prior to complete expulsion or extraction of products of conception from its mother.
Fresh stillbirth: clinically defined as those deaths with no signs of life at any time after birth and without any signs of maceration.
1-day neonatal mortality: defined as number of deaths in first 24 hours of life
7-day neonatal mortality: defined as number of deaths in first 7 days of life
Perinatal mortality: defined as number of stillbirths and deaths in the first week of life.
28-day neonatal mortality: defined as number of deaths in the first 28 days of life.
Search strategy
We searched following electronic databases from inception to July 2016: MEDLINE (PubMed), The Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library); Education Resources Information Centre (ERIC), Web of Science, Science Citation Index and Scientific Electronic Library Online. The search strategies for PubMed and CENTRAL can be found in supplementary files S1 and S2 respectively. We also searched for ongoing trials at www.clinicaltrials.gov and www.controlled-trials.com. We searched published abstracts of conferences and examined bibliographies of retrieved articles for additional studies. We contacted and requested experts and authors in this field to provide possible unpublished work.
Study selection and data extraction
Screening of studies
Two reviewers (MNK and AB) independently examined studies identified by literature search; discarded articles that did not fulfil the inclusion criteria and assessed full texts of all relevant articles for inclusion. A third reviewer (AP) resolved disagreement among the primary reviewers.
Data extraction and management
For all studies that fulfilled the inclusion criteria, two reviewers (KK, SB) extracted data (table 1 and 2). Third review author (AP) cross-checked the data and resolved discrepancies. For studies where required data was lacking or could not be calculated, we requested the corresponding author for details.
Characteristic of included studies
Assessment of risk of bias in included studies
Two authors (SB, KK) independently assessed risk of bias for each study using criteria suggested by Cochrane Effective Practice and Organization of Care (EPOC)12 and using criteria outlined in Chapter 8 of Cochrane Handbook for Systematic Reviews of Interventions.13 Disagreements were resolved by discussion with the third reviewer (MNK).
Data analysis
Measures of treatment effect
We conducted meta-analysis and reported pooled statistics as risk ratios (RR) with 95% confidence interval (CIs) for dichotomous data. We followed recommendations of the Cochrane Handbook for Systematic Reviews of Interventions Sections 9.2 and 9.4 for measuring the effects.13
Assessment of heterogeneity
We assessed heterogeneity amongst studies by inspecting forest plots for the overlap of confidence intervals, analysed statistical heterogeneity through Χ2 test (P value >0.10) and quantified through I2 statistics(Chapter 9.5 of Cochrane Handbook for Systematic Reviews).13 We regarded heterogeneity as substantial if in the Χ2 test for heterogeneity there was either I2>50%, or P value <0.10. We interpreted I2 values between 0% and 40% as possibly unimportant, 30% and 60% as possibly significant, 50% and 90% as possibly substantial and 75% and 100% as possibly considerable.
Assessment of reporting bias
We used funnel plots for assessment of publication bias if ten or more studies were included in a meta-analysis.
Data synthesis and analysis
We analysed the data using Review Manager V.5.3 software.14 We conducted meta-analyses for individual studies and reported pooled statistics as relative risk (RR) between experimental and control groups with 95% CI. We explored possible clinical and methodological reasons for heterogeneity, and in the presence of significant heterogeneity, we carried out sensitivity analysis and employed inverse-variance method with Random-effects model. We did not pool randomised and non-randomised (pre–post NRT) studies in the same meta-analysis.
Summary of findings table
We created ‘summary of findings’ (SoF) table using five GRADE considerations (study limitations, consistency of effect, imprecision, indirectness and publication bias) to assess the quality of a body of evidence. We used methods and recommendations described in Chapter 12 of the Cochrane Handbook for Systematic Reviews of Interventions13 using GRADEpro software.15 GRADE working Group grades of evidence were used in the SoF.16
Results
Search results
We identified 148 records through database searching and 11 records through other sources. After initial screening on the basis of title and abstract, we assessed 47 full-text articles for eligibility and finally included 20 articles in the meta-analysis. The screening details are presented in a Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram (figure 1).

Flow diagram of the study selection process. NRP, Neonatal Resuscitation Program.
Included studies
Amongst included studies, two randomised trials addressed the efficacy of NRT in improving neonatal and perinatal outcomes, whereas 18 were pre–post studies. A full description of each study is included in table 1 and 2. All studies were from low-income and middle-income countries. Four studies were done in community setting, whereas 16 studies were carried in hospital setting.
Characteristic of included studies (training and outcomes)
Carlo et al 17 18 assessed baseline perinatal outcomes, then imparted Essential Newborn Care (ENC) training to all which also included basic steps of NRT. They then randomised all clusters that had received ENC training into two groups. One group received an in-depth NRT while the other group did not (control group). For this study we evaluated the pre-ENC outcome of all clusters and compared them to outcomes of those clusters that received ENC +post ENC in-depth NRT. We therefore did not include this study in the NRT versus control analysis because the control group had also received NRT as a part of ENC training.
The study from Kenya had a complex design of randomisation of health workers to two groups—early training (phase I) or late training (phase II) and did not include a control group without training.19 Therefore, we analysed this study as before–after study where the rate of stillbirths prior to any training were compared with the rate of stillbirths after all phases of training.
Participants of the NRT programme differed across studies and included village health workers, community birth attendants,17 18 20 community birth attendants/traditional birth attendants,21 hospital-based birth attendants,19 22–26 or hospital-based birth attendants including high-level and mid-level staff/specialists.27–34
Different types of training employed by studies included AAP, HBB or NRP curricula23 24 27 31 32 34 35 AAP/American Heart Association (AHA),21 24 26 basic neonatal resuscitation and ENC,17–19 25 home-based neonatal care, basic training with mouth to mask or tube and mask resuscitation,35 Advanced Life Support in Obstetrics (ALSO),29 Bulgarian program on NRT.30 The duration of NRT also differed acrossstudies.
We also included two unpublished trials after permission from authors (tables 1 and 2).
Excluded studies
Studies that included interventions that did not qualify as NRT were excluded from the review. These included trainings in safe birthing techniques,36 Emergency Obstetric and Neonatal Care (EmONC),37 38 ENC,39–41promotion of antenatal care and maternal health education,42and newborn care intervention package.43
Other interventions that did not qualify as NRT44–50 or included interventions like neonatal intensive care unit/special neonatal care unit training51 52 were also excluded.
Studies in which desired outcomes (fetal and neonatal outcome) were not assessed,53–58 or only trainees/training outcomes were assessed,59–73 were also excluded from the analysis.
Some studies that were subgroups of larger studies like Ersdal et al.74 75 (subgroup of Msemo et al 22), Matendo et al 76(subgroup of Carlo et al 18), Matendo et al 76 and Vossius et al 77 (subgroup of Msemo et al 22) were also not included. However, Vossius et al 77 was included in the analysis for outcomes where data from22 Msemo et al 22 were not available.
Risk of bias in included studies has been depicted in table 3.
Risk of bias assessment across studies
Effects of interventions
Neonatal and perinatal outcomes were reported in majority of included studies. The overall analysis showed a trend towards reduction in neonatal deaths, early neonatal deaths, perinatal deaths and stillbirths with NRT; most of which are statistically significant.
NRT verses control
The meta-analysis for NRT verses control shows that NRT decreases the risk of all stillbirths by 21% (RR 0.79, 95% CI 0.44 to 1.41; participants=5661; studies=2; I2=67%) (figure 2), 7-day neonatal deaths by 47% (RR 0.53, 95% CI 0.38 to 0.73; participants=5518; studies=2; I2=0%) (figure 3), 28-day neonatal deaths by 50% (RR 0.50, 95% CI 0.37 to 0.68; participants=5442; studies=2; I2=0%) (figure 4), and perinatal deaths by 37% (RR 0.63, 95% CI 0.42 to 0.94; participants=5584; studies=2; I2=68%)(figure 5). The effect was significant for ay 7-day neonatal mortality , 28-day neonatal mortality and perinatal mortality . Significant heterogeneity was observed in analysis of total stillbirths and perinatal mortality.

Forest plot comparing all SB between the NRT and the control groups. NRT, neonatal resuscitation training; SB, stillbirths.

Forest plot comparing 7-day neonatal mortality between the NRT and the control groups. NRT, neonatal resuscitation training.

Forest plot comparing 28-day neonatal mortality between the NRT and the control groups. NRT, neonatal resuscitation training.

Forest plot comparing perinatal mortality between the NRT and the control groups. NRT, neonatal resuscitation training.
The grade of quality of evidence for the meta-analysis of the trials was moderate to high (table 4).
Summary of findings for NRT versus control groups
Post-NRT verses pre-NRT
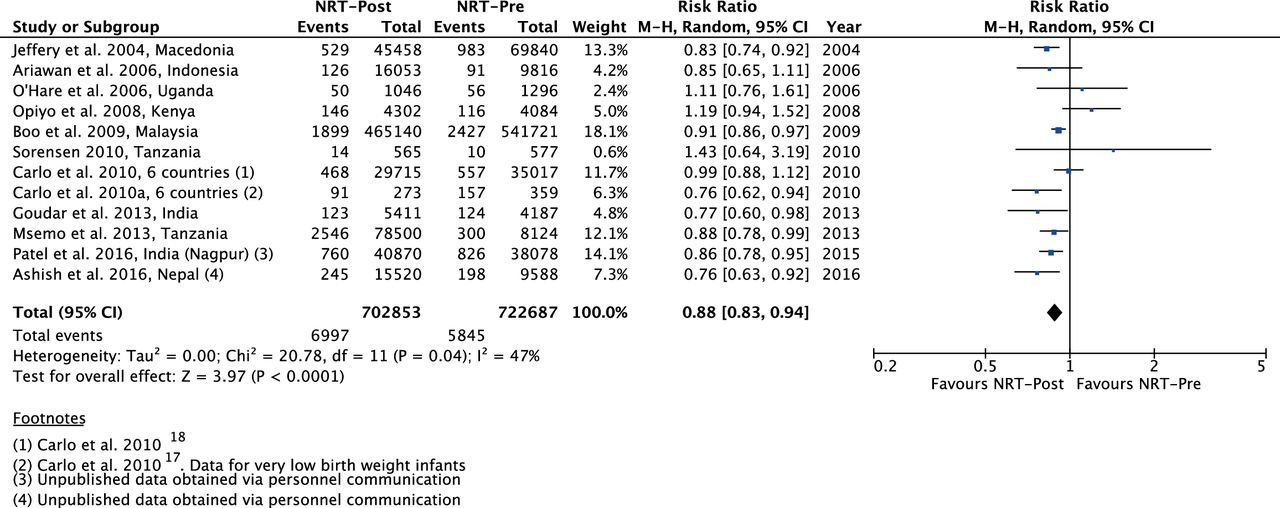
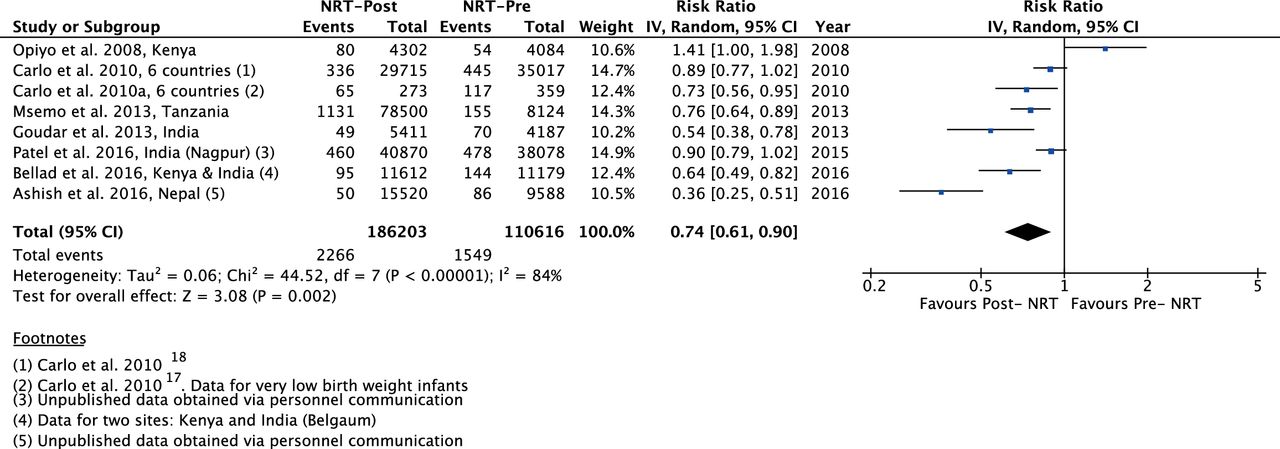
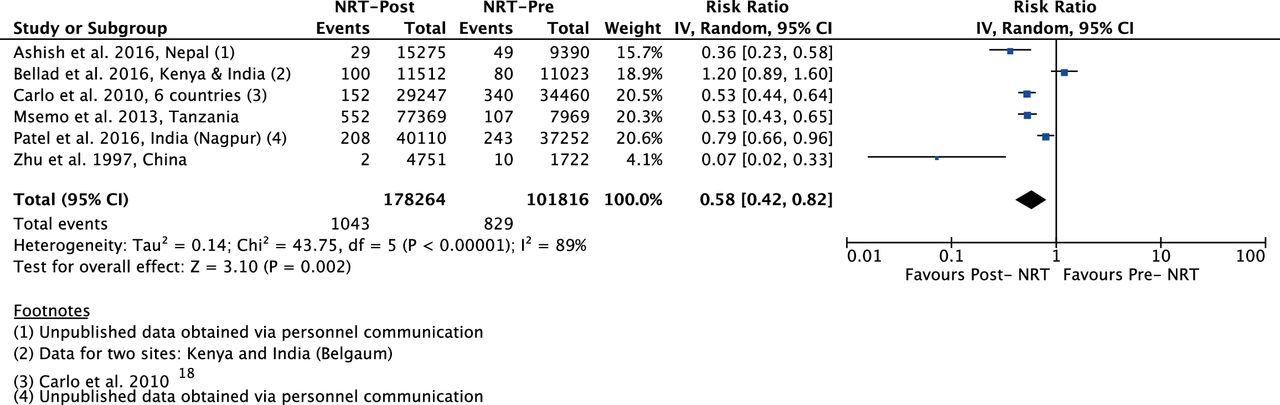
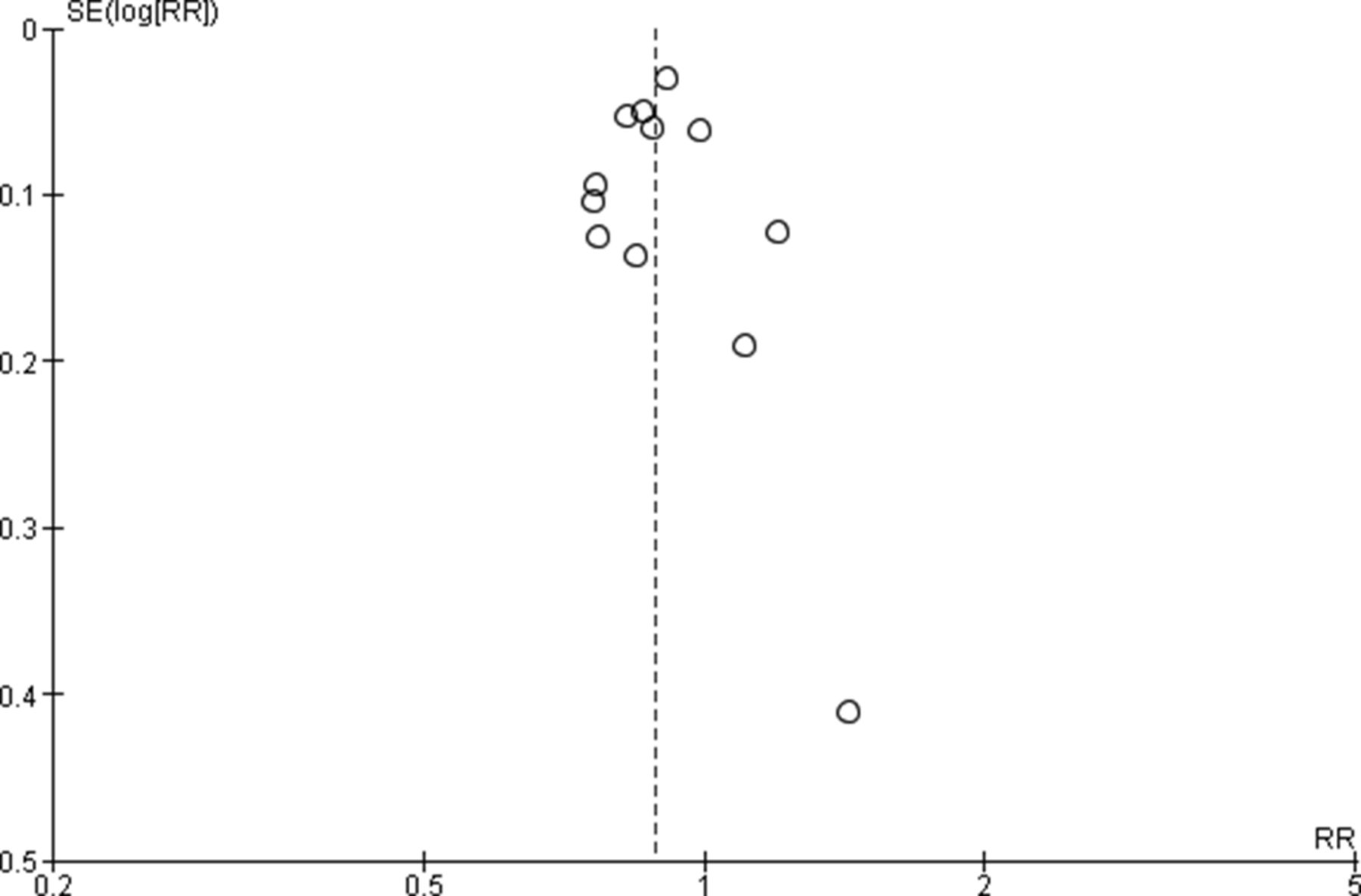
The meta-analysis of post-NRT verses pre-NRT shows that post-NRT decreases the risk of all stillbirths by 12% (RR 0.88, 95% CI 0.83 to 0.94; participants=1 425 540; studies=12; I2=47%, figure 6), fresh stillbirths by 26% (RR 0.74, 95% CI 0.61 to 0.90; participants=296 819; studies=8; I2=84%, figure 7), 1-day neonatal mortality by 42% (RR 0.58, 95% CI 0.42 to 0.82; participants=280 080; studies=6; I2=89%, figure 8), 7-day neonatal mortality by 18% (RR 0.82, 95% CI 0.73 to 0.93; participants=360 383; studies=7; I2=71%, figure 9), 28-day neonatal mortality by 14% (RR 0.86, 95% CI 0.65 to 1.13; participants=1 116 463; studies=7; I2=95%, figure 10) and perinatal mortality by 18% (RR 0.82, 95% CI 0.74 to 0.91; participants=1 243 802; studies=6; I2=90%, figure 11). The changes were significant in all the outcomes; except 28-day neonatal mortality. Heterogeneity was significant in all outcomes except all stillbirths. We created a funnel plot for all stillbirths , which showed asymmetry, thereby indicating a publication bias (figure 12).
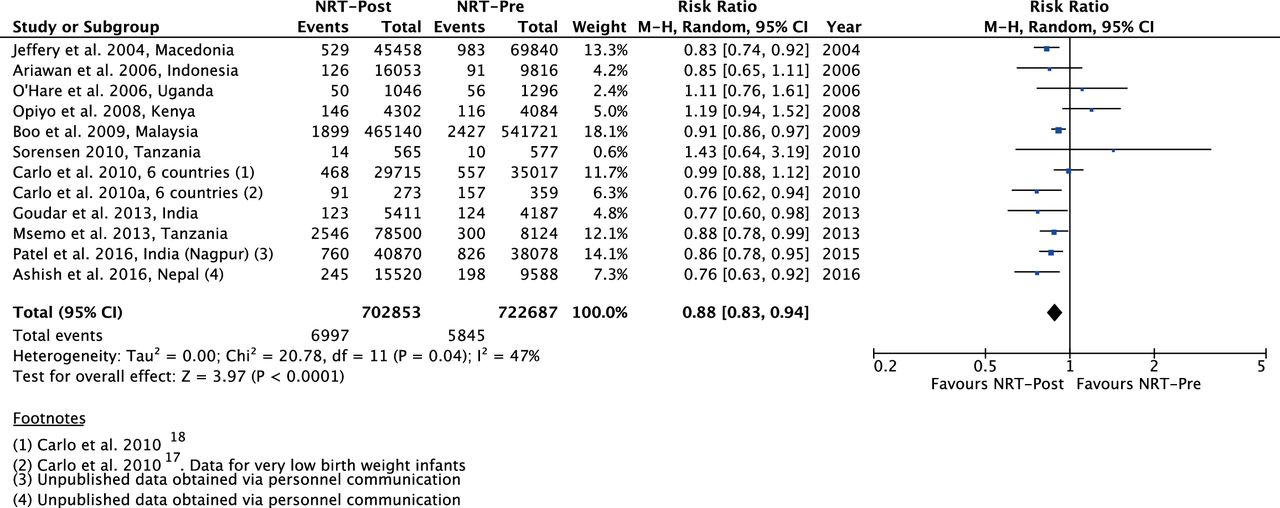
Forest plot comparing all SB between the post-NRT and the pre-NRT groups. NRT, neonatal resuscitation training; SB, stillbirths.
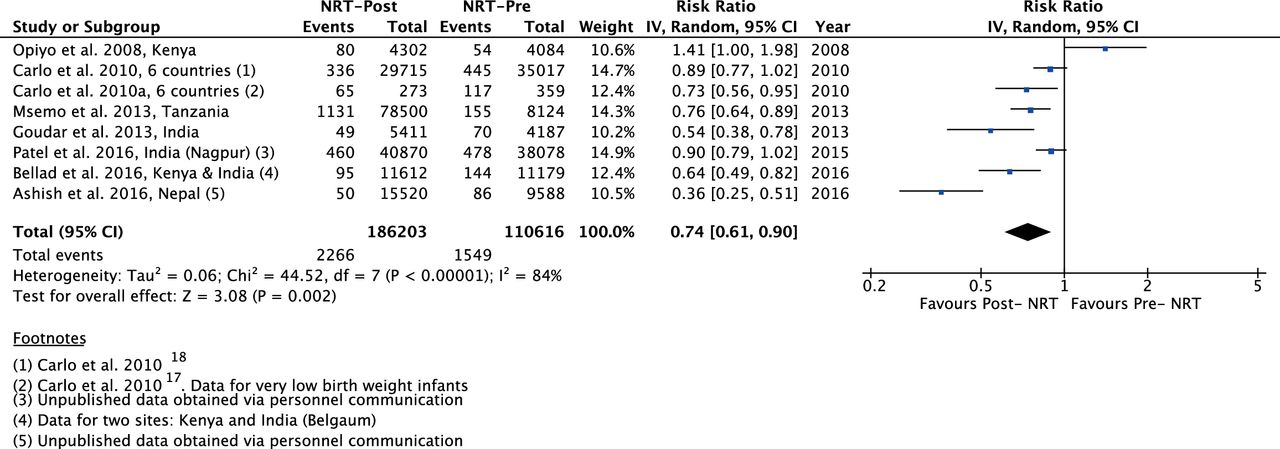
Forest plot comparing fresh SB between the post-NRT and the pre-NRT groups. NRT, neonatal resuscitation training; SB, stillbirths.

Forest plot comparing 1-day neonatal mortality between the post-NRT and the pre-NRT groups. NRT, neonatal resuscitation training.

Forest plot comparing 7-day neonatal mortality between the post-NRT and the pre-NRT groups. NRT, neonatal resuscitation training.
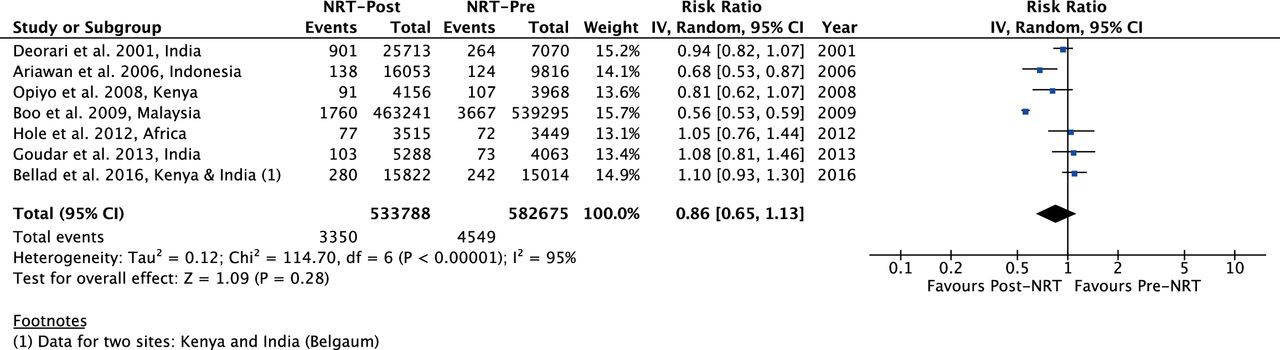
Forest plot comparing 28-day neonatal mortality between the post-NRT and the pre-NRT groups. NRT, neonatal resuscitation training.

Forest plot comparing perinatal m between the post-NRT and the pre-NRT groups. NRT, neonatal resuscitation training.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Funnel plot of comparison: Post-NRT verses pPre-NRT for all SB. NRT, neonatal resuscitation training; RR, risk ratio; SB, stillbirths.
The quality of evidence for NRT verses control was very low for SB and 1-day neonatal mortality, high for 7-day and 28-day neonatal mortality and moderate for perinatal mortality (table 4). The quality of evidence for post-NRT verses pre-NRT was very low for all our outcomes (table 5).
Summary of findings for Post-NRT versus Pre-NRT groups
Discussion
This meta-analysis assessed the impact of any NRT programme either by itself or as a part of newborn care package on rates of stillbirths, perinatal mortality, all-cause neonatal mortality on day-1, up till day-7 and till 28th day after birth. We did not evaluate intrapartum-related neonatal deaths or asphyxia/cause-specific neonatal mortality. Mortality in neonates <7 days of life is a proxy measure for intrapartum-related deaths.43 78 Meta-analysis of before–after studies showed a significant reduction in all stillbirths by 12% (12 studies) and of FSB by 26% (8 studies). The reduction in fresh stillbirths can be attributed to NRT that helps in resuscitating neonates that appear lifeless at birth.17 18 Of 12 studies, seven studies reported a significant and one study reported a non-significant reduction in fresh stillbirths. However, a non-significant increase in risk of stillbirths was reported in three African studies which blunted the impact of NRT on reduction of stillbirths.
There was reduction in 1-day mortality of 42% (6 studies) and that of 7-day mortality was 18%. All studies included in the analysis (figures 8 and 9) showed a reduction with an exception of one study.27 Failure to observe reduction in mortality in Bellad et al could be due to two reasons. First, NRT was provided in diverse health systems within a short period of time. Second, mortality was not assessed in facilities where training was imparted but was measured in the population.
The meta-analysis showed a non-significant reduction of 14% in 28-day mortality. Of the seven included studies only two studies reported a significant reduction in mortality. Resuscitation at delivery helps to reduce neonatal mortality in the first hour of birth when the neonate is at the highest risk of intrapartum-related deaths3 and the impact diminishes subsequently. For reduction of 28-day neonatal mortality, post-resuscitation specialised care for survivors is required and only NRT is unlikely to have the desired impact on 28-day neonatal mortality.79 80
Trials that randomise facilities to NRT versus controls (where NRT is not a standard practice) would be ideal to assess the reduction in neonatal mortality. Trials are also likely to result in higher impact as compared with before–after studies as other changes at health facilities or in communities during the time period of before–after studies can confound the results. Because NRT is a standard practice and randomising individuals or clusters to no resuscitation training is unethical, there were only two trials available for the meta-analysis.20 21 They showed a reduction of 7-day neonatal mortality and 28-day mortality by 47% (figure 3) and 50% (figure 4), respectively. The perinatal mortality reduced by 37% (figure 5) with no significant reduction in SB rates.
Previously, an expert panel published a systematic review for community-based studies and conducted a meta-analysis that evaluated whether NRT reduced all-cause neonatal mortality in th first 7 days of life. They reported a 38% reduction in mortality which is larger than the 18% (7 studies) reduction observed in the current meta-analysis. Our meta-analysis included community-based studies that resulted in a smaller effect size. Community-based studies (trials or before–after) report a smaller reduction effect on any day neonatal mortality.8 17 18 47 The reduction in effect size of neonatal mortality in these studies can arise due to several reasons. All births in the intervention community may not be attended by birth attendants trained in neonatal resuscitation, especially if it is a home delivery.81 82 Second, women may decide to deliver at facilities or homes outside communities where NRT has been imparted. Finally, assessing mortality outcomes in the community can be challenging. Another meta-analysis11 was published in Cochrane which evaluated outcomes such as knowledge, skills, neonatal morbidity, neonatal mortality in first 7 days after birth and from day 8 to 28. This analysis did not include stillbirths, 1-day neonatal mortality or perinatal mortality that was included in the current meta-analysis.
The current meta-analysis consists largely of before–after studies with lack of concurrent control group that limits isolation of effect of resuscitation training alone from other changes at health facilities or in communities during the time period. Other limitation is lack of consistency of settings, duration of training, varying study designs and lack of consistent outcomes which contributed to substantial heterogeneity. Lack of subgroup analysis of type of health facilities may be perceived as a limitation. An improvement in mortality would be maximised in low-resource settings with poor quality of care. However, it is presumed that there is regular training of health workers in basic resuscitation skills in higher levels of care that would translate to higher quality of care. Our recent study83 84 that evaluated the knowledge and skills of trainees trained in HBB included 384 tertiary-level facilities in India. Only 3% of physicians and 5% of nurses were able to pass the pre-training bag and mask resuscitation skill assessment.84 Therefore, in the absence of reporting of pre-training skills of health workers in low-resource or high-resource settings or any indicator of quality of care, it would be erroneous to conduct a subgroup analysis based merely on resource settings and mostly will not change the results or the main message of this meta-analysis. We emphasise that despite the heterogeneity in settings, type of training, type of trainees, type of trainers and the duration of training, this study showed an improvement in mortality at and soon after birth.
To conclude, NRT resulted in reduction in stillbirths and improved survival of newborns. The impact on survival of newborns can be further improved by providing a continuum of care beyond 7 days which is not addressed by NRT alone.
The meta-analysis performed showed beneficial effect of NRT in improving neonatal and perinatal outcomes. The models of training were not consistent across studies, with variations in training, trainee and setting. Generalisation of results of the pooled analysis to many currently available programme may not be appropriate. There was evidence of heterogeneity across studies in our meta-analyses; however, overall there is consistency in the direction of effect.
This review identified several important limitations of the current evidence from included studies. Due to inadequate information about the methodology followed and variety of resuscitation programmes in included studies, the quality of the evidence was downgraded for risk of bias and indirectness resulting in inability to adequately assess the effects of this intervention.
Conclusions
Implications for practice
This review shows that the implementation of NRT improves neonatal and perinatal outcomes.
Implications for research
Further good quality, multicentric randomised controlled trials addressing the role of NRT for improving neonatal and perinatal outcomes may be warranted. Impact of NRT on improving neonatal and perinatal outcomes as well as the best combination of settings and type of trainee should be established in future trials. More studies need to be done to assess the frequency with which NRT needs to be conducted to sustain the existing effect on perinatal mortality reduction.
Acknowledgments
The authors wish to acknowledge Richard Kirubhakaran (Research Scientist, Cochrane South Asia, Prof B V Moses Centre for Evidence-Informed Healthcare & Health Policy, Christian Medical College, Vellore) for his inputs on meta-analysis and Lauren Arlington, Partner Healthcare, for her help in getting the full text of the articles required for this review.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
Footnotes
Contributors AP: conception of the work, design of the work, manuscript drafting with final approval of the version to be published. MNK: developed and run the search strategy, screened and selected studies, and did meta-analysis, GRADE assessment and manuscript drafting. KK and SB: involved in preparation of characteristic of studies table, data acquisition and manuscript drafting. AB: screening and selection of studies, data acquisition and manuscript drafting.
Funding This work was supported by Lata Medical Research Foundation, Nagpur, India (Grant no: LMRF/GRP02/072016).
Competing interests The authors AP and AB were investigators in two of the studies (Bellad et al and Patel et al) included in the meta-analysis. There were no other competing interest.
Provenance and peer review Not commissioned; externally peer reviewed.