Article Text

Abstract
Objective Prolonged neonatal jaundice is common and usually benign; however, assessment of bilirubin fractions is recommended to determine the need for further assessment for congenital liver disease, particularly biliary atresia. The direct (conjugated) bilirubin thresholds currently used are variable and poorly evidenced. Hence, we aimed to delineate direct bilirubin levels in disease-free neonates with prolonged jaundice.
Methods We performed a retrospective cohort analysis of split bilirubin levels, and subsequent follow-up, for all neonates initially assessed in our prolonged neonatal jaundice clinic over 2 years. We plotted centile charts for total, direct and direct–total bilirubin ratio levels against age at sampling. The association was assessed using linear regression analysis.
Results Data were collected for 420 neonates (501 blood samples) across an age range of 10–70 days. No significant liver disease was found. For each day of older age, total bilirubin fell by 3.72 µmol/L (95% CI 2.46 to 5.00) and direct bilirubin fell by 0.39 µmol/L (0.18 to 0.59). The ratio between the two did not change significantly (−0.0006 to +0.0034). The 95th centile for direct bilirubin was stable at ~25 µmol/L. Direct–total bilirubin ratio was very variable with some 95th centiles >30%.
Conclusions In a clinically relevant population of disease-free neonates with prolonged jaundice both the total and the direct bilirubin decreased with age. The absolute direct bilirubin is more useful clinically than the direct–total bilirubin ratio. Our results support National Institute for Health and Care Excellence guidance that conjugated bilirubin >25 µmol/L, or even more stringent criteria, constitutes an appropriate threshold for further investigation for neonatal liver disease.
- hepatology
- jaundice
- metabolic
- neonatology
- biochemistry
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Biliary atresia and other congenital liver diseases are distinguished from physiological prolonged neonatal jaundice as they are associated with conjugated (direct), rather than unconjugated, hyperbilirubinaemia.
The natural history of the total bilirubin level in the first 4 weeks of life in disease-free neonates is to decrease over time.
The criteria currently recommended for further investigation in cases of prolonged neonatal jaundice are variable and supported by little evidence.
What this study hopes to add?
In disease-free states, direct bilirubin decreases with age, particularly at the level of the individual. We produce centile charts that may serve as reference tools.
However, the direct–total bilirubin ratio shows no clear trend and thus is an unreliable marker of serious pathology, including congenital liver disease.
Our data support the NICE guidance advocating investigation for liver disease in neonates with conjugated bilirubin >25 µmol/L, although more stringent criteria may also be valid.
Background
Prolonged neonatal jaundice is yellowing of the skin and sclerae, secondary to hyperbilirubinaemia, persisting beyond 14 days after birth. It is very common—20–30% of breastfed neonates are still jaundiced at 1 month1—and is usually transient and benign; however, it can be an important indicator of serious underlying pathology.2 The most common cause is physiological jaundice (especially in breastfed neonates), but a number of disease processes must be excluded, including haemolysis, sepsis, hypothyroidism, cystic fibrosis, metabolic disease and liver disease (mainly congenital hepatitis B/C or biliary atresia).3 It is particularly important to diagnose biliary atresia as, although rare, it is the only cause that is usually asymptomatic but in which early specialist assessment and surgery (Kasai portoenterostomy; ideally within 6–8 weeks of age) are crucial for prognosis.4 The abnormality of the biliary tree causes an obstructive jaundice with conjugated (direct) hyperbilirubinaemia, whereas physiological jaundice and almost all other pathological causes result in a predominantly unconjugated hyperbilirubinaemia.5
Current National Institute for Health and Care Excellence—the primary publisher of UK clinical guidelines (NICE)—guidance is that the cause of prolonged jaundice requires investigation and referral for any neonate with a conjugated hyperbilirubinaemia >25 µmol/L, but this is based on no referenced data.2 The North American Society for Pediatric Gastroenterology, Hepatology and Nutrition (NASPGHN) recently released an updated guideline in collaboration with their European Society (ESPGHN) recommending further investigation under the definition of an abnormal direct bilirubin (a slight overestimate of conjugated bilirubin—see the Methods section) as >1.0 mg/dL (17.2 µmol/L).6 Their previous guideline, which also incorporated the direct–total bilirubin ratio, acknowledged that their thresholds are based on ‘lower quality studies’.7 And they now state that the move away from using the ratio is for simplicity rather than any novel evidence.6
We therefore sought to re-evaluate the poorly evidenced thresholds through characterising the natural history of both total and direct bilirubin levels. Total bilirubin levels have previously been shown to decrease reverse-exponentially with age in disease-free neonates,1 but to our knowledge the variation of direct bilirubin levels with age in this population is yet to be characterised (explaining the lack of evidence behind NICE’s 25 µmol/L cut-off).2 Hence, our aims were to establish the spread of direct bilirubin levels in our sample and concordantly inform national guidance for the investigation of prolonged neonatal jaundice.
Methods
Sample population and data collection
We performed a retrospective cohort study of the last 460 neonates who attended the prolonged neonatal jaundice clinic at the Royal Free Hospital (from December 2012 to November 2014). The community midwives were to refer all neonates who were visibly jaundiced at 14 days. The neonates referred were approximately 8% of the neonates in the community midwifery service. A paediatric nurse assessed all the neonates and took venous blood for split (total and direct) bilirubin. Further follow-up was arranged based on these results by criteria that, due to lack of confidence in local and national guidance (the impetus for this work), were decided by the responsible clinician on a case-by-case basis. The neonates’ date of birth and the results and dates of the initial split bilirubin as well as any further bilirubin measurements and further investigations (up until May 2015) were extracted from the hospital database and compiled. All these further investigations were assessed for abnormalities that may indicate underlying pathology (with particular focus on liver function tests and ultrasound imaging).
Statistical analysis
To analyse trends at the population level, we calculated the age at time of testing from each neonate’s date of birth and the date of their split bilirubin measurement(s). The software used was SAS v9.3. The majority of our neonates were aged 14–30 days at testing (range 10–70). Table 1 shows the bilirubin measurements by age band, expressed as centiles. On testing (via histogram and Q-Q plot as well as numerical analysis with logarithmic conversion for direct–total bilirubin ratio), the data were found to be normally distributed. We therefore plotted centile charts using mean and SD values (figure 1).
Centiles (95% CI—calculated using bootstrapping with 5000 repetitions) of split bilirubin levels (µmol/L) by age group at measurement—summary of raw data

{kind=link}
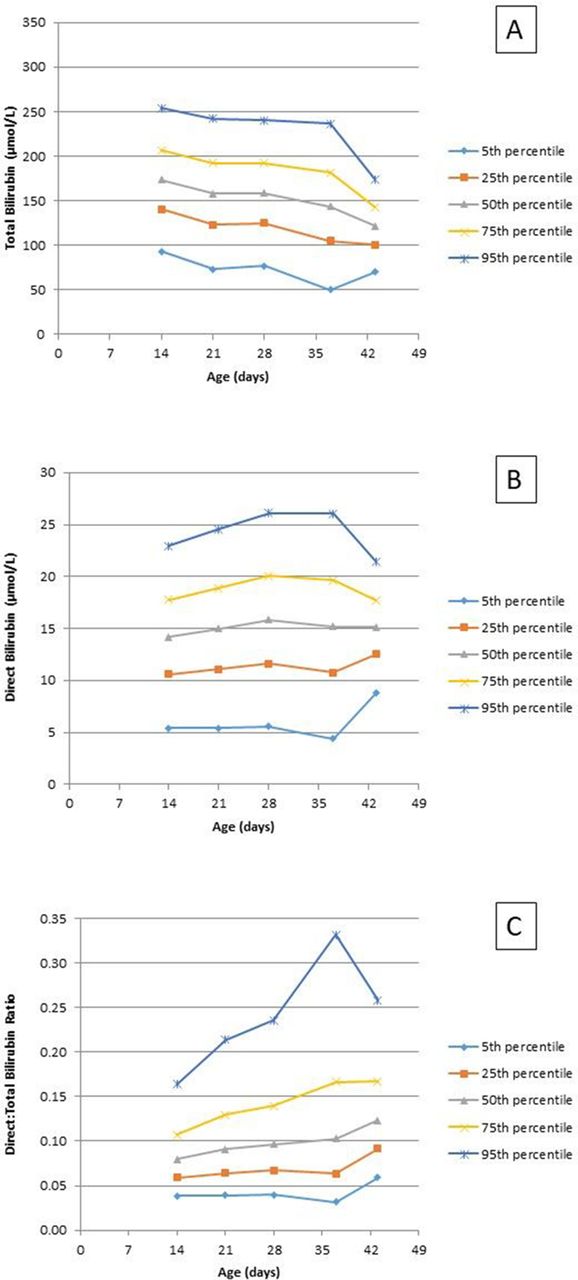
Bilirubin centile charts versus age at measurement calculated from mean and SD values (assuming normal distribution). (A) Total bilirubin, (B) direct bilirubin and (C) direct–total bilirubin ratio.
We also used linear regression to assess the association between bilirubin and age for all samples between 10 and 42 days (96.8% of all samples), incorporating general estimating equations to account for some neonates having more than one measurement.
Lastly, some neonates had two time-separated split bilirubins which allowed for limited analysis at the individual level.
Biochemistry
Total and direct bilirubin on all samples was measured using the Roche/Hitachi 902 which employs diazo methods. Bilirubin in plasma exists in three forms: unconjugated bilirubin (reversibly bound to albumin; usually the major component), free conjugated bilirubin and delta bilirubin (conjugated bilirubin covalently bonded to albumin; normal range approximately 0.0–3.0 µmol/L). Using diazo methods for direct bilirubin, both conjugated and delta bilirubin are measured photometrically and thus the value is a little higher than conjugated bilirubin alone.8
Results
Sample population and data collection
Forty neonates had no successful investigations at all because they were either no longer deemed jaundiced by the nurses or the blood sample was insufficient for analysis. The remaining 420 had blood sampled for split bilirubin levels (419 with at least one total bilirubin; 418 direct bilirubin). Further investigations were a repeat split bilirubin±further blood tests and liver ultrasound scan. The total number of times split bilirubin samples were taken was 501 (499 total bilirubin; 496 direct bilirubin). 359 children had one measurement, 46 had two, 10 had three and 5 had four. None of the neonates we investigated further (eg, additional bloods and imaging) were found to have liver disease (ie, all liver function tests and ultrasound scans were not indicative of causation).
The population level
Figure 1A shows that, at the population level of disease-free neonates with prolonged jaundice, the total bilirubin decreases noticeably with age at measurement in a similar curve to that described by previous studies1 with means around 150 µmol/L and 95th centiles of up to 250 µmol/L.
Graphically, the direct bilirubin level appeared relatively independent of age. Figure 1B shows that the mean remains close to 15 µmol/L and the 95th centile around 25 µmol/L.
Figure 1C shows that the direct–total bilirubin ratio showed no clear trend and was very variable, especially across the 95th centile, with some values >30%.
Linear regression analysis showed that for each day of older age, total bilirubin fell by 3.72 µmol/L (95% CI 2.46 to 5.00; P value <0.0001) and the direct bilirubin fell by 0.39 µmol/L (0.18 to 0.59; P value 0.0002). This equates to a 2.5%/day reduction from the approximate mean total bilirubin of 150 µmol/L and 2.6%/day from the approximate mean direct bilirubin of 15 µmol/L, respectively. The ratio between the two did not change significantly (95% CI −0.0006 to +0.0034; P value 0.1659).
The individual level
Sixty neonates had two complete split bilirubin samples taken. The first sample was taken at a median of 17 days (range 10–63) and the second at a median of 25 days (range 18–70). The median number of days between samples was 5 days (range 1–24). The median value of the first sample was a total bilirubin of 164 µmol/L (range 12–318), direct bilirubin of 14 µmol/L (1–32) and direct–total bilirubin ratio of 0.087 (0.007–0.500). In these neonates, the mean change between samples in total bilirubin was −10 µmol/L (95% CI −137,+68; P value<0.0001) and in direct bilirubin was −4.5 µmol/L (95% CI −22,+22; P value<0.0001). This equates to an average 1.2%/day reduction from initial total bilirubin and 6.4%/day reduction from initial direct bilirubin. On the other hand, the direct–total bilirubin ratio did not change significantly at −0.002 (95% CI -0.096,+0.179; P value 0.8785).
We note that this group of neonates cannot be considered the same as those who had only one sample taken. In comparison, neonates with more than one split bilirubin sample have, on average, 27% higher total bilirubin (P=0.0002), 6% higher direct bilirubin (P=0.0370) and 30% higher direct–total bilirubin ratio (P=0.0067).
Discussion
We consider our data to be an accurate, novel and clinically significant description of split bilirubin levels in a population of disease-free neonates referred with prolonged jaundice. None of the neonates we did investigate further were found to have significant liver disease. Indeed, no neonates in the study have relevant subsequent abnormal liver function tests recorded on our system—which due to biliary atresia’s aggressive course would almost certainly not go unrecorded. It is unlikely that there was a subsequent diagnosis of biliary atresia of which we were not aware as neonates in our area having surgery for biliary atresia return to our community nursing service for follow-up care. We acknowledge that as we are a London centre it is possible for a neonate to have presented to a nearby service with a liver problem of which we were unaware. However, the incidence of biliary atresia is 1:18 000 in the general population4 or a maximum of 1:1500 in our sample (8% of those in our community midwife service). Therefore, the likelihood of a neonate(s) with biliary atresia being present in our sample and not detected by us is exceptionally low and in any case would exert minimal skew on the trends observed.
Our sample is not representative of the normal population, rather it is a description of the population of neonates with prolonged jaundice—this is the clinically relevant group regarding which clinicians must make decisions. Nonetheless, it is reassuring that our results concord with existing data. Maisels et al, a team from Oakland University, describe the natural history of total bilirubin levels (transcutaneous) in a breastfed population.1 The total bilirubin values in our neonates were higher, as expected in a population referred for visible jaundice, but our data decreased with age along a similar trend.
We also plotted the direct bilirubin level against age, which has not been done previously. At the population level in the age range 11–42 days inclusive (96.6% of sample), graphically the direct bilirubin appeared relatively constant with a mean of 15 µmol/L and a 95th centile value of approximately 25 µmol/L. Linear regression analysis showed that direct bilirubin decreases with age, but nonetheless values of direct bilirubin up to 25 µmol/L are seen in disease-free neonates at 2–6 weeks of age. Clinicians may wish to use figure 1 as a reference tool during their practice.
Our direct bilirubin values are generally higher than those found in previous population studies which have been based on neonates in the first 2 weeks of life. Previous work from Birmingham has shown the 97.5th centile for direct bilirubin measured in routinely collected screening specimens of approximately 27 000 neonates at 6–10 days was 21 µmol/L.9 Davis et al 10 found 96% of approximately 70 000 neonates undergoing clinically indicated split bilirubin measurements had a maximum conjugated bilirubin <17 µmol/L in the first 2 weeks of life. Although the neonates in these studies were less than 14 days of age, this appears to be the only evidence informing current advice regarding investigation of prolonged jaundice.2 7 Combining our data with previous studies suggests that the direct bilirubin tends to rise in the first 2 weeks of life, but thereafter decreases slowly in disease-free neonates.
We also calculated the direct–total bilirubin ratio. Linear regression analysis found no significant change with age. The 95th centile values were particularly variable with some >30% and so the direct–total bilirubin ratio used alone is unlikely to be a reliable marker of pathology.
Sixty neonates had two complete split bilirubin samples, allowing us limited interpretation of trends over time at the individual level. Both total and direct bilirubin levels decreased significantly (P values <0.0001)—direct bilirubin by a mean of 4.5 µmol/L over a median of 5 days—while the direct–total bilirubin ratio showed no significant trend (P value 0.8785). The average drop in direct bilirubin was 6.4 %/day compared with 2.6 %/day at the population level. Therefore, failure for direct bilirubin to decrease in an individual must be taken particularly seriously. There is, however, a bias towards these individuals having higher bilirubin levels than those with only one sample taken. Of interest, this was more marked with direct–total bilirubin ratio (30% greater) than direct bilirubin (6% greater), thus highlighting that practitioners continue to consider a raised ratio more significant (warranting further investigations, including repeat split bilirubin) than a raised direct bilirubin which, as discussed above, may be inappropriate.
Our study does not allow calculation of a definitive threshold for direct bilirubin below which biliary atresia or other significant congenital liver disease can be excluded. However, there are data on the rise in direct bilirubin in neonates less than 2 weeks of age found to have biliary atresia demonstrating levels well above 25 µmol/L. Harpavat et al 11 found that the mean direct bilirubin in 34 neonates with biliary atresia was 25 µmol/L at 24–48 hours and 45 µmol/L at 72–96 hours. Terui et al 12 noted a direct bilirubin level of around 90 µmol/L at 2–3 weeks of age in 19 neonates with biliary atresia. Siu and colleagues13 reported a mean direct bilirubin of 142 µmol/L in 20 neonates aged less than 3 months (median 45 days) with biliary atresia. According to our data (see figure 1B), a threshold of 25 µmol/L would result in investigation of roughly 5% of all neonates with prolonged jaundice and seem to carry little risk of missing a case of biliary atresia.
This threshold may even contain a large safety margin. Many centres will measure direct bilirubin, where a threshold of 25 µmol/L would actually reflect a more conservative conjugated bilirubin of 22–25 µmol/L. Furthermore, there is a published audit of a prolonged jaundice service in the UK.14 The protocol for further investigation was a direct bilirubin >18 µmol/L and >20% of total. Ten of 882 (1.1%) neonates tested positive on this measure; eight of whom were confirmed to have neonatal liver disease. None of the others went on to receive such a diagnosis. Thirty-three other neonates were diagnosed with liver disease outside of the prolonged jaundice service, but within the study area during the audit period, and all also met the criteria—the authors conclude that their criteria are 100% sensitive for liver disease. Our data suggest that 5% of neonates with prolonged jaundice have direct bilirubin levels above 25 µmol/L—approximately 4.5 times greater than the 1.1% satisfying Cartledge’s criteria. Their investigation threshold must, therefore, have been more stringent than that recommended by NICE, but still failed to miss a single case of neonatal liver disease.
Conclusion
In a clinically relevant population of disease-free neonates referred with prolonged jaundice, we found the 95th centile for direct bilirubin decreased slowly with age but was approximately 25 µmol/L. Failure for direct bilirubin to decrease with time at an individual level is particularly concerning. In contrast, the direct–total bilirubin ratio was highly variable and hence an unreliable indicator of pathology. While we acknowledge our data do not include any patients with liver disease, they nonetheless provide support for the NICE recommendation that well neonates with prolonged jaundice do not require investigation for liver disease if the conjugated bilirubin is ≤25 µmol/L.2 This threshold has the merits of simplicity and a high margin of safety; however, compared with other more stringent criteria,14 it may result in more neonates being extensively investigated with negligible gain in sensitivity.
References
Footnotes
Contributors JMH: contributed towards planning, conduct and reporting jointly with VHvS and contributed towards data collection alone. VHvS: contributed towards planning, conduct and reporting jointly with JMH. CS : contributed towards data analysis alone. AG: contributed towards explanation of biochemical analysis (direct vs conjugated bilirubin) alone.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.