Article Text

Abstract
Objectives To investigate the association between the mode of birth and adverse neonatal outcomes of macrosomic (birth weight ≥4000 g) and non-macrosomic (birth weight <4000 g) live-born term singletons in vertex presentation (TSV) born to mothers with diabetes (pre-existing and gestational diabetes mellitus (GDM)).
Design A population-based retrospective cohort study.
Setting New South Wales, Australia.
Patients All live-born TSV born to mothers with diabetes from 2002 to 2012.
Intervention Comparison of neonatal outcomes by mode of birth (prelabour caesarean section (CS) and planned vaginal birth resulted in intrapartum CS, non-instrumental or instrumental vaginal birth).
Main outcome measures Five-minute Apgar score <7, admission to neonatal intensive care unit (NICU) or special care nursery (SCN) and the need for resuscitation.
Results Among the 48 882 TSV born to mothers with diabetes, prelabour CS was associated with a significant increase in the rate of admission to NICU/SCN compared with planned vaginal birth.
For TSV born to mothers with pre-existing diabetes, compared with non-instrumental vaginal birth, instrumental vaginal birth was associated with increased odds of the need for resuscitation in macrosomic (adjusted ORs (AOR) 2.6; 95% CI (1.2 to 7.5)) and non-macrosomic TSV (AOR 3.3; 95% CI (2.2 to 5.0)).
For TSV born to mothers with GDM, intrapartum CS was associated with increased odds of the need for resuscitation compared with non-instrumental vaginal birth in non-macrosomic TSV (AOR 2.3; 95% CI (2.1 to 2.7)). Instrumental vaginal birth was associated with increased likelihood of requiring resuscitation compared with non-instrumental vaginal birth for both macrosomic (AOR 2.3; 95% CI (1.7 to 3.1)) and non-macrosomic (AOR 2.5; 95% CI (2.2 to 2.9)) TSV.
Conclusion Pregnant women with diabetes, particularly those with suspected fetal macrosomia, need to be aware of the increased likelihood of adverse neonatal outcomes following instrumental vaginal birth and intrapartum CS when planning mode of birth.
- diabetes
- intensive care
- outcomes research
- resuscitation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Diabetes during pregnancy is associated with adverse neonatal and long-term baby outcomes.
There is no agreement in the national and international guidelines about the best mode of birth for women with diabetes during pregnancy.
What this study hopes to add?
Diabetic women gave birth to macrosomic term singletons in vertex presentation are likely to give birth by intrapartum caesarean section (CS) and those who gave birth to non-macrosomic by instrumental birth.
Intrapartum CS and instrumental vaginal birth are associated with increased likelihood of adverse neonatal outcomes.
Introduction
Diabetes during pregnancy is associated with increased incidence of adverse baby outcomes.1 Babies born to mothers with diabetes during pregnancy are at higher risk of perinatal mortality and morbidity including preterm birth, congenital abnormality, neonatal hypoglycaemia and macrosomia.2
There is little consistency internationally regarding recommendations on the mode of birth for women with diabetes during pregnancy. Variations are seen in both national and professional society guidelines and recommendations.2 The American College of Obstetricians and Gynecologists guidelines recommend caesarean section (CS) for women with diabetes during pregnancy with an estimated birth weight >4500 g.3 4 The National Institute for Health and Care Excellence (NICE) guideline in the UK recommends induction of labour or elective CS if indicated, between 37+0 and 38+6 weeks of gestation for women with pre-existing diabetes.5 For women with gestational diabetes mellitus (GDM), the NICE guideline recommends elective birth no later than 40+6 weeks of gestation.5 The Australasian Diabetes in Pregnancy Society (ADIPS) guidelines advise that for women with pre-existing diabetes, elective CS should be considered if estimated birth weight exceeds 4250–4500 g.6 For women with uncomplicated GDM, ADIPS guideline does not recommend birth before term unless there is an obstetric indication.7
The rate of CS is high among women with diabetes during pregnancy in Australia.8 The leading reasons for a planned CS (prelabour CS) are for the prevention of stillbirth and the reduction of birth complications associated with macrosomia.2 9 Currently, there are no population-based studies in Australia that have evaluated the neonatal outcomes of babies born to mothers with diabetes according to the mode of birth.
Our study aimed to compare adverse neonatal outcomes for live-born term singletons in vertex presentation (TSV) born to mothers with diabetes during pregnancy (pre-existing diabetes and GDM) by mode of birth-stratified macrosomia (macrosomic and non-macrosomic TSV).
Materials and methods
Data source
A population-based retrospective cohort study was conducted using the New South Wales (NSW) Perinatal Data Collection (PDC).10 The PDC is a population-based surveillance system. It includes all births occurring in NSW public and private hospitals as well as home births. Women giving birth to live births and stillbirths of at least 20 weeks or at least 400 g birth weight are included in the database. Around 32% of the Australian population lives in NSW, and more than 95 000 women give birth in this state annually.11 12
The NSW PDC is based on electronic forms that are completed at birth by the attendants. Information on maternal demographics, maternal health, pregnancy, obstetric complications, labour and perinatal outcomes is included in the form. The forms are submitted to NSW Ministry of Health where the information is validated and compiled into the statewide PDC.10
Study population
There were 48 983 TSV born during the study period of which 101 are stillbirths (18 (0.4%) born to mothers with pre-existing diabetes and 83 (0.2%) born to mothers with GDM). Due to our inability to identify times of stillbirth (antepartum or intrapartum), these stillbirths were excluded from the study. The study includes all live-born TSV (n=48 882) born in NSW to mothers with diabetes during pregnancy between 1 January 2002 and 31 December 2012. Of these, 4501 (9.2%) were born to mothers with pre-existing diabetes and 44 381 (90.8%) were born to mothers with GDM.
Of our study population, 276 (0.4%) TSV were excluded from the multivariate logistic regression due to admission to neonatal intensive care unit (NICU) or special care nursery (SCN) with one or more diagnosed birth defects, and 71 (0.1%) were excluded because of missing data (mode of birth, birth weight and admission to NICU or SCN due to birth defect). A total of 4458 live-born TSV born to mothers with pre-existing diabetes and 44 148 born to mothers with GDM were included in the multivariate logistic regression.
Study factors and outcome measurements
Pre-existing diabetes includes type I and type II. GDM is defined as glucose intolerance that is diagnosed for the first time during pregnancy which may include hyperglycaemia induced by pregnancy or previously undiagnosed existing abnormalities of glucose tolerance.13
Modes of birth include non-instrumental and instrumental vaginal births, prelabour CS (often known as an elective CS) and intrapartum CS. Planned vaginal births are births that were primarily intended to be non-instrumental vaginal births, although they might end with intrapartum CS, instrumental vaginal birth or non-instrumental vaginal birth.
The definition for macrosomia adopted by the International Association of Diabetes in Pregnancy Study Group of birth weight ≥4000 g was used.14 ‘Large for gestational age’ was defined as a birth weight greater than the 90th percentile for gestational age and ‘small for gestational age’ is birth weight less than the 10th percentile.14
Adverse neonatal outcomes were 5 min Apgar score <7, neonate admission to NICU or SCN, and the need for resuscitation which included resuscitation by intermittent positive pressure respiration by bag and mask, intubation, and intermittent positive pressure respiration, external cardiac massage and ventilation.
Statistical analysis
Maternal characteristics and baby outcomes were compared by mode of birth using Χ2 test. Trend analysis was used to compare the rate of prelabour CS by year using Mantel-Haenszel test for trend analysis.
Multivariate logistic regression was used to investigate the likelihood of adverse neonatal outcomes by mode of birth. Two analyses were conducted; the first compared TSV born by prelabour CS with TSV born by all other modes of birth combined as planned vaginal births. This first analysis was performed to inform the decision of performing prelabour CS or proceed to planned vaginal birth. The second compared TSV born by non-instrumental vaginal birth, TSV who were planned as vaginal births but for whom resorting to instrumental birth and intrapartum CS, and TSV born by prelabour CS. The second analysis was performed to help inform the decision in the situation where vaginal birth is planned.
Adjusted OR (AOR) and 95% CI were presented. The adjustment was made for maternal age, maternal country of birth (Australian-born mothers, overseas-born mothers), parity (no previous pregnancies; one, two, three or more previous pregnancies), smoking during pregnancy (smoked, did not smoke), essential and pregnancy-induced hypertension, and hospital sector (public, private). The analysis was performed using Statistical Package for Social Science (SPSS) software V.22.0 (IBM). P value <0.05 or CI not including 1 was considered statistically significant.
Results
Maternal characteristics and baby outcomes are presented in tables 1 and 2. Among mothers who went into labour, 38.8% with pre-existing diabetes and 31.5% with GDM gave birth by instrumental vaginal birth or intrapartum CS. The highest proportion of mothers aged <25 years were among mothers with pre-existing diabetes who gave birth by instrumental vaginal birth (16.9%, P<0.001) (table 1). The proportion of primipara mothers were higher among those who had instrumental vaginal birth (70.5% and 77.3% among mothers with pre-existing diabetes and mothers with GDM, respectively) (tables 1 and 2). There were 17 neonatal deaths of which 2 (0.4 per 1000 live-born TSV) were born to women with pre-existing diabetes and 15 (0.3 per 1000 live-born TSV) were born to women with GDM.
Maternal characteristics and birth outcomes for TSV born to women with pre-existing diabetes, 2002–2012
Maternal characteristics and birth outcomes for TSV born to women with gestational diabetes, 2002–2012
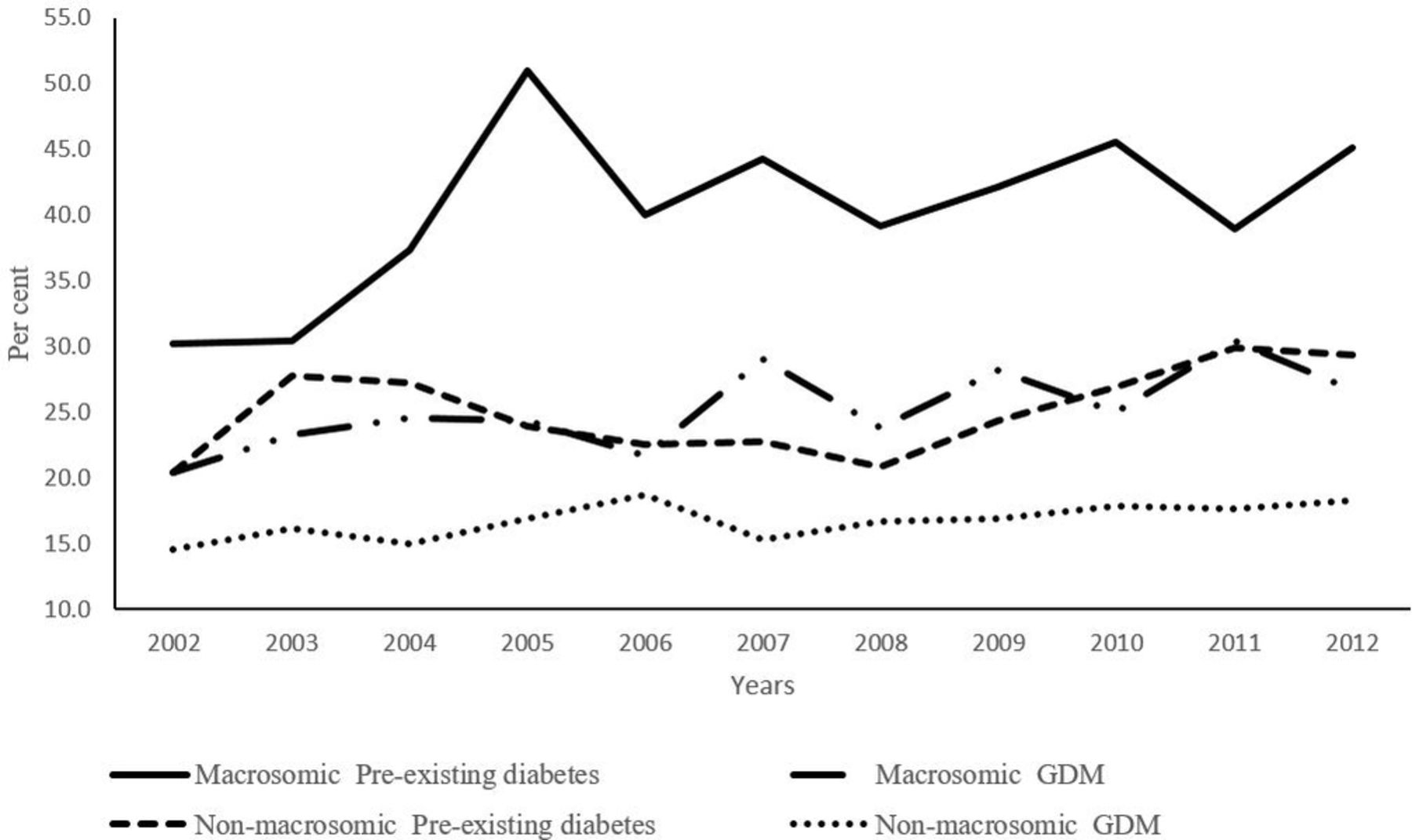
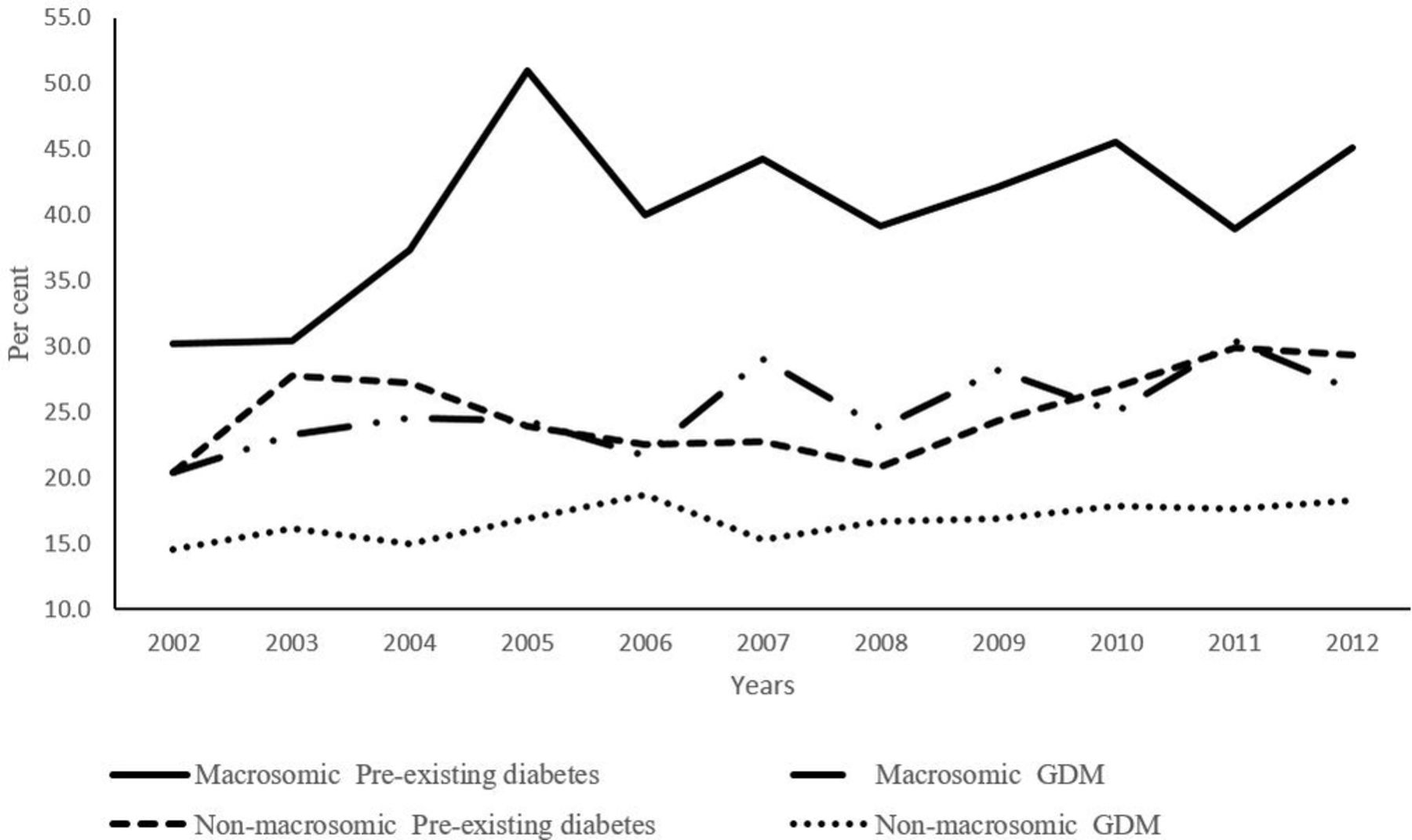
Figure 1 shows an increasing trend in prelabour CS for both macrosomic and non-macrosomic TSV. The largest increase was seen among macrosomic TSV (P=0.048), followed by non-macrosomic TSV born to mothers with pre-existing diabetes (P=0.032).
{kind=link}
Rates of prelabour caesarean section. GDM, gestational diabetes mellitus.
Among mothers with pre-existing diabetes in the planned vaginal birth group, the highest rate of instrumental vaginal birth was among those who gave birth to non-macrosomic TSV who had induction of labour (13.2%) (online supplementary figure 1). Mothers with GDM who had induction of labour and gave birth to non-macrosomic TSV had the highest rate of instrumental vaginal birth (15.2%) (online supplementary figure 2).
Supplementary file 1
Supplementary file 2
There were no significant changes in the rate of admission to NICU/SCN for TSV born to mothers with pre-existing diabetes and for macrosomic TSV born to mothers with GDM from 2002 to 2012. There was a significant increase in the rate of high-level resuscitation for non-macrosomic TSV born to mothers with GDM between 2002 and 2012.
Prelabour CS compared with planned vaginal birth
For TSV born to mothers with pre-existing diabetes by prelabour CS, there was a significant increase in the odds of admission to NICU/SCN compared with TSV born by planned vaginal birth (AOR 2.3, 95% CI (1.7 to 3.2) for macrosomic TSV; AOR 1.6, 95% CI (1.4 to 1.9) for non-macrosomic TSV) (table 3).
Adjusted ORs for adverse neonatal outcomes of TSV born to women with diabetes during pregnancy after prelabour CS and planned vaginal birth, 2002–2012
Non-instrumental vaginal birth compared with other modes of birth
TSV born to mothers with pre-existing diabetes
For non-macrosomic TSV, prelabour CS, instrumental vaginal birth and intrapartum CS were associated with increased odds of admission to NICU/SCN compared with non-instrumental vaginal birth (AOR 2.1, 95% CI (1.8 to 2.5) for prelabour CS; AOR 1.8, 95% CI (1.4 to 2.3) for instrumental vaginal birth; AOR 2.4, 95% CI (2.0 to 3.0) for intrapartum CS). Both instrumental vaginal birth and intrapartum CS were associated with a significant increase in the odds of requiring resuscitation compared with non-instrumental vaginal birth (AOR 3.3, 95% CI (2.2 to 5.0) for instrumental vaginal birth; AOR 2.3, 95% CI (1.6 to 3.4) for intrapartum CS) (table 4).
Adjusted ORs for adverse neonatal outcomes of TSV born to women with diabetes during pregnancy by mode of birth, 2002–2012
For macrosomic TSV, instrumental vaginal birth was associated with a significant increase in the odds of requiring resuscitation (AOR 2.6, 95% CI (1.2 to 5.7)) and admission to NICU/SCN (AOR 2.1, 95% CI (1.1 to 3.9)) compared with non-instrumental vaginal birth (table 4).
TSV born to mothers with GDM
Among non-macrosomic TSV, compared with non-instrumental vaginal birth, all other modes of birth were associated with increased odds of admission to NICU/SCN (AOR 1.5, 95% CI (1.4 to 1.6) for instrumental vaginal birth; AOR 1.9, 95% CI (1.7 to 2.0) for intrapartum CS; AOR 1.6, 95% CI (1.5 to 1.7) for prelabour CS) and need for resuscitation (AOR 2.5, 95% CI (2.2 to 2.9) for instrumental vaginal birth; AOR 2.3, 95% CI (2.1 to 2.7) for intrapartum CS; AOR 1.5, 95% CI (1.3 to 1.7) for prelabour CS) (table 4).
Among macrosomic TSV born to GDM mothers, compared with non-instrumental vaginal birth, the rate of requiring resuscitation was higher after instrumental vaginal birth (AOR 2.3, 95% CI (1.7 to 3.1)) and lower after prelabour CS (AOR 0.7, 95% CI (0.6 to 0.9)) (table 4).
Discussion
To our knowledge, this Australian study is the largest population-based investigation of neonatal outcomes related to mode of birth in live-born TSV born to mothers with diabetes during pregnancy. The study results showed that, among TSV born to mothers with diabetes during pregnancy, prelabour CS was associated with a significant increase in the rate of admission to NICU/SCN compared with planned vaginal birth. Both instrumental vaginal birth and intrapartum CS were associated with increased odds of requiring resuscitation compared with non-instrumental vaginal birth.
The use of a large validated population-based data set with high accuracy15 generates a high level of evidence that cannot be achieved in hospital settings. Our study provides population-level evidence on the association between mode of birth and neonatal outcomes of TSV born to mothers with diabetes during pregnancy in NSW. Our study also provides information about clinical practice for mothers with diabetes during pregnancy. The validation study by Ampt et al on the NSW PDC shows that the PDC had high sensitivity (≥94.7%) and high positive predictive value (≥96.1%) in reporting dichotomised outcome variables such as 5 min Apgar score <7 and neonatal resuscitation.16
The limitation of the study is the lack of information on reasons for NICU/SCN admissions as macrosomic TSV are routinely admitted to NICU/SCN for expected hypoglycaemia without clinical necessity which increases the rate of admission to NICU/SCN. Some services do have a routine policy of admitting babies born to mothers with diabetes to an NICU/SCN, hence the numbers could be higher. Another limitation is the lack of information on maternal body mass index and on umbilical artery pH and lactate levels. To remove the confounding related to birth defects, we excluded TSV admitted to NICU/SCN because of birth defects from our multivariable logistic regression. However, we are unable to adjust for maternal body mass index, an independent risk factor for adverse pregnancy outcomes such as low Apgar score and a higher rate of admission to NICU.17 We used stratification by estimated fetal macrosomia using birth weight to limit the impact of maternal body mass index on the mode of birth and neonatal outcomes. We are also unable to adjust for shoulder dystocia as it was not captured in NSW PDC. We also lack information on second-stage CS which did not allow us to compare between intrapartum CS and instrumental vaginal birth.
There was no significant difference in the odds of 5 min Apgar score <7 between TSV born after prelabour CS and those born after planned vaginal birth for mothers who had pre-existing diabetes or GDM. Stuart et al found a significant reduction in the odds of 5 min Apgar score <7 among TSV born to mothers with diabetes during pregnancy who were born after prelabour CS at 38 weeks’ gestation compared with those born after planned vaginal birth at 39 weeks’ gestation.18
TSV born to mothers with diabetes during pregnancy can be affected by a number of morbidities including respiratory distress syndrome, hypoglycaemia and hypocalcaemia that can lead to an increase in the likelihood of admission to NICU/SCN.5 In addition, CS is associated with increased odds of neonatal respiratory morbidity.19 The NICE guideline recommended admission to NICU if babies who were born to mothers with diabetes had one of the following symptoms: hypoglycaemia, respiratory distress or jaundice, signs of cardiac decompensation, neonatal encephalopathy or polycythaemia, the need for tube feeding or who were born preterm.5
Our study found that instrumental vaginal birth and intrapartum CS were associated with an increase in the odds of the need for resuscitation and admission to NICU/SCN compared with non-instrumental vaginal birth. One indication for instrumental vaginal birth and intrapartum CS is fetal compromise,20 which is also an indication for neonatal resuscitation.21 Thus, requiring resuscitation might have been associated with fetal compromise, not the use of instrumental vaginal birth or intrapartum CS. However, instrumental vaginal birth alone is also considered a risk factor for requiring neonatal resuscitation.21
Our study found that women with diabetes have a low rate of non-instrumental vaginal birth and high rate of giving birth by intrapartum CS and instrumental birth. This is consistent with previous studies.18 22 Among our population of mothers who went into labour, 38.8% of those with pre-existing diabetes and 31.5% of those with GDM gave birth by instrumental vaginal birth or intrapartum CS compared with 29.4% of women in the NSW general population.23 One in four mothers (25.9%) with planned vaginal birth gave birth to a macrosomic TSV by intrapartum CS, and one in five mothers (20.5%) with planned vaginal birth gave birth to a non-macrosomic TSV by instrumental vaginal birth. Given that both intrapartum CS and instrumental birth are associated with increased odds of adverse neonatal outcomes, the high proportion of resorting to instrumental vaginal birth for non-macrosomic TSV or intrapartum CS for macrosomic TSV should be considered when planning vaginal births.
Although prelabour CS was associated with a reduction in some adverse neonatal outcomes, specifically requiring resuscitation for macrosomic TSV, prelabour CS is associated with adverse maternal outcomes. In the general population, CS is associated with immediate risk to the mother of infection, haemorrhage, anaesthetic risks and mortality.24 It is also associated with an increased likelihood of repeat elective CS in future pregnancies and increased risk of stillbirth and placenta praevia and accreta, uterine rupture, and peripartum hysterectomy.24 The risk of adverse maternal outcomes following CS might be escalated for women with diabetes during pregnancy since they are at higher risk of adverse maternal outcomes (such as infection and impaired wound healing) than women without diabetes.25
Conclusion
Of mothers with planned vaginal birth, one in four gave birth to a macrosomic TSV by intrapartum CS and one in five gave birth to a non-macrosomic TSV by instrumental vaginal birth. The potential risk of adverse neonatal outcomes associated with intrapartum CS and instrumental vaginal birth should be considered when planning for birth of women with diabetes. Close monitoring and readiness to intervene are needed when planning labour for TSV, particularly when the baby is macrosomic as CS is often required to expedite birth.
Acknowledgments
This research is supported by an Australian GovernmentResearch Training Program Scholarship. This study is based on NSW Perinatal Data Collection made available by theCentre for Epidemiology and Evidence, NSW Ministry of Health. We would like to thank the NSW Ministry of Health forproviding the data.
References
Footnotes
Contributors All authors were involved in the conception and design of the work and interpretation of the data for the manuscript. RZ was involved in initial drafting of the work. RZ, ZL and AYW were involved in analysing the data. ALL authors were involved in the critical revision of the manuscript for intellectual content and approved the paper as submitted. All authors agree to be accountable for all aspects of the work and in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding None declared.
Competing interests None declared.
Ethics approval University of Technology Sydney Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.