Article Text

Abstract
Introduction Conducting research with children in low/middle-income countries (LMIC) requires consideration of socioeconomic inequalities and cultural and linguistic differences. Our objective was to survey the literature on informed consent in paediatric LMIC research, assessing for practical guidance for culturally and linguistically appropriate procedures.
Methods We conducted a scoping review on informed consent in paediatric LMIC research searching the PubMed, Web of Science and PsycINFO databases. Eligible articles were published in English, from any date range, of any study design or format.
Results The search identified 2027 references, of which 50 were included in the analysis following full-text review. Reviewed guidelines emphasised individual, informed and voluntary consent from parents and caregivers. Reviewed articles provided detailed practical guidance on adapting these guiding principles to LMIC settings, including considerations for community engagement, verbal or other alternative consent procedures for low-literacy settings or less commonly spoken languages and guarding against therapeutic misconception by caregivers. There was uncertainty, however, on how to best protect individual autonomy, especially when influenced by gender dynamics, leadership hierarchies or the social status of researchers themselves. There was, furthermore, limited research discussing the special case of research involving adolescents or of procedures for documenting assent by participating children.
Conclusions A scoping review of paediatric research in LMICs revealed substantial guidance on several features of culturally appropriate informed consent. However, additional research and guidance is needed, especially in the areas of gender imbalances, research with adolescents and children’s own assent to participate in research.
- ethics
- health services research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Conducting research with children in low/middle-income countries (LMIC) requires careful consideration of socioeconomic inequalities and cultural and linguistic differences.
International standards for the conduct of paediatric research include informed consent, voluntariness and assent, but there is limited guidance on operationalising these concepts in LMICs.
What this study hopes to add?
Highlighting consensus for best practices in community engagement, verbal and alternative consent procedures and guarding against therapeutic misconception in interventional and randomised controlled trial designs.
Demonstrating where additional research i, especially around the protection of the individual autonomy of caregivers and safeguarding children’s own assent to participate in research.
Introduction
Prior to World War II, there was little international consensus on the ethical conduct of human subjects research. The Nuremberg code, developed in 1947 during the Nuremberg war crime trials, was one of the first attempts to articulate basic ethical principles, such as the right to informed consent.1 Subsequently, the World Medical Association’s Declaration of Helsinki in 1964 provided a more definitive consensus statement on the core principles of ethical conduct of research—beneficence, self-determination and informed consent—which is widely considered the foundational international document in modern research ethics.2 Practical guidance on ethical practice is well codified in the joint statements produced by the Council for International Organizations of Medical Sciences (CIOMS) and the WHO.3
Extension of ethical research principles to include considerations appropriate for research in paediatric populations is also important, including guidance on obtaining informed consent from parents or guardians, obtaining assent from children themselves and weighing the balance of risks and benefits of proposed research.3 4 Improvements in the conduct and volume of paediatric clinical trials, which have historically been few in number and of lower quality than corresponding trials in adult subjects, have also recently been advocated.5
However, there still remains uncertainty around how best to implement international ethical principles of paediatric research in some settings. This is especially the case in low/middle-income countries (LMIC), and in research with groups such as indigenous populations, speakers of less common languages or populations with high levels of illiteracy. Practically, we experienced this recently while designing a clinical trial of a nutrition intervention for indigenous Maya children in rural Guatemala, and our experience navigating consent, literacy and translingual adaptation in this population prompted our interest in more formally exploring the topic.6 To this end, here we conduct a scoping review of the existing literature on cultural and contextual considerations for informed consent in the conduct of paediatric research in LMICs. Through this review, we identify evidence for specific culturally and contextually sensitive practices, as well as areas where additional research and guideline development is needed.
Methods
Search and inclusion strategy
To identify articles, we searched the PubMed, Web of Science and PsycINFO databases. We conducted searches using a combination of the following key terms: ‘pediatric’ or ‘children’ or ‘adolescents’; ‘research’ or ‘biomedical research’; ‘consent’ or ‘informed consent’ or ‘ethics’; ‘developing countries’ or ‘low income countries’ or ‘middle income countries’; ‘illiteracy’; ‘culturally competent’. We used no date limits and included all articles published through May 2018. In addition, we visited the websites of international health policy organisations to identify ethics guidelines for the conduct of research in LMICs. We also manually reviewed the reference lists of articles identified using the above methods. For this scoping review we included for analysis any type of study design or format (original research, commentary, case study, review, expert opinion), which addressed the informed consent process specifically for paediatric or adolescent populations in LMICs. Articles not in English were excluded.
Data extraction and synthesis
We exported identified articles into an Excel spreadsheet template which recorded location of study, study type and design, study context, aspects of informed consent examined and key findings. Both authors reviewed the study titles and abstracts. After removal of articles which were deemed not eligible for inclusion, one author (MC) performed a full-text review of all the remaining articles. As a scoping review to assess the patterns of existing literature on informed consent in LMIC paediatric research, assessments of individual study bias and quality were not performed. Data extracted from articles were collated in summary form (table 1–8), and major qualitative findings are presented in the following narrative synthesis.
Summary of selected major guidelines on ethical conduct of research in children
Results
Results of literature screen
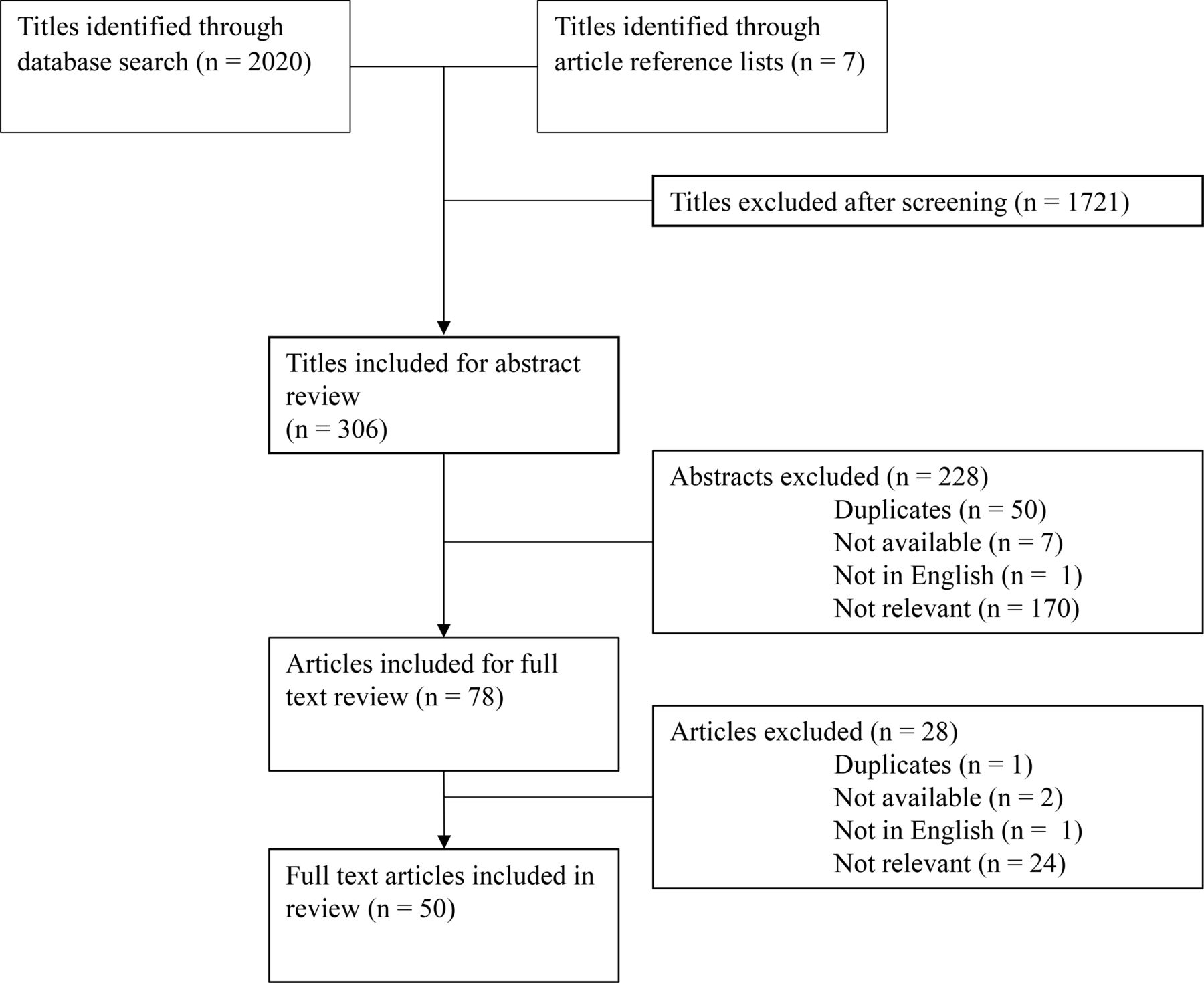
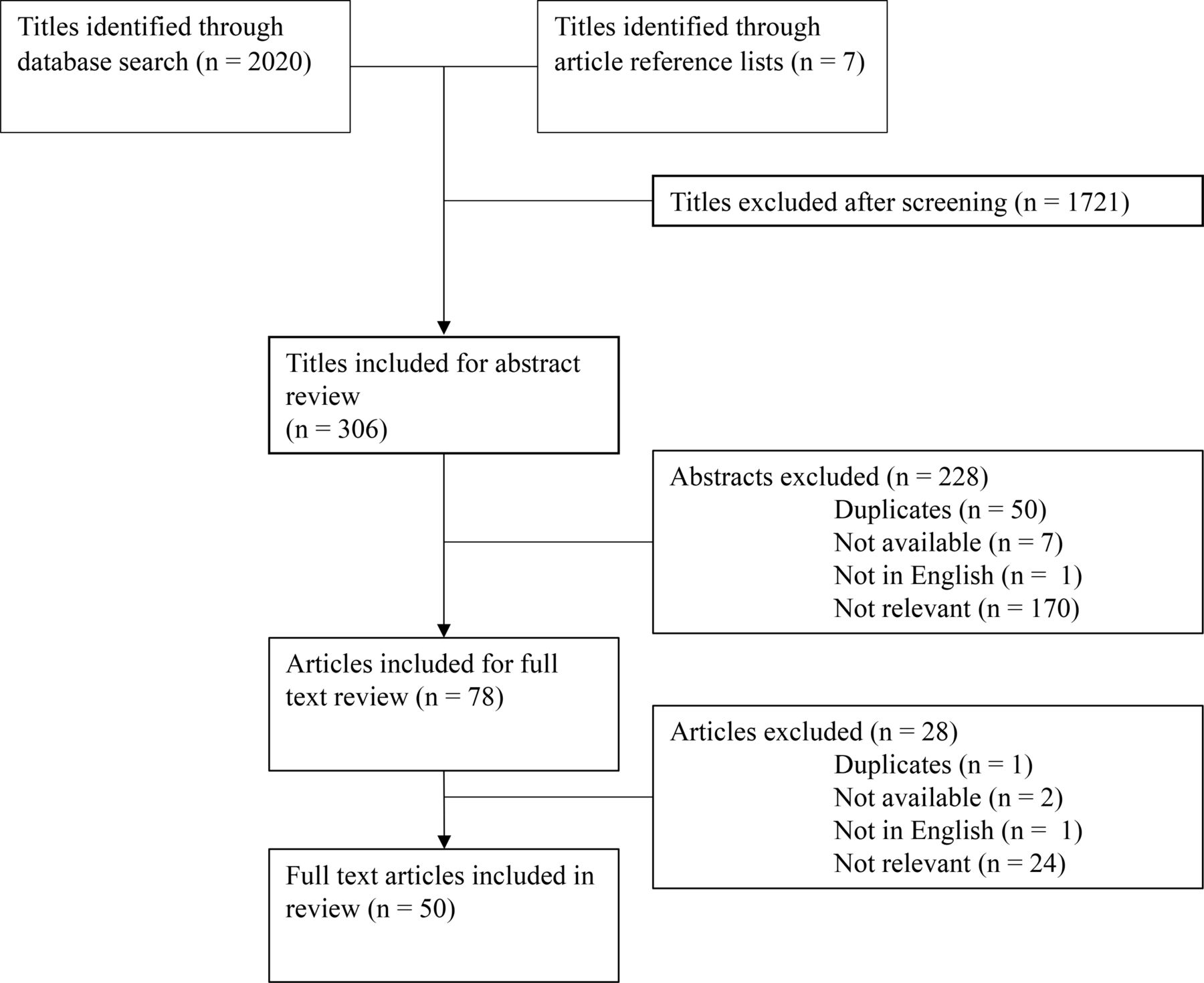
A total of 2027 candidate titles were identified through database searches, supplemented by reference list and website reviews. Of these, 1721 did not meet eligibility criteria, and 306 were included for abstract review. If the abstract was not available but full text was, the title was included for full-text review. After abstract review, 50 duplicates were found, 1 was not in English, 7 were not available (abstract nor full text) and 170 abstracts did not meet inclusion criteria. Seventy-eight articles were selected for full-text review, of which 24 subsequently did not meet inclusion criteria, 1 was in French, 1 was a duplicate and 2 did not have available full text. Therefore, 50 full-text articles were included in this review (figure 1, table 1–8). Of the articles excluded at the abstract and full-text review stages, the most common reasons for exclusion were: no mention of the informed consent process for research with paediatric or adolescent populations; research not taking place in an LMIC; and articles on paediatric research in LMICs that did not discuss the informed consent process.
{kind=link}
Results of literature screen. Flow diagram depicting results of the literature search and review procedure.
Summary of guidelines and commentaries
We identified seven guidelines that addressed issues of informed consent in international settings and in research involving children in our scoping review. Of these, we selected for detailed review five that were most comprehensive, summarising key recommendations in table 1. All guidelines emphasise the importance of obtaining individual, informed and voluntary consent for research.3 4 7–9 Importantly, however, the guidelines do not necessarily specify in detail how best to operationalise these core principles. For example, the Declaration of Helsinki comments only that informed consent requires that a subject be adequately informed of the ‘aims, methods, sources of funding, any possible conflicts of interest, institutional affiliations of the researcher, the anticipated benefits and potential risks of the study and the discomfort it may entail, post-study provisions and any other relevant aspects of the study’ (Article 26).7 Similarly, on voluntariness, the CIOMS guidelines note only that consent is voluntary if ‘an individual’s decision to participate is free of undue influence’ (p 35).3
Some of the guidelines do suggest modifications appropriate for lower resource settings, such as obtaining witnessed verbal consent when literacy is a barrier.7 9 The US National Bioethics Advisory Commission also acknowledges that oral consent might even be preferable in some circumstances.8 However, as other commentaries note, there is little specificity on how best to operationalise these suggestions, such as how to formally document verbal consent or characteristics of a qualified witness.10 11
Another important consideration of LMIC research addressed in guidelines is an emphasis on the need to at times obtain consent from community stakeholders and leaders, or other key local decision makers. Nevertheless, all guidelines unanimously assert that community-based consent can never replace individual consent. When local cultural practices around community-based consent contradict core principles of the international consensus on the informed consent process, such as the need for voluntary individual consent, researchers are advised to search for culturally sensitive ways of providing all information to potential participants without compromising the substantive ethical standard of informed consent, an adaptive process in which local research ethics committees are expected to place a substantial role.8 10–12
Finally, with respect to children or adolescents not capable of providing informed consent, in addition to obtaining consent from parents or legal representatives, most guidelines also reinforce the need to obtain assent from the child or adolescent in an age-appropriate way.3 4 7 9 The CIOMS guidelines note that assent is ‘a process…not merely the absence of dissent’ and requires ‘meaningful engage[ment] in the research discussion in accordance with…capacities’ (p 67).3 They also note that as adolescents reach the age of maturity, their agreement to participate may be ethically considered as informed consent. However, if they legally remain minors, researchers are cautioned that consent from a parent is still generally needed, but a list is provided of possible situations when parental consent might be waived, such as with legally emancipated adolescents, or under circumstances where obtaining parental consent is not desirable because of the research topic.3
Thematic summary of research on consent in LMIC paediatric research
Existing published work on informed consent in paediatric research in LMICs includes a number of review and opinion articles (table 2) as well as case studies describing the experience of individual research teams and discussing the challenges and solutions used when adapting consent processes to their local context. We summarise several major themes emerging from these studies here in narrative form and provide detailed key findings from the reviewed articles in the accompanying tables.
Summary of review and opinion articles on ethical conduct of research in children
Understanding social norms around decision-making and protecting individual autonomy
An important principle highlighted in international guidelines on informed consent in LMICs is appropriate and early engagement with existing local leadership structures (such as a council of elders) balanced against respect for the autonomy of individual children or their caregivers.3 8 In practice, this can be a delicate balance to maintain (table 3). Kongsholm and colleagues, for example, describe consent processes in rural Pakistan, where family structures are patriarchal and hierarchical. In this setting, consent procedures involved first seeking consent from an elder, who provided initial consent for the entire family. However, under this approach, the voluntariness of individual participants may be undermined, and it is unclear how best to ensure that individuals still retain an ‘opt out’ mechanism or, conversely, the right to participate in research if they wish to do so but the elder declines.13
Summary of articles discussing social norms, decision-making and autonomy*
Another important consideration explored by some studies is understanding how not all potential consenting caregivers may feel empowered to decline participating in research. Consent procedures administered by local research personnel or by individuals with high social status, such as physicians, may inspire trust.13 14 However, it may also make them reluctant to decline participation, or to resist active participation. For example, in one study in Kenya, explicit refusals to participate were often considered to be impolite. Here researchers found that caregivers expressed their unwillingness to participate by delaying the consent process, or by participating inconsistently in research procedures even after initially having consented to the study.15
Adapting consent procedures to low-literate settings
There is strong consensus in international ethics guidelines that written, informed consent is preferred when conducting research (table 4). In the case of paediatric research, this typically involves obtaining written consent from one or both primary caregivers.4 9 16 However, in many LMIC settings, literacy may be low or a high value may be placed on oral interactions, and lack of alternative consent procedures may violate another core ethics principle, namely the equitable distribution of research benefits and burdens across populations.3 14 17 Some of the studies we reviewed described these procedures, with verbal consent commonly being obtained, most often in the presence of a literate witness who is able to read available consent documents.13 14 17 18 In one very thoughtful piece, Kalabuanga and colleagues note, however, that witnesses may often impose their views on the consenting caregiver and their child, rather than encouraging dialogue and acting as a safeguard, especially since they are often recruited in an ad hoc fashion (eg, other literate patients or ancillary hospital staff).18 Kalabuanga et al go on to suggest that these challenges may be mitigated by careful vetting and training of independent witnesses or, alternatively, by allowing potential consenting caregivers to use a trusted relative or friend as their witness.18
Summary of articles discussing working in low-literate settings, and with indigenous or less commonly spoken languages
Another issue identified in the review is that of emerging mandates in some LMICs to document consent procedures. For example, in India, audiovisual documentation of obtaining informed consent is now required for most clinical trials if participants are low literate. This introduced significant new logistical challenges and costs related to obtaining and archiving recordings, and it may also pose a barrier to potential research subjects who may distrust or refuse to be recorded.19
Working in indigenous or less commonly spoken languages
International ethics guidelines emphasise that research information should be provided to consenting caregivers in a local language understandable to the individual (table 4).7 8 16 However, this is most commonly understood to be a working lingua franca, and the issue of provisioning consent processes in an indigenous language is largely unaddressed in LMICs.20 This is an important consideration, given that a substantial proportion of the potential paediatric research population in LMICs are from populations that speak indigenous or less commonly spoken languages.21 In an interesting review of lessons learnt in a paediatric vaccine trial in West Africa, Martellet and colleagues noted challenges in preparing consent procedures in some of the less common language groups included in the trial, where use of the written form was uncommon, where substantial need to rely on metaphor and paraphrase made back-translation difficult and where written documents were perceived as not being dynamic enough in cultures which valued interactivity and person-to-person exchange. They describe alternative procedures, such as the preparation of recordings of consent scripts in local languages and extensive practice sessions with research staff obtaining consent in local languages.17 Similarly, another vaccine trial in The Gambia described the successful use of Speaking Book audiovisual tools in local less common languages to consent caregivers.22
Gender dynamics in caregiver consent
Local gender dynamics and decision-making procedures when consenting male and female caregivers for research are an important consideration (table 5). For example, when consenting with caregiving couples or within an extended family unit, instances are discussed where a female caregiver wishes to allow her child to participate, but is unable to do so because her husband or another male authority figure refuses.13 The opposite may also occur, if a research study is consented by a male figure, but requires significant participatory effort from the primary female for study-related activities, leading the woman to express their refusal through procedural delay or inconsistent participation.15 Given concerns about gender power imbalance and potential repercussions for consenting female caregivers, some studies discussed working to routinely involve fathers or male authority figures in the consent process for more complex or higher risk research interventions.15 23 In one interesting study based in India, Rajaraman and colleagues found that caregivers were more likely to actively participate in the consent process when both were present. They also observed, however, that this factor may have been due to the fact that most study staff obtaining consent were male, and they call for more research on how the gender of research staff impacts the consent process.24
Summary of articles discussing gender
It is important to note that most discussions of gender dynamics that we reviewed were limited in nuance, tending to focus on instances of overt over-riding of female decision-making by male authorities. A broader consideration of the range of ways in which female caregivers communicate, influence and negotiate decision-making with male family members and other community authorities is an obvious point for future investigation.
Disclosing potential benefits and risks of participation in research
Participation in some research studies, particularly those with a randomised controlled design or those with differing intervention arms, may not result in direct benefit to all participants. Several studies report difficulties explaining to caregivers that medical research procedures may not result in direct benefit to their children, and in verifying that caregivers comprehended randomisation or control procedures (table 6).25–28 Others noted the need to address issues of information recall and retention, particularly with complex study procedures or consent forms, and to emphasise the right of study withdrawal and the ongoing reaffirmation of consent throughout a study.26–29 Furthermore, other reports discussed how therapeutic misconception—the perception by research subjects that participation in any component of a multiple-arm, controlled trial will result in therapeutic benefits—might be hard to avoid in certain contexts, as it might be affected by factors like educational level and cultural and religious beliefs about disease.13 18
Summary of articles discussing communicating about risks and benefits of research
At the same time, care must be given to a culturally appropriate degree of information disclosure. For example, in several studies, caregivers—especially those of higher socioeconomic or educational status—were more likely to participate when provided with detailed and in-depth information about the study processes and given opportunities to ask questions.12 23 24 30 At the same time, other case studies point out how overdetailed discussion of study procedures or scientific rationale may provoke unneeded reserve or suspicion where such detailed disclosures by health professionals are not culturally customary.13
Finally, in settings where access to healthcare and other important social goods may be limited, even basic diagnostic or ancillary procedures that occur as part of research studies may be better than the local standard of care, leading to an undue inducement or highly compelling incentives for caregivers to enrol their children in research, even after being informed about the experimental nature of studies and the risk-benefit balance.11 13 18 These considerations highlight the importance of considering the socioeconomic and cultural background of study settings well before beginning research and making plans to incorporate appropriate early, equitable benefit-sharing measures when possible, such as using study resources to improve community-level care, not just care for eligible trial participants.18
Adolescents
Adolescents constitute a special population with vulnerabilities different from those of adults and younger children, and they should be included in research that addresses their specific needs (table 7). However, as legal minors they often cannot give informed consent for research.16 In research in LMICs, regulations vary significantly from country to country regarding when adolescents can provide legal consent for research.31 For example, even when legal frameworks allow adolescents to seek contraception services without parental permission, they cannot necessarily provide consent for research on that theme.32 33 In a scoping review of postabortion care research, Zulu and coauthors discuss how the need to balance adolescents’ privacy needs and the demand for parental consent poses difficulties for researchers in this field.34 Woollett and colleagues describe an interesting case study where they sought consent from a High Court in South Africa for research involving orphaned HIV-positive adolescents. In that study, they provide detailed recommendations for consent involving adolescents, including training staff about confidentiality requirements; recognising immature decision-making by adolescents and developing appropriate methods for probing comprehension and consent; and using methods that promote active participation in research, such as mobile phones.33
Summary of articles discussing research with adolescents
Assent
Paediatric research guidelines are unanimous on the need to obtain age-appropriate assent from children and adolescents who do not provide their own informed consent (table 1). However, we found little explicit discussion or description of procedures for obtaining assent in the research reports we reviewed (table 8).35 36 One interesting qualitative study on parental perceptions of assent in Jordan revealed considerable variability in caregivers’ perspectives about at what age assent should be solicited or if assent should even be obtained and dissent respected in all cases.23
Summary of articles discussing assent
Discussion
Children in low-resource settings are highly vulnerable to exploitation in research, because of circumstances including socioeconomic inequalities, limited access to healthcare and high burden of illness.37 In addition, even where international consensus exists around core ethical principles for providing protections to children as research subjects, it may be unclear how best to operationalise those principles in many low-resource settings, where gender norms, literacy, unfamiliarity with scientific research and language barriers may all be important adaptive barriers.10 11
Through a scoping review of research reports and case studies from LMICs, we identified, however, several core areas where existing research reports provided considerable insight and operational guidance which could be used to guide informed consent design processes in additional LMIC settings. These included: (1) careful consideration of community hierarchy, where consent for research may first proceed through a council of elders or other authority figure, prior to approaching individual caregivers; (2) guidance on developing verbal consent procedures in settings where caregivers have low literacy levels; (3) recognition of the challenges of consent in indigenous or less commonly spoken languages, particularly when that language is not commonly written and where alternative procedures, such as audio recordings in the language, must be employed; and (4) careful consideration of the possibility of therapeutic misconception and of developing consent procedures that ensure caregivers’ comprehension of the potential benefits (or lack thereof) and risks of research procedures for their children.
However, within these four broad thematic areas, we also noted the need for additional careful investigation. In particular, there is considerable uncertainty on how to ensure the principle of subsequent individual informed consent when community leaders or other authorities are approached first. This is especially the case when gender power imbalance is at play, and female caregivers may be either unempowered to consent or to opt out of a research decision made by a male authority. In addition, the social status of individuals administering or witnessing consent procedures may unduly influence the decision-making of caregivers, and research is needed to better understand and accommodate for the interpersonal dynamics of obtaining consent.
Finally, two thematic topics seem to be particularly under-represented in the literature on paediatric LMIC research, and more work is urgently needed. First, despite extensive discussions about the difficulties of conducting research with adolescents, we found only few studies with practical discussions or guidance on how to navigate these difficulties. More investigation of the ethical conduct of research with adolescents is needed, with a broader representation of health conditions, research designs and geographic regions. Second, despite strong representation of the principle of assent in international guidelines on research with children and adolescents, we found little research on cultural and regional differences around notions of assent and virtually no discussion of the mechanics of assessing assent in research studies. Additional research into the topic of assent for research among children in LMICs should be an important priority.
Our review has two important limitations that must be considered. First, we included only articles published in English in major indexing databases. We believe this approach is justified, given our desire to provide a high-level overview of the topic without focusing specifically on any geographic region. Nevertheless, our review has undoubtedly missed resources in other languages or within the grey literature, which could be taken up in more detailed region-specific work on this topic. Second, given the diversity and heterogeneity of the literature reviewed, it was not possible to detail many of the practical insights and tips given in the individual articles. Nevertheless, given the annotation and thematic organisation provided in the tables, we are confident that readers will be able to identify areas of particular interest for more in-depth examination.
Acknowledgments
We thank the research subjects and clinical staff at Maya Health Alliance for inspiring our interest in this important topic.
References
Footnotes
Contributors MC designed the search strategy, extracted data from articles and wrote the first draft of the manuscript. PR conceived the study, reviewed abstracts and revised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.