Article Text

Abstract
Setting Basic epidemiological information on childhood cancer in Western Kenya is lacking. This deficit obstructs efforts to improve the care and survival rates of children in this part of the world.
Objective Our study provides an overview of childhood cancer patients presenting for treatment in Western Kenya.
Design A retrospective analysis of childhood cancer patients presenting for treatment in Western Kenya was carried out using information from three separate databases at the Moi Teaching and Referral Hospital in Eldoret. All patients aged 0–19 years first presenting between January 2006 and January 2010 with a newly diagnosed malignancy were included.
Results A total of 436 children with cancer were registered during the period. There were 256 (59%) boys and 180 (41%) girls with a male/female ratio of 1.4:1. The group aged 6–10 years contained most children (29%). Median age at admission was 8 years. Non-Hodgkin's lymphoma was the most common type of cancer (34%), followed by acute lymphoblastic leukaemia (15%), Hodgkin's lymphoma (8%), nephroblastoma (8%), rhabdomyosarcoma (7%), retinoblastoma (5%) and Kaposi's sarcoma (5%). Only four (1%) children with brain tumours were documented. Ewing's sarcoma was not diagnosed.
Conclusions Our study provides an overview of childhood cancer patients presenting for treatment in Western Kenya. The distribution of malignancies is similar to findings from other equatorial African countries but differs markedly from studies in high-income countries. The new comprehensive cancer registration system will be continued and extended to serve as the basis for an evidence-based oncology program. Eventually this may lead to improved clinical outcomes.
Statistics from Altmetric.com
Introduction
In Western Kenya, the lack of basic epidemiological information on childhood cancer hampers understanding of the spectrum of childhood malignancies and the problems faced. This important pitfall must be redressed so that the care and survival rates of children in this part of the world can be improved.
At least 70% of childhood cancers are currently curable and about 80% of children with adequate cancer treatment are expected to survive. However, only 20% of children affected worldwide benefit from the best available therapy. The vast majority of childhood cancer patients live in low-income countries like Kenya and have only limited or no access to effective therapy and thus little or no chance of survival.1,–,7
What is already known on this topic
▶ Basic epidemiological information on childhood cancer in Western Kenya is lacking.
▶ This deficit obstructs efforts to improve the care and survival rates of children in this part of the world.
What this study adds
▶ An overview of childhood cancer patients presenting for treatment in Western Kenya is presented.
▶ The distribution of malignancies is similar to those in other equatorial African countries but differs markedly from those in high-income countries.
▶ The new comprehensive cancer registration should be used as the basis for an evidence-based oncology program.
This study aims to provide an overview of childhood cancer patients presenting for treatment to Moi Teaching and Referral Hospital (MTRH), the only hospital in Western Kenya treating children with cancer. MTRH did not have a comprehensive hospital-based registry of childhood cancer patients.
Methods
Setting
Kenya is a low-income country and 50% of its population live below the poverty line. In 2009 Kenya had 39 million inhabitants, 42% (16 million) of whom were children under 15 years of age. The male/female sex ratio was 1.01:1.00.8 Kenya has only two academic hospitals able to provide oncology patients with treatment. The first is situated in the capital city Nairobi, while the second, MTRH, is in Eldoret.
The study was carried out at MTRH, the only hospital in Western Kenya treating children with cancer. MTRH serves an estimated population of 16–18 million people, 40–45% of all Kenyan inhabitants, including approximately 7 million children under 15 years of age. With a childhood cancer incidence in low-income countries of 102 per million children under 15 years of age,9,–,11 we would expect around 700 childhood cancer patients under 15 years of age in the area served by MTRH.
MTRH has a total of 550 inpatient beds. The paediatric department has 72 of these beds, 12 of which are reserved for oncology patients, who are cared for by one or two paediatricians. The pathology services employ four pathologists who only use morphology (fine needle aspirate or tissue biopsy) for diagnosis. Children are hospitalised during diagnosis. Children under 15 years of age are treated by a paediatrician in the paediatric ward, while children between 15 and 19 years of age are consulted by a paediatrician in an adult ward. Treatment options include surgery and chemotherapy, but radiotherapy is not available. Treatment protocols developed in the academic hospital in Nairobi are used. Starting in 2007, an outpatient clinic is held once a week with clinicians and nurses in attendance for patients who return home the same day. Paediatric and adult patients are seen together.
Study design
All patients aged 0–19 years with a newly diagnosed malignancy were included in the retrospective study. First presentation of patients occurred between January 2006 and January 2010.
No comprehensive hospital-based registry of childhood cancer patients was available at MTRH: although basic patient information had been collected in three separate databases, the databases had not been merged together. Patients were enrolled if their name was mentioned in at least one of the three databases: (1) the paediatric database, which was started by paediatricians in 2006 and consists of handwritten and electronic reports of hospitalised childhood cancer patients up to 19 years of age; (2) the computerised pathology database, into which pathologists have entered the results of biopsies, fine needle aspirates, bone marrow aspirates and cerebrospinal fluid samples since 2004; and (3) the outpatient oncology database, which contains information on paediatric oncology patients attending day clinics since 2007. A new comprehensive cancer registration database was established by merging these three data sets together.
We collected the following variables: name and registration number of the childhood cancer patient, type of cancer, gender, age at admission and year of first admission. We determined which children were recorded in more than one database by matching names and registration numbers.
Malignancies were diagnosed by clinical observation and by histological examination which was often carried out on tumour material obtained by fine needle aspiration with May-Grünwald Giemsa (MGG) staining. Pathologists sent written diagnostic reports to the paediatrician, who inserted them in the medical records.
Malignancies were classified into six groups: (1) haematological tumours (acute lymphoblastic leukaemia, acute myeloid leukaemia, chronic myeloid leukaemia, non-Hodgkin's lymphoma, Hodgkin's lymphoma, anaplastic large cell lymphoma); (2) brain tumours (medulloblastoma, ependymoma, astrocytoma, glioma); (3) solid tumours (neuroblastoma, nephroblastoma, rhabdomyosarcoma, Ewing's sarcoma, osteosarcoma, retinoblastoma, Kaposi's sarcoma); (4) rare tumours; (5) a group of ‘unspecified’ malignancies which included patients for whom only the primary site of the malignancy was known; and (6) an ‘unconfirmed’ group which consisted of patients mentioned in one of the three databases but for whom we could not confirm the diagnosis.
Data analysis
Data management was performed with Microsoft Excel 2000. Descriptive statistics were used.
Results
By using the three different databases, we gathered information on 436 childhood cancer patients who first presented at MTRH between January 2006 and January 2010 and met the study's inclusion criteria. The paediatric database provided information on 354 (81%) patients, the pathology database on 157 (36%) patients and the outpatient oncology database on 78 (18%) children. Figure 1 shows that 40 (9%) children were registered in all three databases, 73 (17%) in two databases and 323 (74%) in one database.

Intersection of the three databases: the paediatric database, the pathology database and the outpatient oncology database (n=436).
The completeness of the separate databases differed. A total of 436 children initially attended the inpatient clinic and had their diagnosis confirmed by pathologists. However, the paediatric database missed 82 (19%) children, who were either never registered or whose medical records were lost. The electronic pathology database missed 279 (64%) children who were never registered although the pathologists sent written reports on them to the paediatrician. During the 3 years since the outpatient clinic started in 2007, 325 children were diagnosed with cancer but the outpatient oncology database missed 247 (76%) children: these children either never attended the outpatient clinic (because they abandoned treatment, died or only required inpatient care) or were never registered.
The 436 patients consisted of 256 (59%) boys and 180 (41%) girls and the male/female ratio was 1.4:1. The number of new childhood cancer patients seen in MTRH ranged from 103 to 115 annually for the 4-year period (figure 2), with a yearly average of 109 patients.

Male and female childhood cancer patients diagnosed annually at Moi Teaching and Referral Hospital, Kenya (n=436).
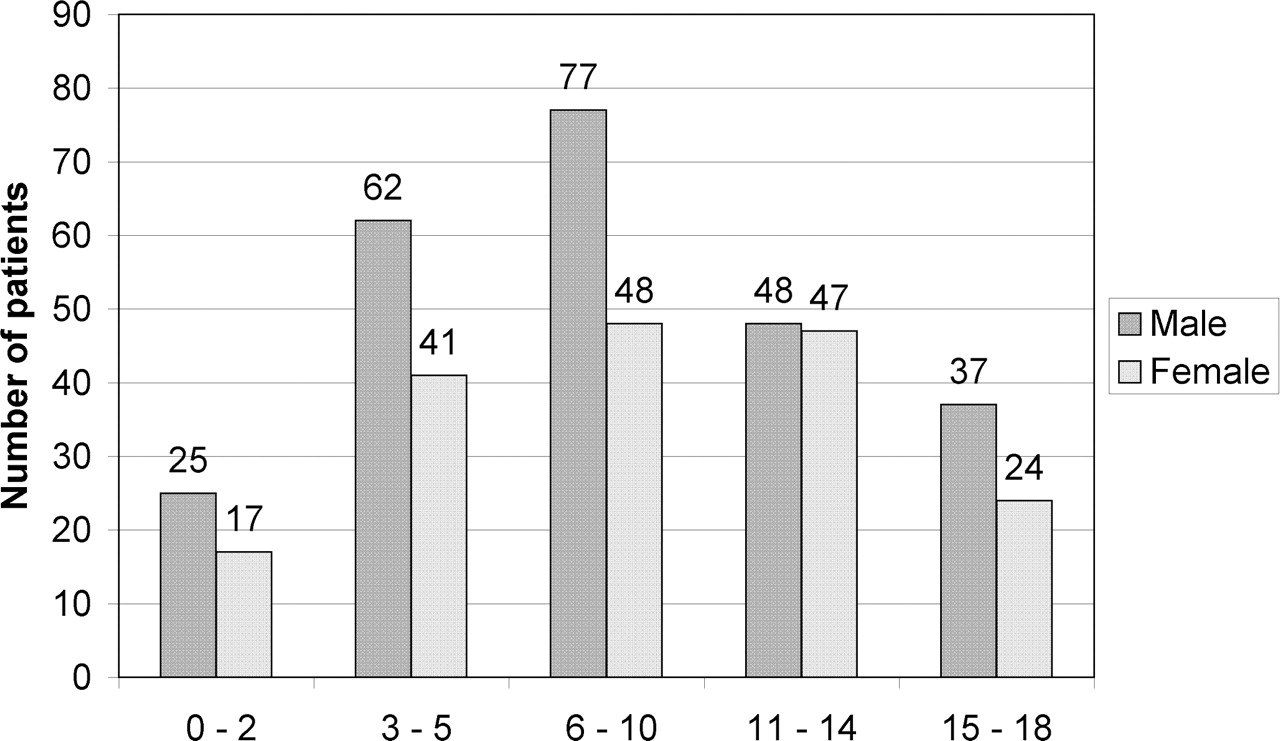
Age at admission was recorded in 426 (98%) children and ranged from 0 to 18 years (figure 3). The peak incidence of cancer was in the group aged 6–10 years (29%), mean 8.6 (SD 5.0), median 8. Table 1 presents the difference in expected and reported incidence of childhood cancer per million children under 15 years of age.

Age and gender at admission of childhood cancer patients diagnosed at Moi Teaching and Referral Hospital, Kenya (n=426).
Expected and reported incidence of childhood cancer per million children under 15 years of age
Figure 4 shows the distribution of the different types of cancer. A similar distribution of diagnoses was found in the three databases. Of all 436 children, in 11 (3%) only the primary site of the malignancy was known (such as the kidney), in 27 (6%) a specific diagnosis was not confirmed and in 398 (91%) a specific diagnosis was made. Of these 398 children, 246 (62%) had haematological malignancies, 4 (1%) brain tumours, 123 (31%) solid tumours and 25 (6%) rare tumours.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distribution of childhood cancers between 2006 and 2010 (n=436). *Such as nasopharyngeal carcinoma, germ cell tumours, hepatoblastoma, hepatocellular carcinoma and follicular thyroid carcinoma. **Only the primary site of the malignancy was known, for example, ‘renal tumour’.
Two types of haematological malignancies are responsible for almost half of all cases of childhood cancer in MTRH. Non-Hodgkin's lymphoma is by far the most common type of cancer (34%), followed by acute lymphoblastic leukaemia (15%), Hodgkin's lymphoma (8%), acute myeloid leukaemia (4%) and chronic myeloid leukaemia (2%). Brain tumours included glioma (0.5%), astrocytoma (0.3%) and medulloblastoma (0.3%). Solid tumours consisted of nephroblastoma (8%), rhabdomyosarcoma (7%), retinoblastoma (5%), Kaposi's sarcoma (5%), osteosarcoma (3%) and neuroblastoma (3%). Rare tumours included nasopharyngeal carcinoma (2%), germ cell tumours (2%), hepatoblastoma (0.5%), hepatocellular carcinoma (0.5%) and follicular thyroid carcinoma (0.3%).
Discussion
The area served by MTRH suggests that the number of paediatric patients with cancer is many times larger than the annual average of 109 patients who visit the hospital.9,–,11 There are numerous reasons why there are fewer reported than actual cases of childhood malignancies in low-income countries. Cancer cases can only be identified after diagnosis and accurate registration.9 12 Lack of parental education and low awareness of health issues delay seeking of medical help. Parents may not recognise symptoms of paediatric malignancies, or may believe cancer is incurable and therefore do not seek medical care.9 12 13 Parents may rely on traditional healers using herbs or witchcraft.14 Parents may not have a means of transport to a medical centre, or may not be able to pay for diagnostic procedures or treatment.15 16 Healthcare providers may not be skilled in recognising childhood cancer, and laboratory and imaging devices may be lacking.9 12 Personnel may also believe that cancer is incurable or that parents cannot afford treatment and therefore decide referral or treatment is not worthwhile.17 18 And if malignancies are accurately diagnosed, they may not be registered systematically.9 Each misstep can prevent documentation of cases, and results in a lower reported than actual incidence of cancer. These difficulties may be overcome by increasing public awareness of the symptoms, diagnosis and treatment of childhood cancer, emphasising the fact that most cancer can be cured, facilitating access to medical services for poor families, training healthcare providers, enhancing diagnostic capacities and rigorously improving record-keeping.
The distribution of malignancies in Western Kenya is similar to findings in other equatorial African countries but differs markedly from studies performed in high-income countries.12 19,–,25 Such differences may be the result of the cumulative effect of variable genetic predisposition, infectious diseases, environmental exposures and inaccurate registration.26 In high-income countries, haematological malignancies are the most common, followed by brain tumours and solid tumours.9,–,11 Our study reveals that haematological malignancies in Western Kenya are also the most prevalent cancers. However, in high-income countries acute lymphoblastic leukaemia is the most common haematological cancer, whereas in Kenya it is non-Hodgkin's lymphoma. Very few brain tumours are registered at MTRH. The substantial underestimation of brain tumours in low-income countries may be related to scarcity of the neuro-imaging facilities required for diagnosis and limited possibilities to perform tumour biopsies, and requires further exploration in the future.27 The group of solid tumours encompasses the second largest group of cancers in Kenya.
Our study showed that non-Hodgkin's lymphoma was the most common type of cancer in MTRH. In Kenya, Burkitt's lymphoma, a subtype of non-Hodgkin's lymphoma, is much more prevalent than in high-income countries due to increased infection rates with Epstein–Barr virus and immune stimulation by malaria.28,–,31 However, pathologists in MTRH are unable to distinguish Burkitt's lymphoma from other non-Hodgkin's lymphomas because fine needle aspirates are used for diagnosis, facilities for additional staining are lacking and technical challenges hinder the reading of slides.
We found a relatively low rate of acute lymphoblastic leukaemia. The difference between the reported and actual incidence of childhood malignancies in low-income countries is most striking for leukaemia, the symptoms of which resemble those of infections including malaria, and children can die before cancer is suspected or diagnosed. In lymphomas and solid tumours, visible symptoms encourage parents to seek medical help and early death is less common.9
We also found high numbers of retinoblastoma and Kaposi's sarcoma. Non-heritable retinoblastoma has a higher incidence among less affluent populations, suggesting an association with poor living conditions and an infectious aetiology. The high rate of Kaposi's sarcoma in Kenya is due to the high percentage of HIV-positive children.8 32,–,35 In one of our studies at MTRH, we found that 13% of childhood cancer patients were HIV-positive and that 57% of these HIV-positive children were diagnosed with Kaposi's sarcoma (unpublished data).
The absence of Ewing's sarcoma in MTRH is remarkable. In low-income countries a very low incidence of a particular malignancy may indicate systematic misdiagnosis, especially among malignancies that are difficult to identify without expertise and pathological diagnostic facilities. When Ewing's sarcoma, for instance, is often misdiagnosed as rhabdomyosarcoma, the rate of Ewing's sarcomas is strikingly low while that of rhabdomyosarcoma is remarkably high. This necessitates further investigation at MTRH. The diagnosis of certain tumour types may be limited by lack of access to specialised diagnostic stains.9
Our finding that more males than females develop cancer is in accordance with earlier studies in Africa, but is unexplained. It is known that slightly more males have cancer and that boys are more susceptible to Burkitt's lymphoma than girls. Some studies suggest that sex chromosome linked genes may play a role in the latter.12 20,–,23 Other possible explanations for male preponderance are cultural and economic. Parents may consider that boys are more important for the family, contribute more to society and will take care of their aging parents, leading to more frequent presentations of boys than girls to healthcare centres.23 36
Our study shows that there is a wide age distribution of malignancies in Kenya. This pattern is also found in other African countries but differs from that of high-income countries. In high-income countries most childhood cancers occur in children under 5 years of age, decrease between 6 and 14 years of age and increase again between 15 and 18 years of age.10 11 However, the largest group of children attending MTRH are between 6 and 10 years old, perhaps because the majority of children with acute lymphoblastic leukaemia (aged 3–6 years) die of complications before reaching hospital. In addition, parents are aware of the high death rate of children and so if those below 6 years of age fall seriously ill, more parents are resigned to the fact that they will die. However, when children are older they start to contribute to the family income and medical help will be sought sooner. The group of children aged 15–18 years with cancer is quite small.
Gathering data in a low-income country like Kenya posed several difficulties. Filling in of medical records is often not seen as a priority, and storage space is insufficient and frequently changed. Thus medical records were at times mixed up in piles in remote rooms which had not been opened for years. Many medical records were missing, while the records themselves were in poor condition, falling apart and missing notifications because papers had been torn from the files. Important information was either not categorised by date and issue or not documented at all. If medical records are unorganised, the status of patients is very difficult to monitor. Overall, getting access to medical records and extracting reliable data took substantial effort.
Before this study was carried out, information on patients was not gathered in a comprehensive or systematic manner at MTRH. None of the three databases was complete, indicating that the thoroughness and quality of the data sources require profound improvement: for example, all children in whom a malignancy is confirmed need to be recorded in the pathology database.
Our study provides an overview of childhood cancer patients presenting for treatment in Western Kenya over 4 years. We cannot confirm that we succeeded in collecting the names of all childhood cancer patients. However, local caregivers believe that we assembled the vast majority of files and that we are able to provide a reliable overview. Basic data for childhood cancer patients must be collected before improvements can be made. We also learned that more research on non-Hodgkin's lymphoma is advisable. This type of cancer, when diagnosed at an early stage, has a high cure rate, and so treating it successfully would demonstrate that cancer can be cured in Kenya and encourage patients, parents and medical staff. MTRH should continue and extend the new comprehensive cancer registration system to serve as the basis for an evidence-based oncology program, which may lead to better clinical results.9
Acknowledgments
The purpose of the Doctor 2 Doctor program, a collaboration between VU University Medical Centre (VUmc), Moi Teaching and Referral Hospital (MTRH) and KLM (Royal Dutch Airlines), is to share knowledge, improve treatment and increase the survival of children in MTRH. The authors are grateful to Brinio Veldhuijzen van Zanten from KLM and to Judith Stuijt, Kees Klarenbeek and John Roord at VUmc for their ongoing support of the Doctor 2 Doctor program. The authors thank the participants of the USAID-Academic Model Providing Access to Healthcare (AMPATH) program, the administrators at the medical records storage facilities, and the local caregivers at MTRH for their assistance.
S Mostert and F Njuguna are joint first authors and contributed equally to the content of the manuscript.
References
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.