Article Text

Abstract
Objective To explore the acceptance of uncoated drug-free mini-tablets 2 mm in diameter in children aged 0.5–6 years and their ability to swallow the mini-tablets.
Methods 60 children aged 0.5–6 years (10 subjects per year of life) were enrolled in our prospective, open random, two-way cross-over exploratory pilot study. The children were administered either an uncoated drug-free mini-tablet 2 mm in diameter with a beverage of their choice or 3 ml of glucose syrup 15% followed by the other formulation. Deglutition was visually assessed for the two different dosage forms using a predefined criteria list.
Results The study hypothesis was that children would accept the liquid formulation better than the solid mini-tablets. Surprisingly, the authors found that the acceptance of the mini-tablets, defined as immediate swallowing or chewing first with subsequent swallowing, was higher or at least equal to that of the syrup. Very young children (6–12 months) were fully capable of swallowing the mini-tablets and may even accept them better than the sweet liquid formulation. Some children aged between 2 and 4 years chewed the tablets before swallowing, but still accepted them quite well. The acceptance rate of the mini-tablets in the different age groups was much higher than expected.
Conclusions Uncoated mini-tablets seem to be a very promising alternative to liquid formulations and could be used at an earlier age in paediatric drug therapy than previously anticipated.
Statistics from Altmetric.com
Introduction
Liquids are the most frequently used drug formulations for young children. Although they are considered simple to administer and the dose can easily be changed, they also have major disadvantages such as chemical, physical or microbial instability, taste issues and lack of controlled release properties.1 Only a few safe excipients, solvents, preservatives and antioxidants are available.2 Masking the unpleasant taste of a drug is much harder to achieve in liquid than in solid forms, and the unpleasant taste may affect the accuracy of dosing.3
Recent European regulations4 and a WHO campaign5 have stimulated the development of novel products and clinical research in paediatrics. One option might be to increase the use of solid dosage forms.6 7 In the recent draft ‘Guideline on pharmaceutical development of medicines for paediatric use’,8 the European Medicines Agency (EMA) considered the acceptability of tablets as a function of children's age and tablet size (table 1). The main concern is inhalation of solid particles during administration.
Suitability of tablets according to the recent EMA/CHMP draft ‘Guideline on pharmaceutical development of medicines for paediatric use’6
What is already known on this topic
▶ It is generally assumed that young children have difficulty swallowing solid dosage forms.
▶ It is generally assumed that young children prefer sweet liquid drug formulations.
▶ Drug regulatory agencies do not accept tablet formulations for children aged <2 years.
What this study adds
▶ Most young children and infants are capable of swallowing small mini-tablets and accept them well.
▶ Solid and liquid formulations are accepted equally well by young children; indeed, mini-tablets seem to be superior.
▶ Based on our data there is no reason to refuse drug approval for small, dissolvable tablets for young children.
The current general consensus on the acceptability of dosage forms is based on the EMA/CHMP (Committee for Medicinal Products for Human Use) reflection paper6 which claims that children below 6 years of age have difficulties with, or are even unable to swallow, solid oral dosage forms. Only powders, multiparticulates and orodispersibles are considered suitable for children ≥2 years of age.
The aim of the present study was to explore the acceptance of 2-mm mini-tablets (figure 1) in children aged between 6 months and 6 years, which has not previously been investigated. The primary objective of the prospective study was to investigate differences in acceptability and ability to swallow two oral drug-free formulations: a glucose syrup and a 2-mm mini-tablet. Three secondary objectives were to identify the number of children who refuse to take an oral drug-free formulation, the number of children who spit it out, and any possible problems.

Drug-free mini-tablets (2 mm in diameter) used in the study.
Materials and methods
Mini-tablets were composed of microcrystalline cellulose (Avicel PH-105; FMC BioPolymer, Philadelphia, Pennsylvania, USA), α-lactose monohydrate (FlowLac 100; Meggle, Wasserburg, Germany), anhydrous colloidal silica (Aerosil 200; Evonik, Essen, Germany) and magnesium stearate (Bärlocher, Unterschleissheim, Germany). Glucose syrup was purchased from Caelo (Hilden, Germany).
For the production of the drug-free mini-tablets, all ingredients were blended in a Turbula T2F mixer (WA Bachofen, Muttenz, Switzerland) for 10 min and directly compressed on a Pressima rotary tablet press (IMA Kilian, Cologne, Germany) equipped with a Euro-B 19-tip tool (Ritter, Stapelfeld, Germany). Biconvex mini-tablets with a diameter of 2 mm and a mass of approximately 7 mg were obtained. Just before administration, the glucose syrup was mixed with tap water to produce a glucose concentration of 15%. The produced mini-tablets fulfilled all Ph.Eur. criteria for an uncoated tablet.9 The radial crushing strength was determined using a TA-XT2i texture analyser (Stable Micro Systems, Godalming, UK) as recently described10 and found to be 8.1±1.1 N (n=30) which enables handling without splitting or abrasion. To minimise the risk of aspiration and particle deposition in the lung, the disintegration time was checked using a DT2 (Sotax, Basle, Switzerland) modified for pharmaceutical pellets11 and found to be <5 s in purified water (37°C).
This exploratory pilot study in 60 children in six different age groups was performed using a single-centre, open, randomised, two-way cross-over design whereby every child received the two drug-free formulations as single applications. Patients were recruited in the University Children's Hospital of Heinrich Heine University, Düsseldorf. Children satisfying the inclusion and exclusion criteria (see below) were enrolled and randomised to the order of application of the two oral placebo formulations. The children were stratified into the following six age groups (10 children per age group): 0.5–1, 1–2, 2–3, 3–4, 4–5 and 5–6 years. Children had to be able to swallow. Any impairment of swallowing as a consequence of chronic illness (eg, cerebral palsy), acute illness (eg, gastroenteritis, respiratory tract infection) or oral deformation, led to exclusion from the study. Patients with lactose intolerance, nausea, fatigue or palsy due to previous or concomitant medication, as well as patients who had recently undergone surgical intervention were also excluded.
Parents received a detailed patient information sheet and children a comic explaining all patient-related aspects of the study. They were given adequate time to read and consider the information provided and to ask questions before they signed informed consent. One mini-tablet was placed on the tongue and the patient had to swallow it with up to three mouthfuls of a drink of their choice. Glucose syrup was either given with a pipette or a teaspoon depending on the child's ability to understand instructions. The glucose syrup had to be swallowed without any additional liquid. Swallowing was carefully observed. After deglutition the patient's mouth was inspected by the investigator using a flashlight and the criteria shown in table 2 used to evaluate the outcome. As soon as the child was ready for the second part of the study, the administration and assessment procedures were repeated with the other formulation within 10 min.
Evaluation criteria for the outcome of mini-tablet or syrup administration
The study was performed according to the requirements of the ICH E6 Guideline on Good Clinical Practice12 and was approved by the University Ethics Committee Düsseldorf (No. 3334). Study design support and data management were provided by the University Hospital Düsseldorf's Coordination Center for Clinical Trials (KKS) under registration code P_MINITAB. This pilot study was registered with the German Study Register under number DRKS00000396.
As this was an exploratory pilot study, only descriptive statistics were applied: proportion and 95% CI were calculated for the two primary endpoints ‘swallowed’ and ‘overall acceptance’ using Microsoft Excel.
Results
A total of parents of 120 children had to be approached to recruit the required 60 male and female children aged 0.5–6 years. Detailed criteria of the assessment procedure are provided in table 2.
Children aged 5–6 years were the only age group to completely swallow both the mini-tablet and the liquid formulation (figure 2). In the other age groups there were no clear differences between the mini-tablets and the glucose syrup. Some children in all age groups chewed the mini-tablet before swallowing, particularly those aged 2–3 years. In this age group the mean value of the ability to swallow, our first primary endpoint, is slightly higher for the syrup than for the mini-tablet. Only one child from the 1–2-year-old age group spat out the mini-tablet. For the very young children (0.5–1 year) the mean value of the ability to swallow was better for the mini-tablet than for the syrup (tables 3,4). When administering the liquid formulation we observed small runlets in three children in the youngest age group (0.5–1 year). Complete refusal of the administration was observed in all age categories except the 5–6-year-old children and, surprisingly, was much higher for the liquid (13) than for the solid (3) formulation. Almost 40% of the children aged 1–2 years refused the liquid formulation, but only 10% refused the mini-tablet. It is important to mention that none of the 60 children choked on either the mini-tablet or the syrup and that no adverse events occurred during the present study.
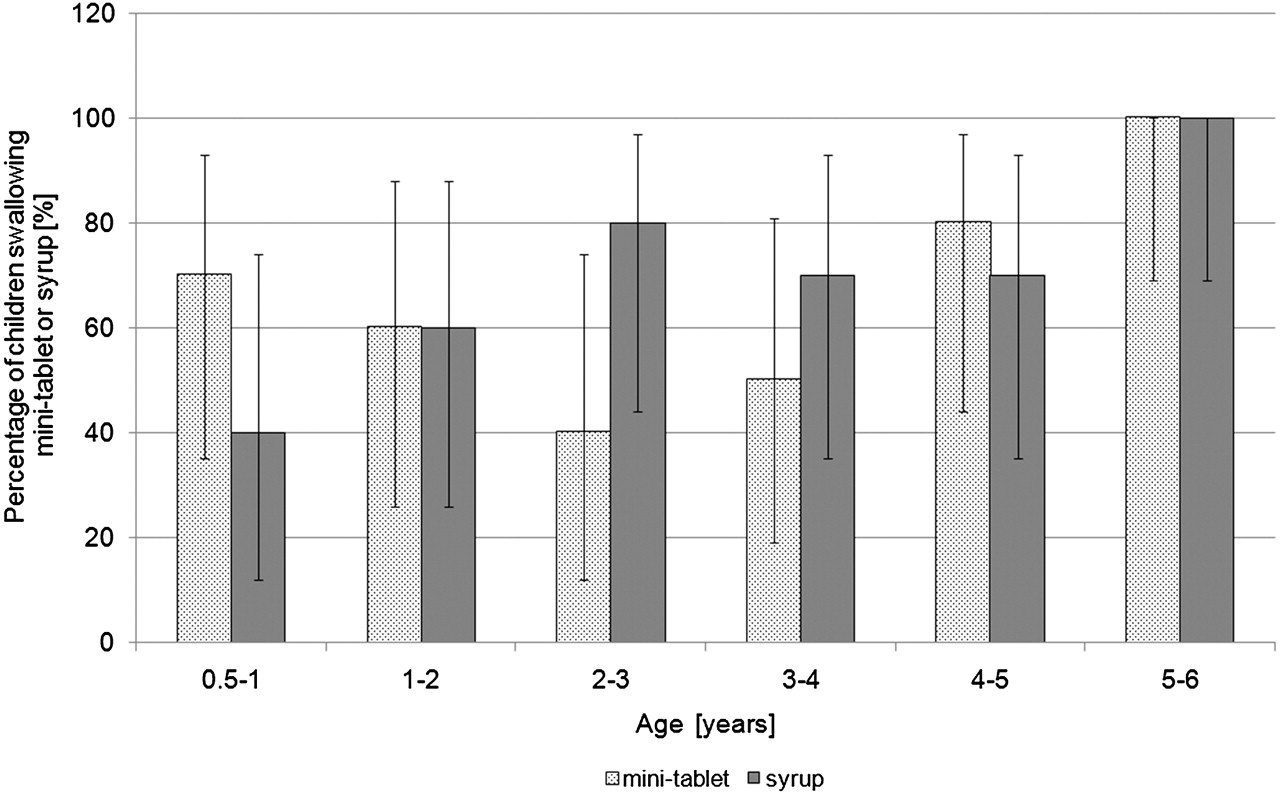
Children's ability to completely swallow mini-tablets and glucose syrup (n=10 per age group; mean±95% CI).
Results for the mini-tablet formulation
Results for the glucose syrup
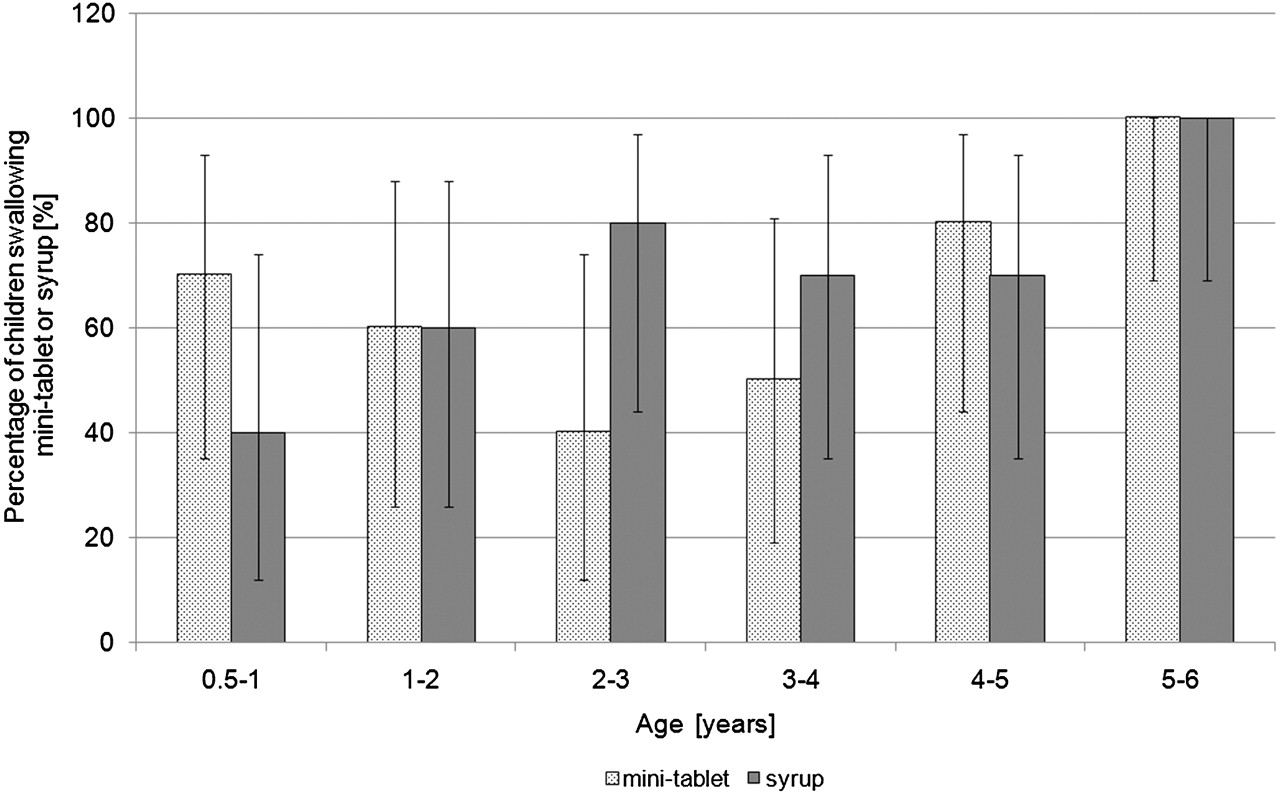
Swallowing and chewing (with subsequent swallowing) of the uncoated mini-tablet was considered overall acceptance (figure 3). The mean acceptance of the uncoated mini-tablet was higher or at least equal to that of the syrup in all age categories.

{kind=link}
{kind=link}
{kind=link}
Overall acceptance of mini-tablets and glucose syrup in children <6 years of age (n=10 per age group; mean±95% CI).
Discussion
Our study demonstrates that mini-tablets might be an alternative option as drug carriers for children. Based on the available literature, we anticipated that, depending on age, the mini-tablets would be less acceptable than the syrup, but this was not found. The main limitation of our study is the small number of patients since it was designed as a pilot study.
In 2009, a prospective study was published on the acceptance of drug-free mini-tablets (3 mm in diameter), without a liquid control, in 100 children aged 2–6 years. Overall, 46% of the 2-year-old children were able to swallow the mini-tablets, increasing up to 86% for the oldest children. The authors therefore reported that it was safe to use 3-mm mini-tablets in children aged 4–6 years.13 Our results are in clear contrast to current expert opinion and the recommendations of regulatory agencies. The mean acceptance values for the liquid formulation are not superior to the mean values for the mini-tablet. Obviously, the poor acceptance of liquids is often neglected in discussions on the suitability of dosage forms. Furthermore, different conditions and requirements in developing countries are often ignored. Hot and humid climates may seriously affect the stability of liquid formulations and access to clean water as well as high transport and storage costs have also to be taken into account.
Conclusion
This exploratory study indicates that mini-tablets might be a suitable method for administering drugs, especially in young children. The surprising outcome of our study is that the overall acceptance of 2-mm uncoated mini-tablets is at least equal to or even better than that of sweet tasting syrup, even for children aged 2 years or less. This may have some implications. First of all, the study should be repeated with a larger cohort to statistically corroborate our results and confirm safety. Further, it should be explored whether the observed chewing before swallowing, especially in children aged 2–4 years, has an impact on the usability of coated mini-tablets. The industry should consider 2-mm mini-tablets as a modality for the safe delivery of small doses to young children. The WHO position on solid small sized drug carriers is supported by our study. The EMA should adopt uncoated 2-mm mini-tablets in its recent draft guideline for children aged ≥6 months.
Acknowledgments
The authors gratefully acknowledge the assistance of Indira Hodzic in mini-tablet production, the cooperation of KKS for preparing the in vivo study and all staff members of the University Children's Hospital in Düsseldorf for their continuous support.
Footnotes
-
Competing interests None.
-
Ethics approval The Ethics Committee of Düsseldorf University approved this study (No. 3334).
-
Provenance and peer review Not commissioned; externally peer reviewed.