Article Text

Abstract
Stevens–Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are rare life-threatening conditions almost exclusively attributed to drugs. The incidence in children is lower than in adults and has a better outcome. Mycosplama pneumoniae infection may be involved in some cases of paediatric SJS. The main etiologic factors for both SSJ and TEN are sulphonamides and anticonvulsants, followed by penicillins and non-steroidal anti-inflammatory drugs. In rare instances, paracetamol is the only suspected drug. By contrast with adults, allopurinol, oxicams and nevirapine are not identified as causative agents in children, probably due to differences in drug prescriptions. The only aspects of treatment that have been proved to improve survival are the rapid withdrawal of the suspected offending drugs and an optimal supportive therapy with emphasis in nutritional support, accompanied by management of denuded skin areas. The use of specific therapies remains controversial.
- Dermatology
- Intensive Care
- Multidisciplinary team-care
Statistics from Altmetric.com
Introduction
In 1922, Stevens and Johnson described two children who developed an acute mucocutaneous syndrome characterised by extensive mucosal necrosis and purpuric macules on the skin associated with fever, stomatitis and ophthalmia, with a probable infectious origin.1 Thereafter in 1956, Lyell described four patients who developed a more extensive skin necrosis, resembling scalding of the skin.2 These conditions became widely known as Stevens–Johnson syndrome (SJS) and Lyell syndrome or toxic epidermal necrolysis (TEN), respectively. SJS and TEN are rare, life-threatening, severe cutaneous adverse reactions that affect both adults and children. The considerable overlap in the cardinal clinical, aetiological and histopathological features of both entities justifies them to be considered clinical presentations of the wider spectrum known as ‘SJS/TEN’.3 ,4 The main difference lies in the percentage of body surface area (BSA) presenting skin detachment, and is defined SJS when epidermal detachment affects less than 10% of BSA, SJS/TEN overlap when the detachment ranges from 10% to 30%, and TEN when it affects more than 30%.3 Herein, we make an update on SJS/TEN in children, focusing on clinical manifestations and clues to differential diagnosis, pathogenesis, identification of medications associated with a risk for SJS/TEN, diagnosis and management.
Childhood SJS/TEN presents several unique aetiological, prognostic and therapeutic challenges, and despite there being an extensive work of literature regarding this topic in paediatric patients, most publications refer to single case reports or a small number of patients, which complicates the possibility of drawing real conclusions.
SJS/TEN has been observed worldwide with an annual incidence of 1–2 cases per million inhabitants,5 and occurs in all age groups including children, infants and even newborns, who comprise 10–20% of reported paediatric cases.6 The incidence increases with age likely due to increases in drug prescriptions and comorbidities modifying drug effects. Adult SJS may lead to death in up to 5%, while 30% of cases of adult TEN may be fatal.5 Mortality rates in children are highly variable, but seem to be lower than in adults.6 ,7 Sequelae of SJS/TEN are most commonly related to mucosal involvement, mostly ocular.8
Clinical manifestations
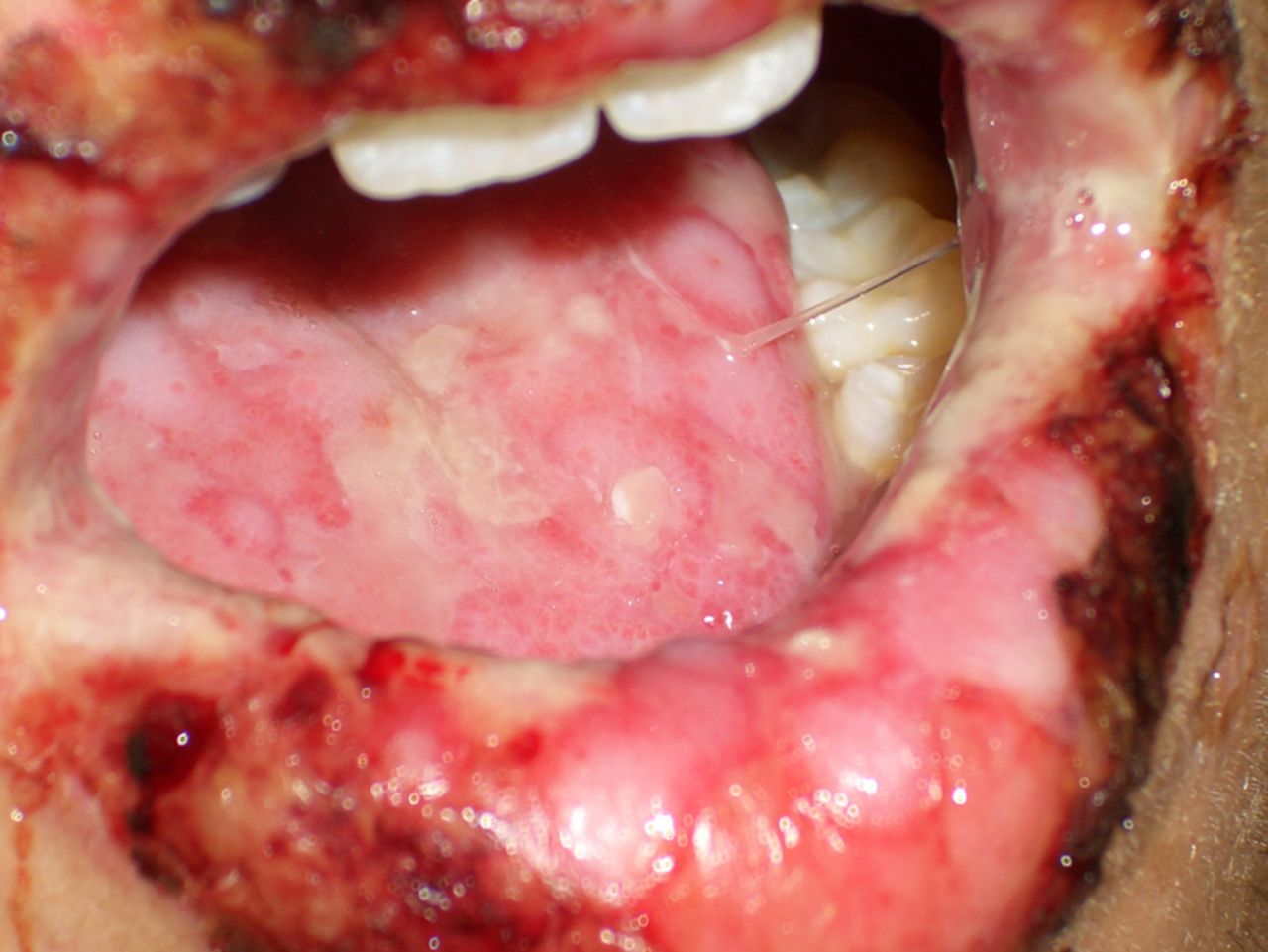
Clinical manifestations in children overlap with clinical presentation in adults.9 SJS/TEN is an acute inflammatory disease, characterised by fever, malaise, cutaneous and mucosal lesions, commonly preceded by prodromal symptoms lasting 1–7 days. The prodromal period is characterised by non-specific symptoms, such as malaise, fever, ocular pruritus and dysphagia. Erythema, erosions, scabs and pseudomembranes gradually develop in the oral, genital and ocular mucous membranes. Inflammation and soreness of the mouth and genitalia is frequent, and usually precedes the skin lesions by a few days3 ,7 ,10 (figure 1).

A 17-year-old male patient diagnosed with Stevens-Johnson syndrome due to azitromicine. Erosions and crusts on the lips with diffuse ulcers on the tongue.
Skin lesions vary in severity, presenting as red macules and papules that sometimes coalesce to a generalised erythematous rash with atypical targetoid lesions, and progress to vesicles, bullae and extended skin necrosis that detaches in large sheets9 ,10 (figures 2⇓–4). When the leading cutaneous finding is erythema, the Nikolsky sign may guide the diagnosis, although it is not exclusive of SJS/TEN. Nikolsky sign is defined as an epidermal detachment that appears when applying a tangential pressure on erythematous, non-blistering skin. In cases with a Nikolsky sign, the patient should be admitted to a burn care unit with a suspect diagnosis of SJS/TEN.3

Atypical target lesions in a 1-year-old female patient with Stevens–Johnson syndrome due to phenobarbital.

Initial phase of toxic epidermal necrolysis with diffuse erythema and vesicles that will evolve to full epidermal necrosis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
A 5-year-old female patient with toxic epidermal necrolysis with three suspected drugs (penicillin, ibuprophene and paracetamol).
Practically all patients present affected mucous membranes with varying severity, which is often painful and haemorrhagic. Common symptoms include purulent conjunctivitis and inflammation, erosions, ulcers and crusts of other mucosal surfaces like the mouth, nose, pharynx, respiratory and digestive tracts, and anogenital mucosa, which may result in potentially life-threatening complications, such as bleeding and infection.8 Very severe cases may additionally develop renal and/or hepatic failure.
Differential diagnosis
SJS/TEN represents a very severe form of drug-induced reaction. The differential diagnosis includes entities such as drug-induced linear IgA. Linear IgA is an autoimmune subepidermal blistering disease that may be associated with drug exposure (mainly, vancomycin). The diagnostic hallmark of this condition is the linear deposition of IgA at the basal membrane of perilesional skin observed by direct immunofluorescence.11 Other entities that should be ruled out include drug rash with eosinophilia and systemic symptoms (DRESS), a multisystemic disorder characterised by a skin eruption with oedema that evolves to form blisters, accompanied by peripheral eosinophilia >1.5×109/L, atypical lymphocytes and systemic abnormalities.12 Most common drugs responsible for this disease are anticonvulsants, sulphonamides, minocycline and allopurinol. A drug-induced maculo-papular exanthema should also be excluded, as this is the most common cutaneous adverse drug reaction. This rash may evolve to an extensive desquamation which can occasionally be confused with TEN. Mucosal involvement is rare. Sometimes, at the onset of the rash, a more ‘dusky’ hue of the lesions may support a diagnosis of SJS/TEN, as it is thought the darker hue may herald the skin detachment.13 Staphylococcal scalded skin syndrome (SSSS) should also be included in the differential diagnosis. The syndrome is induced by epidermolytic exotoxins A and B, which are released by Staphylococcus aureus. The clues for correctly identifying SSSS include the absence of mucosal involvement, a Nikolsky sign present in both erythematous and ‘apparently normal’ skin and no prior history of drug intake.14 Finally, erythema multiforme is characterised by the appearance of typical target lesions showing three concentric well-defined areas of different skin colour or raised atypical targetoid lesions at acral sites. There often appears a subtle inflammation of the oral mucosa accompanied by a swollen lip, but not a true mucositis with erosions and haemorrhagic crusts like in SJS/TEN. It affects predominantly young and healthy people, and herpes simplex virus may be responsible for most cases. The clinical course is mild and may frequently recur. It is considered a distinct entity from SJS/TEN.15 ,16
Pathogenesis
SJS/TEN is considered a delayed-type hypersensitivity reaction (or type IV reaction), reinforced by the fact that these reactions resolve upon removal of the drug and occur more rapidly on drug reintroduction.17 ,18 However, the immune-physiopathology of SJS/TEN is not fully understood and remains controversial. The major pathological finding in this disease is a widespread apoptosis of keratinocytes, but it is still unknown how a certain drug may actually induce epidermal necrosis. The Fas-Fas ligand interaction and activation of caspase enzymes are pathways involved in apoptosis that could, in part, be responsible for this disease. On the other hand, TEN and SJS blisters have shown to be rich in cytotoxic T-cells and natural killer cells that would induce damage via perforin/granzyme B/granulysin and tumour necrosis factor-α.6 ,19
Over the last decade, there have been many associations between SJS/TEN and Class I and II Human Leucocyte Antigens (HLA) alleles of the MHC (major histocompatibility complex). Several non-mutually exclusive models have been proposed to explain how small molecular synthetic compounds (the drugs) are recognised by T cells in an MHC-dependent fashion, including the hapten concept/prohapten model, the p-i model (pharmacological interaction of drugs with immune receptors), and the altered repertoire model.18
Genetic susceptibility also plays a crucial role in the development of SJS/TEN. HLA-B1502 has been associated with carbamazepine-induced SJS in a Han Chinese population,20 and HLA-B5801 with allopurinol-induced SJS/TEN has been linked to a Japanese population.21 However, those findings could not be confirmed in Europe. Thus, the risk of SJS/TEN is related to the exposure with high-risk drugs, and also to a genetic predisposition.22 In order to improve the safety of drugs, it would be interesting to evaluate on preclinical drug screening programmes the interaction between the drug and the HLA.17
On the other hand, drug reactions generally occur with greater frequency in situations where there is a build up of chemically reactive metabolites, for example, when a decrease in enzymatic metabolism is found. In this sense, polymorphisms in gene families of detoxifying enzymes have been identified, above all in the CYP450 family, which affect drug kinetics and toxicity. Moreover, some patients with SJS/TEN have a low N-acetylating capacity, which predisposes them to serious cutaneous adverse reactions.23
Aetiology
Most cases of SJS/TEN are clearly linked to medications; however, in approximately 5% of cases a drug cannot be identified.24 Although TEN is almost exclusively attributed to drugs, some cases of SJS may be caused by Mycoplasma pneumoniae infection.25 Infections by virus (coxsakie, influenza, Epstein–Barr, human herpes virus 6 and 7, cytomegalovirus, parvovirus), bacteriae (streptococcus β-haemolyticum, group A), mycobacterium, and rickettsia could be potential cofactors or triggers in association with drugs.6 By contrast with adults, the number of published cases in the literature reporting comorbidities is low, with a single case of SJS/TEN arising in a patient with Crohn's, and no patients with HIV, lupus erythematosus, or cancer having been published.23 ,26 As only two paediatric case series with a complete prior history are reported, it is impossible to conclude whether the aforementioned disorders pose a potential risk for SJS/TEN development in children as they do in adults.
SJS/TEN is considered to be drug related if the patient is exposed to the offending agent within 8 weeks prior to the onset of the rash. An infectious origin is considered if the infectious process is noted to take place 1 week prior to the onset of the rash, and titre and/or cold agglutinins (IgM) of the infectious agent are available.26 ,27 Sometimes, both drugs and infectious agents are identified as possible precipitants to the disease, which makes identifying the real culprit a difficult task. For example, when the beginning of the suspicious drug intake concurs with the prodromal symptoms of the rash, the drug could represent treatment of the underlying illness and not a causal association with SJS/TEN. It is biologically plausible that an interaction between an infectious agent and a drug or its metabolite, may precipitate severe skin reactions.27 The infection would probably act as a cofactor in those cases.
Mycoplasma pneumoniae mainly causes atypical pneumonia, but it can also lead to neurological, hepatic and cardiac disorders. Moreover, it has been demonstrated to cause SJS predominantly in childhood and adolescence, a period where infections by this agent are more frequent.25 A clear relationship between M pneumoniae and SJS/TEN has been established in cases of documented SJS without prior exposure to any drug. An interesting study of Kunimi et al compared the clinical characteristics between drug-induced SJS and M pneumoniae-associated SJS in an Asian population. They found no differences with regard to skin, oral or genital lesions, but ocular involvement was significantly more frequent in M pneumoniae-associated SJS than in the drug-induced group (94% vs 64%). With regard to internal organ involvement, hepatitis was more frequent in drug-induced SJS, while respiratory disorders predominated in the M pneumoniae-associated SJS.25
More than 200 drugs have been associated with SJS or TEN, most commonly sulphonamides, anticonvulsants, non-steroidal anti-inflammatory drugs (NSAID) (oxicams), allopurinol and penicillins.24 ,27 ,28 Most studies in children describing aetiological factors are single case reports, although there are a few series reported (table 1).9 ,24 ,26 ,27 ,29–31
Review of literature of causes of SJS/TEN including all case series with 10 or more paediatric patients
The largest cohort was published by Levi et al and used a pooled analysis from two multicentre case-control studies (SCAR – severe cutaneous adverse reactions – and euroSCAR) including 80 patients and 216 matched controls below the age of 15, and concluded that sulphonamides and anticonvulsants (phenobarbital, lamotrigine, and carbamazepine) were the most frequent causative drugs.24 Recent infection with M pneumoniae had been reported in 9% of cases in this cohort, and the window of drug exposure was restricted to 7 days prior to the index day, except for phenobarbital, which has a longer half-life, where it was extended to 3 weeks.
To summarise, most studies in children conclude that the highly suspected drugs responsible for SJS/TEN are sulphonamides and anticonvulsants, including phenobarbital, lamotrigine and carbamazepine.9 ,26–31 However, other drugs, such as penicillins, cephalosporins (a drug rarely involved in adult SJS/TEN), valproic acid, NSAIDs (excluding oxicams in this age group), and paracetamol may pose a potential risk in children.24 ,26 ,27 ,31 By contrast with adults, allopurinol, nevirapine and oxicam NSAIDs were not identified as causative agents in children.28 Drug prescription patterns may be responsible for the changes in the drugs held responsible for disease. In children, anticonvulsants might be mainly used for seizures and attention deficit and hyperactivity disorder. Valproic acid has been identified as an independent risk factor from other highly suspected antiepileptic agents evaluated, and it seems to also convey a higher risk for SJS/TEN.24 Among antibiotics, sulphonamides have become a second-line treatment in most infections, but are also used for chronic digestive diseases, such as Crohńs or ulcerative colitis. Other antibiotics include penicillins, cephalosporins and macrolides, all of them linked to SJS/TEN in several studies of single patients.26 ,27 ,30 ,31
Importantly, in most cases of children with SJS/TEN, there is more than a single drug that could be considered suspect and, therefore, the term ‘suspicious’ rather than ‘causative’ should be used.24 ,26
Diagnosis
The diagnosis of SJS/TEN is mainly clinical, although a skin biopsy showing full epidermal thickness necrosis accompanied by a scarce dermal inflammatory infiltrate may help confirm the diagnosis.
Pinpointing the exact causative agent may be difficult, as there is no definitive laboratory test to confirm the role of suspect agents. In children, disease is more likely to be linked to a drug as they are usually treated with a lower number of drugs. When we suspect a diagnosis of SJS/TEN, we must obtain a detailed medical history listing all new medications taken during the 8 weeks prior to the disease onset, although in our experience, the most important window is the 1 or 2 weeks prior to the onset of the eruption.
Moreover, an infectious origin should always be ruled out and patients should be tested with serology tests (IgM and IgG) and PCR (to assess viral replication) for herpes simplex virus 1 and 2, varicella-zoster virus, cytomegalovirus, Epstein–Barr virus, human herpes virus 6 and 7, parvovirus and M pneumoniae.25 ,32
There is some controversy regarding the usefulness of lymphocyte transformation tests to find causative drugs, with results showing many false positive and negative results. This is a safe and reproducible test used to assess activation of drug-specific T cells in vitro, but in SJS/TEN, it needs to be performed within the first week after onset of the rash to aid in the diagnosis.33 Patch testing has not proven useful in SJS and TEN. Drug challenges with suspected drugs are contraindicated in TEN, because second episodes can be fatal.
Treatment
The most important actions to be taken when a child is affected from SJS or TEN are the rapid withdrawal of the offending drug and a prompt admission to a specialised burn unit or paediatric intensive care unit, as this has been shown to directly decrease morbidity and mortality rates.29 ,33–37 It is therefore crucial to increase awareness of SJS/TEN and aim for early specialist referral.
General care measures include the care by multidisciplinary teams which include specialist physicians and nurses versed in managing extensive cutaneous denouement and mucosal sloughing. Full care of the patient includes ophtalmological revisions and supportive care, with special emphasis on wound management, fluid balance, respiratory and nutritional support, aggressive septic monitoring, pain management, physical and occupational therapy and psychosocial attention.29 ,34–37 The nutritional needs of children with SJS/TEN is an aspect of care that is often neglected. Energy requirements of paediatric patients with SJS/TEN are increased, and the application of a 30% factor to resting energy requirements should be made when calculating nutritional support.38
The local wound treatment is important to avoid complications derived from the loss of barrier function, and includes gentle debridement of broken blisters, removal of necrotic epithelium, topical treatment with antimicrobials, and wound coverage with either biological or traumatic biosynthetic wound dressings.37 In our opinion, silver sulfadiazine-impregnated dressings should be used, except when sulphonamides are included in the suspected drugs, as these dressings are safe, effective and inexpensive.
Literature of specific treatment in children is scant and controversial, with a lack of clinical trials, and only a few observational studies hindered by a low number of patients. In general, there are two principal trends toward specific treatments for SJS/TEN in children. The most commonly studied therapy by far is the use of intravenous immunoglobulins (IVIG), followed by corticosteroid treatment. IVIG have shown promising results because it inhibits Fas-mediated apoptosis in sensitive cell lines by blocking Fas receptors. Most studies have shown that, when used at a dose of 2–4 g/kg within the first 4 days of onset of skin eruptions, patients appear to have a shorter time to cessation of disease progression and complete re-epithelisation, and also have trend towards a better survival rate.39–41 On the contrary, a few studies did not show any benefit on mortality rates.42 On the other hand, corticosteroids have shown good results in some studies, mostly when used during the first days, but also an increased risk of complications and a failing of efficacy in some cases.19 ,43
Other specific treatments include cyclosporine, plasmapheresis, TNF-α inhibitors or a combination of different drugs.19 ,43 In adults, the only therapeutic measure which has proven effective at reducing mortality rates is intensive supportive care.44 On the contrary, a recently published meta-analysis focused on management of SJS/TEN in children, found that patients treated only with care support had a higher morbidity and mortality, and although the literature is scant, patients treated with steroids and IVIG seemed to have a better outcome.43
Systemic antibiotics should only be considered in patients with clinical signs of infection, and always guided by sensitivity assays from systematic cultures of the skin, mucosae, catheters and urine.45
SCORTEN is a TEN-specific severity of illness score used to predict the risk of complications and mortality and is calculated within 24 h after admission. It is also used to evaluate if a therapeutic intervention reduces the complications that we observe versus what was expected based on the SCORTEN prediction.46 ,47 It is based on seven prognostic factors: age, malignancy, surface area involved, heart rate, serum urea, bicarbonate and glucose; however, its use in the paediatric population has not yet been validated.
Recovery may be slow, taking several weeks, and may be even longer in TEN patients. Healing occurs leaving scars in mucosal sites or hairy areas. Long-term sequelae may include hypopigmentation or hyperpigmentation changes, alopecia, anonychia, strictures or chronic ulcers in mucosal areas, and even impaired vision and blindness.26
Conclusions
SJS and TEN are rare life-threatening conditions mostly attributed to drugs. An infectious origin may be responsible for several SJS cases, but it may also act as a cofactor in other cases. In most paediatric patients, sulphonamides and anticonvulsants are the more likely drugs responsible, however, other drugs, such as penicillins and NSAIDs may also be a potential threat. Early withdrawal of suspected drugs and a prompt admission to a specialised burn unit, with emphasis in nutritional support, have proved to improve survival rates.
Acknowledgments
We wish to acknowledge Dr Amaya Viros (Signal Transduction Team, The Institute of Cancer Research, London, UK) for her critical review of the manuscript.
References
Footnotes
Contributors Both authors contributed to conception and design of the manuscript, in drafting the article and final approval of the version to be published.
Competing interests None.
Patient consent Obtained.
Provenance and peer review Commissioned; externally peer reviewed.