Article Text

Abstract
Neonatal jaundice is predominantly a benign condition that affects 60%–80% of newborns worldwide but progresses to potentially harmful severe hyperbilirubinaemia in some. Despite the proven therapeutic benefits of phototherapy for preventing extreme hyperbilirubinaemia, acute bilirubin encephalopathy or kernicterus, several low-income and middle-income countries (LMIC) continue to report high rates of avoidable exchange transfusions, as well as bilirubin-induced mortality and neurodevelopmental disorders. Considering the critical role of appropriate timing in treatment effectiveness, this review set out to examine the contributory factors to the burden of severe hyperbilirubinaemia and kernicterus based on the ‘three delays model’ described by Thaddeus and Maine in the 91 most economically disadvantaged LMICs with Gross National Income per capita ≤US$6000 and median human development index of 0.525 (IQR: 0.436–0.632). Strategies for addressing these delays are proposed including the need for clinical and public health leadership to curtail the risk and burden of kernicterus in LMICs.
- Jaundice
- Neonatology
- Tropical Paediatrics
- Neurodevelopment
Statistics from Altmetric.com
Introduction
Severe neonatal jaundice or hyperbilirubinaemia remains the most common cause of morbidity in the first week of life, affecting 60%–80% of newborns worldwide.1 ,2 The incidence of severe hyperbilirubinaemia in industrialised countries based on objective assessment of bilirubin levels ranges from 2.0 to 45 per 100 000 live births and of acute bilirubin encephalopathy (ABE)/kernicterus from 0.4 to 2.7.3 ,4 Unfortunately, similar estimates using population-based data are lacking in low-income and middle-income countries (LMIC) as severity of hyperbilirubinaemia is commonly based on clinical judgement and the need for phototherapy and/or exchange transfusion.5 However, the burden of severe hyperbilirubinaemia is commonly projected to be significantly higher due to the prevalence of aetiological/risk factors, such as glucose-6-phosphate dehydrogenase (G6PD) deficiency, blood group incompatibilities, low birth weight/prematurity and sepsis/meningitis.6–9 For example, a recent report on the global burden of hyperbilirubinaemia spearheaded by the Child Health Epidemiology Reference Group suggests that sub-Saharan Africa and South Asia are the leading contributors to an estimated 1.1 million babies who would develop severe hyperbilirubinaemia worldwide every year.8 Additionally, several hospital-based studies consistently report substantially higher rates of exchange transfusion and bilirubin-induced neurological dysfunctions (ABE/kernicterus) than reported in developed countries.10–12 It is, therefore, not surprising that bilirubin-induced mortality11–16 and neurological disorders, such as auditory deficits, cerebral palsy, autistic spectrum disorders, epilepsy and general developmental delays secondary to ABE/kernicterus,17–20 are commonly reported in the region (see web table 1).
The onset of severe hyperbilirubinaemia in the vast majority of infants worldwide occurs outside hospitals. Whereas the inability to identify and manage at-risk infants prior to hospital discharge in a timely manner is often cited as the major root cause of adverse outcomes in developed countries,21 the high proportion of non-institutionalised delivery in residential or traditional maternity homes in the vast majority of LMICs suggests that the contributory factors are likely to transcend systems failure. For example, while phototherapy and/or exchange transfusion are proven treatments to prevent or treat ABE and kernicterus worldwide, high rates of adverse outcomes among infants treated with phototherapy and/or exchange transfusion are not uncommon,22 underscoring the potential role of appropriate timing for the effective treatment of the affected infants.11–14 We, therefore, set out to explore the available evidence in the literature on the care-seeking pathways for infants with neonatal jaundice in LMICs based on the conceptual framework proposed by Thaddeus and Maine23 which focuses on three phases of delay: the decision to seek appropriate care, reaching an appropriate health facility and receiving adequate/appropriate care.
Pathways to the care of jaundiced infants in LMICs
Eligible focus countries and literature search strategy
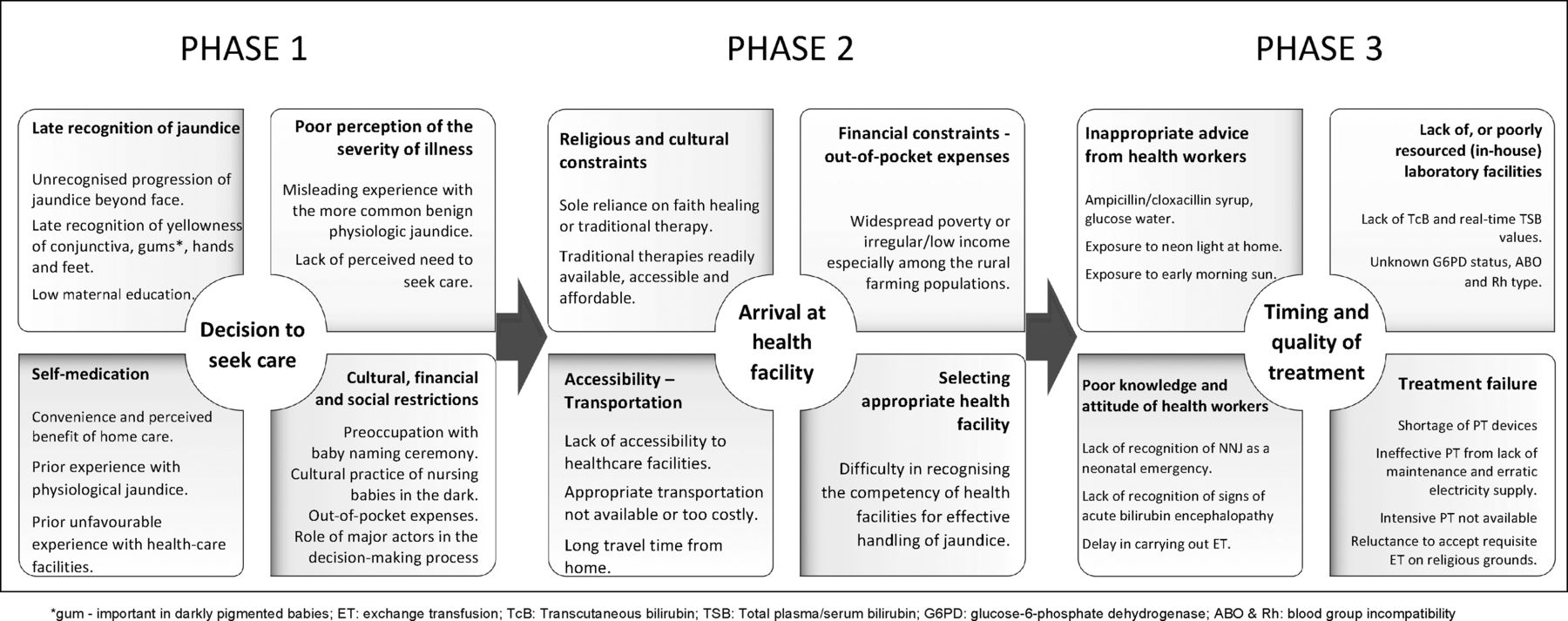
In view of the wide variation in income distribution and developmental status among approximately 140 countries classified as LMICs by the World Bank, we selected the 91 countries with Gross National Income per capita of ≤US$6000 using the Human Development Report 2013 published by United Nations Development Programme in order to focus on the most disadvantageous LMICs (see online supplementary appendix 1 and the box 1).24 An extensive literature search of publications between 1970 and 2013 was conducted to identify the range of issues directly or indirectly related to the three phases of delay as reported in the eligible countries. The search terms ‘neonatal jaundice’ OR ‘neonatal hyperbilirubinaemia’ AND ‘country name’ was applied to PubMed, Scopus, Ovid EMBASE, Cumulative Index to Nursing and Allied Health Literature, WHO Library Database, African Index Medicus and African Journals Online. The key findings which may vary in scope across the countries are summarised in figure 1.
{kind=link}
Phases of delay in the management of neonatal hyperbilirubinaemia in low-income and middle-income countries.
Profile of eligible low-income and middle-income countries used for this review
The Human Development Report 2013, published by United Nations Development Programme, presents country rankings using a Human Development Index (HDI), a robust composite measure of the average achievement in three basic dimensions of human development namely: a long and healthy life (health), knowledge (education) and a decent standard of living (income). The eligible 91 countries account for 64.2% of the total annual live births of roughly 135 million globally, have median institutionalised delivery of 65% (IQR: 43.8%–82.8%) and a median HDI of 0.525 (IQR: 0.436–0.632) compared with 0.878 (IQR: 0.825–0.878) for the 50 most developed countries. By world regions, 42 (46%) countries are from sub-Saharan Africa (SSA), 18 (20%) from East Asia & Pacific (EAP), 10 (11%) from Latin America & Caribbean (LAC), 8 (9%) from Middle East & North Africa (MEN), 7 (8%) from South Asia (SOA) and 6 (6%) from Europe & Central Asia (ECA). Urbanised population averages 27% in SOA, 36% in SSA, 37% in EAP, 44% in ECA, 52% in MEN and 56% in LAC. It ranges from 11% in Burundi to 83% in Jordan. About a third (33 countries) have at least half a million live births annually accounting for over half (58%) of global births and with a median institutionalised delivery rate of 47% (IQR: 35%–65%). Some 65 countries are within the tropical zone.
Delay in seeking appropriate care (phase 1)
Delay in seeking care promptly for newborn illness as a major contributor to adverse neonatal outcomes is well documented.25 The leading causes of such delays for infants with neonatal jaundice include late or failed recognition of the onset of severe jaundice, poor perception of the severity, recourse to self-medication as well as financial or sociocultural barriers.11–13 26–30 Several studies suggest, more commonly among multiparous mothers, a high level of awareness and recognition of neonatal jaundice typically from the yellowish discolouration of the baby's skin, sclera and mucous membranes.13 ,26 However, poor knowledge of the risks and dangers inherent in severe newborn jaundice, the temptation from prior experience to presume that all jaundice is physiological, or inappropriate advice from health workers often account for delay in taking prompt action.13 ,28 ,29 In some cultures, mothers may also be reluctant to leave home before the traditional naming ceremony typically from the 8th day of delivery. Frequently, they only begin to worry when their babies become unusually lethargic, irritable and restless by which time neurological damage would have occurred.12 ,26 It is not uncommon also for mothers to resort to self-medication with antibiotics, vitamins or various traditional therapies including herbal preparations and exposure to direct sunlight as first-line treatment.13 ,26–28 For example, in one survey enquiring knowledge of possible treatment options for jaundice among mothers, exposure to sunlight by mothers was cited by about half (51%), giving glucose drinks to the baby by 27% and use of oral antibiotics by 23% of the respondents.27 It is only when these efforts prove ineffective that frantic attempts are made to seek medical attention. This sequential health-seeking practice results in significant delays to hospital presentation, often necessitating emergency treatment with exchange transfusions.11–13 ,25 ,26
Delay in presenting at ‘appropriate’ health facility (phase 2)
In general, when mothers choose to seek care outside their homes, they may be constrained by difficulties with accessibility to health facilities and/or finances or identifying an ‘appropriate’ hospital that routinely admits and provides essential care for sick babies.13 ,25 It is, therefore, not uncommon for such mothers to present first to the nearest primary health centres/local private clinics most of which are ill-equipped to provide special care for neonates. As typified in one study from Egypt, the mothers of 109 (83.8%) of 130 severely jaundiced out-born infants admitted to the university children's hospital earlier sought medical attention at local clinics, during which only 28 infants had serum bilirubin ordered.13 At these clinics, 87 mothers (79.8%) were advised by doctors to ‘place the infant under neon light’ at home, 75 were advised to supplement breastfeeding with herbal infusions or formula milk and 15 infants were prescribed a variety of medications, including vitamins. In 22 cases, doctors immediately referred the infants to a hospital; despite that, parents of nine of these infants took no action until the babies became lethargic. At the time of hospital arrival, parents of 41 infants had already gone to 2–3 hospitals in search of available or affordable phototherapy with some travelling >5 h before locating the university hospital. Another study also found that over 25% of community health workers at primary care centres were likely to prescribe antibiotics, natural (direct sunlight) phototherapy or herbal therapies.29 Mothers in rural communities also consult traditional healers who prescribe various herbal preparations for treating jaundice.30
Delay in receiving appropriate and adequate care at ‘appropriate’ health facility (phase 3)
The lack of local practice guidelines for the management of jaundice and tools for real-time objective measurement/monitoring of bilirubin levels is common. These often prompt over-reliance by hospital personnel on visual assessment of the cephalocaudal progression or ominous signs of ABE/kernicterus particularly among out-born infants. Similarly, laboratory investigations to rule out possible risk factors like G6PD deficiency, ABO and Rhesus incompatibilities are not available routinely.6 ,31 Where such facilities are available, the turn-around time in obtaining results for prompt clinical decision is usually unhelpful. Many studies from India, Nigeria and Cameroun also exemplify the widespread problem of suboptimal phototherapy emissions well below therapeutic range in most secondary and tertiary hospitals in LMICs.32–34 The ideal first-line treatment with conventional blue-light phototherapy requires light emission spectrum within the bilirubin absorption spectrum of 400–520 nm (peak 450±20 nm); irradiance level ≥30 μW/cm2/nm, exposed to ∼80% of an infant's body surface area; and optimised duration of exposure.35 However, in one study from Nigeria, the majority (94%) of 63 phototherapy devices tested in 12 referral-level hospitals delivered irradiances of ≤10 μW/cm2/nm and none were ≥30 μW/cm2/nm.32 Many hospitals also have to contend with erratic power supply and frequent breakdowns due to poor device maintenance.11 Valuable time is, therefore, often lost exposing infants to prolonged ineffective phototherapy leading to exchange transfusion. Such system failures and late presentation account for high rates of avoidable exchange transfusion with its attendant risks and potential complications.11 ,12 ,36 Another important but less common cause of delay is occasional refusal by parents to accept clinically indicated exchange transfusion for their babies for religious reasons.11
Additionally, despite the high risk of neurodevelopmental impairments among infants treated for severe hyperbilirubinaemia, routine monitoring of affected infants for these long-term sequelae is rarely practiced in most LMICs.20 ,37 Established screening programmes for early detection of hearing deficits as well as other neurological deficits are uncommon for reasons of dearth of skilled personnel, paucity of appropriate equipment and poor awareness. The delay in the initiation of appropriate rehabilitative measures thus exacerbates the burden of severe hyperbilirubinaemia for the surviving infants and their families, especially in communities with unfavourable cultural disposition to child disability.
Improving the care of infants with or at risk of severe hyperbilirubinaemia
Addressing all the wide range of potential risk factors associated with severe hyperbilirubinaemia is unquestionably a daunting challenge for most LMICs already beleaguered with several fatal and communicable diseases. The main thrust of interventions to curtail the burden of neonatal jaundice must be twofold: first, to identify infants with the most prevalent and readily detectable risk factors and second, to eliminate, or reduce to the barest minimum, avoidable delays to effective recognition, timely detection, presentation and treatment of infants at risk of severe hyperbilirubinaemia at appropriate health facilities. Since mothers and other caregivers are often the first to come in contact with infants with jaundice, routine antenatal and predischarge counselling on avoidance of domestic haemolytic agents and the value of early recognition of jaundice should be actively promoted. This is especially important because recognition of illness is often defined by the patient's view/perception of reality which may be discordant with the health professional's medical criteria.23 Thus, it is important to foster closer collaboration between paediatricians and their obstetric and primary care colleagues for this purpose. Health education of expectant mothers must be complemented with the training and re-training of health workers on the principles and value of timely recognition, prevention and management of neonatal jaundice. Professionally led national initiatives on the control of severe neonatal jaundice similar to the existing ‘Helping Babies Breathe’ programme would be valuable in this respect.
The perceived benefits of traditional health providers cannot be dismissed outright, as some mothers may rely on testimonials of prior ‘success’ stories related possibly to physiological jaundice. Visual presentation of well-documented cases of mismanaged severe jaundice resulting in neonatal deaths or physical disability is a powerful educational tool to emphasise the potential dangers of recourse to inappropriate health facilities and the importance of timely appropriate treatment. Unfortunately, it is quite challenging for mothers to identify private clinics or primary care centres/hospitals adequately resourced to provide requisite treatment. It is, therefore, necessary to disseminate information about appropriate centres/hospitals for managing severe hyperbilirubinaemia in each locality. Provision of emergency ambulance services and community loan funds to address accessibility and financial constraints are also worth considering.25
Failure to offer appropriate treatment when infants are present at secondary/tertiary hospitals that routinely admit sick babies undermines the credibility of the entire health system and fosters future reluctance and significant delay in seeking help from these facilities. It also encourages recourse to unorthodox medicine. The need to provide health workers with the requisite training and tools for effective management of infants with or at risk for severe hyperbilirubinaemia cannot be overemphasised. The strategic goal in every hospital is to eliminate or curtail the need for exchange transfusion through timely and effective phototherapy. And when exchange transfusion is inevitable, it must be provided promptly and safely to prevent or treat ABE/kernicterus. The cost of providing intensive/special care for jaundiced newborns could be prohibitive and, perhaps, next only to that of caring for preterm babies in LMICs.38 ,39 The development of affordable phototherapy devices, as well as simple inexpensive adjustments to devices, such as hanging white curtains around units, changing bulbs periodically and optimising the distance between baby and lamps are effective in improving the quality of care and should be widely promoted.33 ,40
Common practice guidelines for neonatal jaundice do not support use of direct exposure to sunlight primarily due to safety concerns regarding potentially harmful infrared and ultraviolet rays and possible sunburn.9 ,41 ,42 But, mothers/caregivers with or without the support of health workers continue to expose their jaundiced babies to direct sunlight,27 ,28 even in developed countries.43–45 Following the successful piloting of filtered sunlight phototherapy for safety and efficacy, a clinical trial is currently ongoing to compare the effectiveness of this novel intervention with conventional blue-light phototherapy.46 This low-cost technology holds promise especially in tropical LMICs where the application of conventional phototherapy is constrained by costs and exogenous factors outside the control of the health system. Also promising is the emerging low-cost, minimally invasive, point-of-care tools for plasma/serum bilirubin monitoring.47 Pharmacotherapies, such as metalloporhyrins and clofibrate, also hold promise as potential low-cost treatments. However, the available evidence is still quite limited to justify their routine application presently. Crucially, developmental surveillance including objective hearing evaluation should be considered routinely for infants treated for severe hyperbilirubinaemia. Local adaptation of guidelines in the developed world,9 ,41 including WHO Handbook for Hospital Care,48 may serve as a possible take-off point for the development of relevant algorithms for the optimal management of severe hyperbilirubinaemia as exemplified in some LMICs.40 ,49 ,50 Overall, policy, public health and clinical leadership are urgently needed to comprehensively address the range of issues required to effectively curtail the burden of severe hyperbilirubinaemia and kernicterus in LMICs.
Conclusion and way forward
Severe hyperbilirubinaemia portends significant risks of avoidable mortality and severe long-term neurodevelopmental sequelae in LMICs. The burden is likely to be exacerbated by lack of poor or timely access to proven therapies that are taken for granted in the developed world. International collaborations are imperative for improved epidemiological data to address the inherent limitations in most of the available research and for the development of affordable and effective technologies for managing hyperbilirubinaemia. Each country must target efforts towards improved public and maternal/antenatal education on the potential dangers of severe neonatal jaundice, timely detection of high-risk infants, adequate resourcing of special care baby units in all referral-level hospitals, as well as the development and active promotion of pragmatic and contextually relevant clinical practice guidelines.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table
Footnotes
-
Acknowledgements We thank Jon F Watchko, Yvonne E Vaucher and Ashok K Deorari for valuable comments made on earlier drafts of this paper.
-
Contributors BOO conceptualised the paper and wrote the first draft with contributions from TAO and TMS. All authors participated in the literature search, selection and review; critically reviewed the manuscript for intellectual content and approved the submitted version.
-
Competing interests None.
-
Provenance and peer review Commissioned; internally peer reviewed.
-
Data sharing statement Human Development Report 2013, UNDP, New York, 2013; The State of the world's children 2013, UNICEF, New York, 2013.