Article Text

Abstract
Background A randomised, double-blind clinical trial was undertaken in order to assess the effectiveness of probiotics in the prevention of necrotising enterocolitis (NEC) in newborns weighing <1500 g.
Methods We studied a group of 150 patients who were randomised in two groups after parental consent was obtained, to receive either a daily feeding supplementation with a multispecies probiotic (Lactobacillus acidophilus, Lactobacillus rhamnosus, Lactobacillus casei, Lactobacillus plantarum, Bifidobacteruim infantis, Streptococcus thermophillus) 1 g per day plus their regular feedings or to receive their regular feedings with nothing added (control group), over the period of January 2007 through June 2010. Clinicians in care of the infants were blinded to the group assignment.
Results The primary outcome was the development of NEC. Both groups were comparable, with no differences during hospitalisation, including the type of nutrition received. Blood cultures obtained from cases that developed sepsis did not reveal lactobacillus or Bifidobacteria growth. No differences were detected in terms of NEC risk reduction (RR: 0.54, 95% CI 0.21 to 1.39) although we did observe a clear trend in the reduction of NEC frequency in the studied cases: 6 (8%) versus 12 (16%) in the control group. When the combined risk of NEC or death was calculated as a post hoc analysis, we found a significantly lower risk (RR: 0.39, 95% CI 0.17 to 0.87) for the study group.
Conclusions Probiotics may offer potential benefits for premature infants and are a promising strategy in the reduction of the risk of NEC in preterm newborns.
Statistics from Altmetric.com
What is already known on this topic
-
Recent randomised trials reports that enterally administered probiotics substantially reduce the risk of necrotising enterocolitis (NEC) and death in preterm newborns <1500 g
-
There is a trend towards improved results in trials using more than one strain as probiotic prophylaxis
-
Bifidobacterium spp. and Lactobacillus acidophilus, have been associated with reports of a reduced incidence of NEC (0.29, 95% CI 0.15 to 0.56) and mortality (0.31, 95% CI 0.17 to 0.57)
What this study adds
-
We employed a multispecies probiotic (six types) without adverse effects being reported
-
This is the first clinical trial evaluating the use of a multispecies probiotic in the reduction of NEC risk in preterm newborns <1500 g in Mexico
Introduction
Necrotising enterocolitis (NEC) is the most commonly acquired intra-abdominal emergency among preterm newborns, with an inverse relationship between gestational age/weight and the risk of NEC.1 ,2 The incidence of NEC in our institution among preterm newborns <1500 g is 12%, with a 1.5% death rate,3 which is a high incidence according to a recent meta-analysis which classified NEC incidence as being high when reports exceed 7%.4 A recent report from the US National Institute of Child Health and Human Development reported an incidence ranging from 2% to 19% in infants weighing 501–750 g, and from 2% to 25% in infants between 1001 and 1500 g.5
At birth, the neonatal intestinal tract is virtually sterile but it becomes colonised quickly afterwards with a variety of bacterial species, sometimes vertically acquired. In an attempt to maintain a balance, the body gives ‘preference’ to a variety of ‘favourable’ gram-positive microorganisms, such as Lactobacilli and Bifidobacteria. In contrast, preterm newborn bowel is likely to be colonised by different microorganisms, predominantly coliforms. The combination of an increase in pathogenic bacteria with a decrease in ‘normal flora’ is one of the factors that render these infants being at increased risk of developing NEC, although there is no single microorganism, virus or fungus implicated as the sole factor in the pathogenesis of NEC.6 Recently, interest on the use of probiotics has grown, as clinical evidence supports their use and benefits in many intestinal and extraintestinal sites. There is a wide variety of types of probiotics according to the methods used for their isolation, their microbiological and physiological characteristics, their uses and the doses required in order to obtain such effects.7,–,9 Lactobacillus acidophilus and Bifidobacterium infantis have been used as probiotics to reduce incidence or NEC, but the dosage, duration, safety and efficacy of probiotics remain controversial.10 A recent systematic review of randomised clinical trials (RCTs) indicates that the trials reporting a significant decline in NEC used multistrain products, whereas those reporting a lesser decline used a single organism.11
The Instituto Nacional de Perinatología is a tertiary-level hospital, where 252–300 preterm infants born <1500 g are attended each year. A double-blind, randomised clinical trial was undertaken in order to assess the use of a multispecies probiotic in the reduction of NEC risk in preterm newborns <1500 g admitted at the intensive and intermediate care units.
Methods
Enrolment
Preterm newborns <1500 g from a tertiary-care hospital who were admitted to the intermediate or intensive care units from January 2007 to June 2010, were recruited on the day they were starting enteral feedings according to their attending physicians decision. This could be started with their own' s mother milk when available or preterm formula. Preterm newborns weighing <1500 g with a low Apgar score (<6 at 5 min), gastrointestinal malformations, genetic syndromes, asphyxia and IA–IB NEC stages according to Bell's classification were excluded from the trial. Intervention was stopped when the clinical condition precluded enteral intake and restarted as soon as the patient was able to accept enteral intake. The study protocol was approved by our Ethics Institutional Review Board and informed consent was obtained from the children's parents.
Randomisation and allocation concealment
Infants were prospectively and randomly assigned to one of two groups using a random digit table, which was handled by the Human Milk Bank staff that was not involved in the care of the patients and adhered to proper trial procedures. Once they assigned them to the interventions, the study group received their regular feeds and a daily multispecies probiotic feeding supplement of 1 g per day diluted in 3 ml of expressed mother's milk when available or a premature infant formula when expressed breast milk was unavailable. The control group received their regular feeds from their mother's own milk when available with nothing added, or a premature infant formula. As allocation concealment measure, the study group received a suspension that matched the physical appearance of milk and the bottles were labelled only with the patient's name and identification number as usual. At feeding time, the staff nurse assigned to any infant on the study would administer the feeds as regular feedings. Attending physicians and nurses caring for the infants were blinded to the group assignments.
Product preparation
Fresh supplement suspensions were individually prepared by the Human Milk Bank staff that was not directly involved in routine patient care. The multispecies probiotic powder contained L acidophilus 1.0×109 colony forming units (CFU) CFU/g, Lactobacillus rhamnosus 4.4×108 CFU/g, Lactobacillus casei 1.0×109 CFU/g, Lactobacillus plantarum 1.76×108 CFU/g, Bifidobacteruim infantis 2.76×107 CFU/g, Streptococcus thermophillus 6.6×105 CFU/g, each pack (Laboratorio Italmex SA, Mexico City, Mexico).We looked for the commercially available product in Mexico that best reached bacterial concentration as suggested by Timmerman HM, et al.12 We kept multispecies probiotic powder at room temperature. Quality control registers were available from the producer anytime. We checked them twice during the study period. This multispecies probiotic powder is registered by the Ministry of Health in Mexico: 107M96 y 106M96.
Follow-up
The amount of feeding was increased slowly if tolerated, according to the Institution's Protocol for Enteral Feeds13 and the feeding was stopped if there was any sign of feeding intolerance, such as gastric residuals, abdominal distension, diarrhoea or vomiting, which were evaluated and recorded daily. Infants received parenteral nutrition until 100 ml/kg/day could be supplied by the enteral route. As primary outcome, we recorded the occurrence of NEC according to Bell's modified classification14 from stage IIA to IIIB. As secondary outcomes, we registered major neonatal morbidities such as sepsis diagnosed in infants with clinical signs occurring after randomisation and proven by positive blood culture; apnoea, defined as the cessation of respiration for >20 s or cessation of respiration of any duration accompanied by bradycardia (HR <100/min) and/or cyanosis; small for gestational age (SGA) defined as weight below the 10th percentile for gestational age; anaemia, defined as Hb<10 g/dl or haematocrit <30%; patent ductus arteriosus (PDA), defined as a connection between the aorta and the pulmonary artery with left to right shunt; and death.
Blood cultures were taken in case of signs of sepsis or ≥2 stage NEC using BactAlert 3D (bioMerieux, Paris, France) paediatric bottles and bacterial identification was performed using Vitek 2 (bioMereiux, France) with gram-positive, negative and anaerobes cards.
Sample size and analysis
Based on an estimated reduction in the incidence of NEC in a previous study15 of 20% in subjects without treatment and 5% with treatment, we used a proportion difference with a power of 0.80 and an α of 0.05, and we calculated a sample size of 72 patients for each group with a single-sized test.
Continuous variables were compared by using Student's t test and Mann–Whitney test for distribution-free quantitative variables; χ2 analysis was used to ascertain significant differences in categorical variables between groups. Significance was defined at p<0.05 and we used two-sided significances. RRs and 95% CIs were used to compare additional risk reduction in probiotic-treated newborns developing NEC with control subjects. Primary outcome was the incidence of NEC. Secondary outcomes were major neonatal morbidities and mortality. The combined risk of NEC or death was calculated as a post hoc analysis.
Results
A total of 168 patients were eligible, but 18 sets of parents did not give their informed written consent, thus, we randomised 75 babies to the study group and 75 to the control group (figure 1).
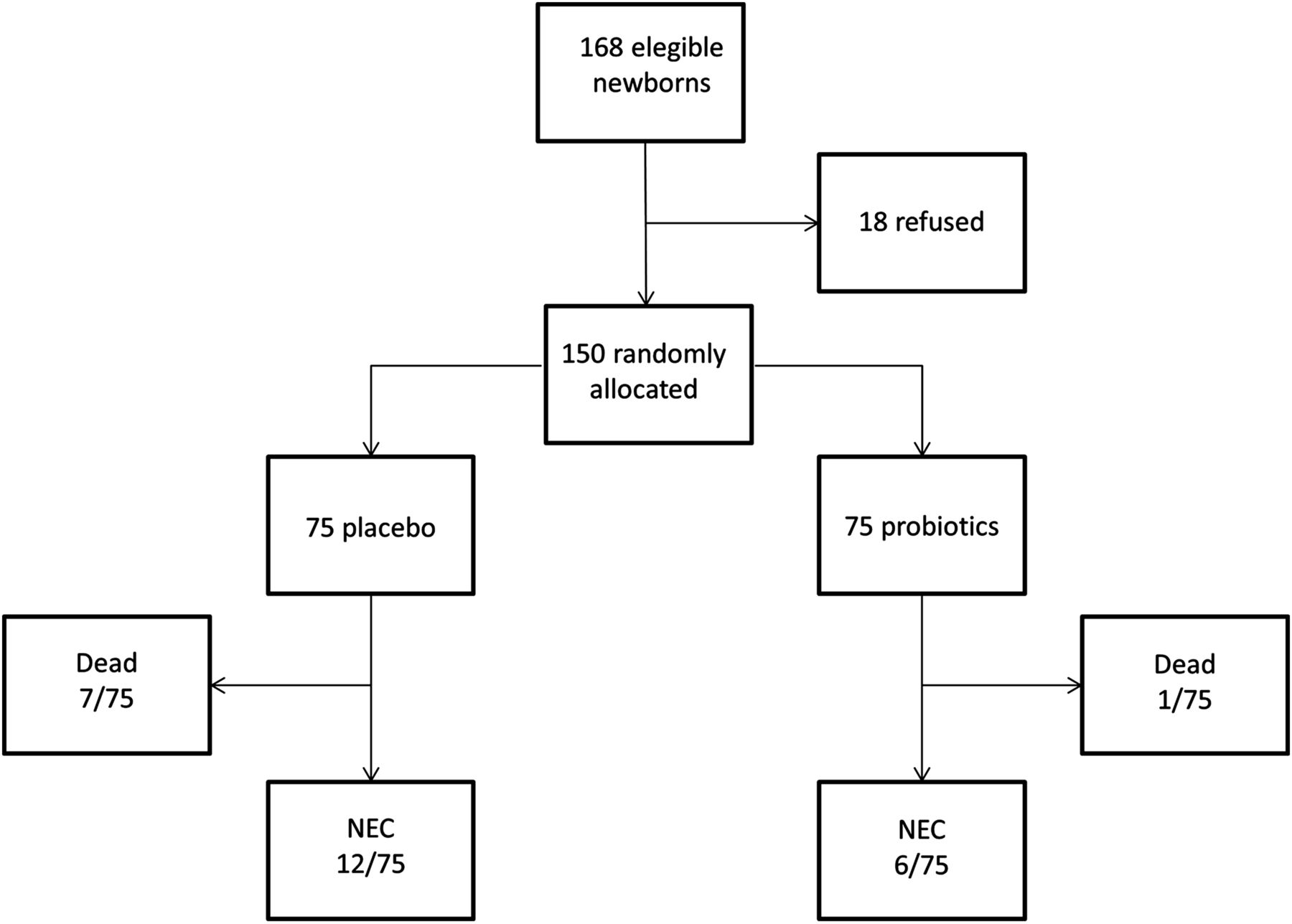
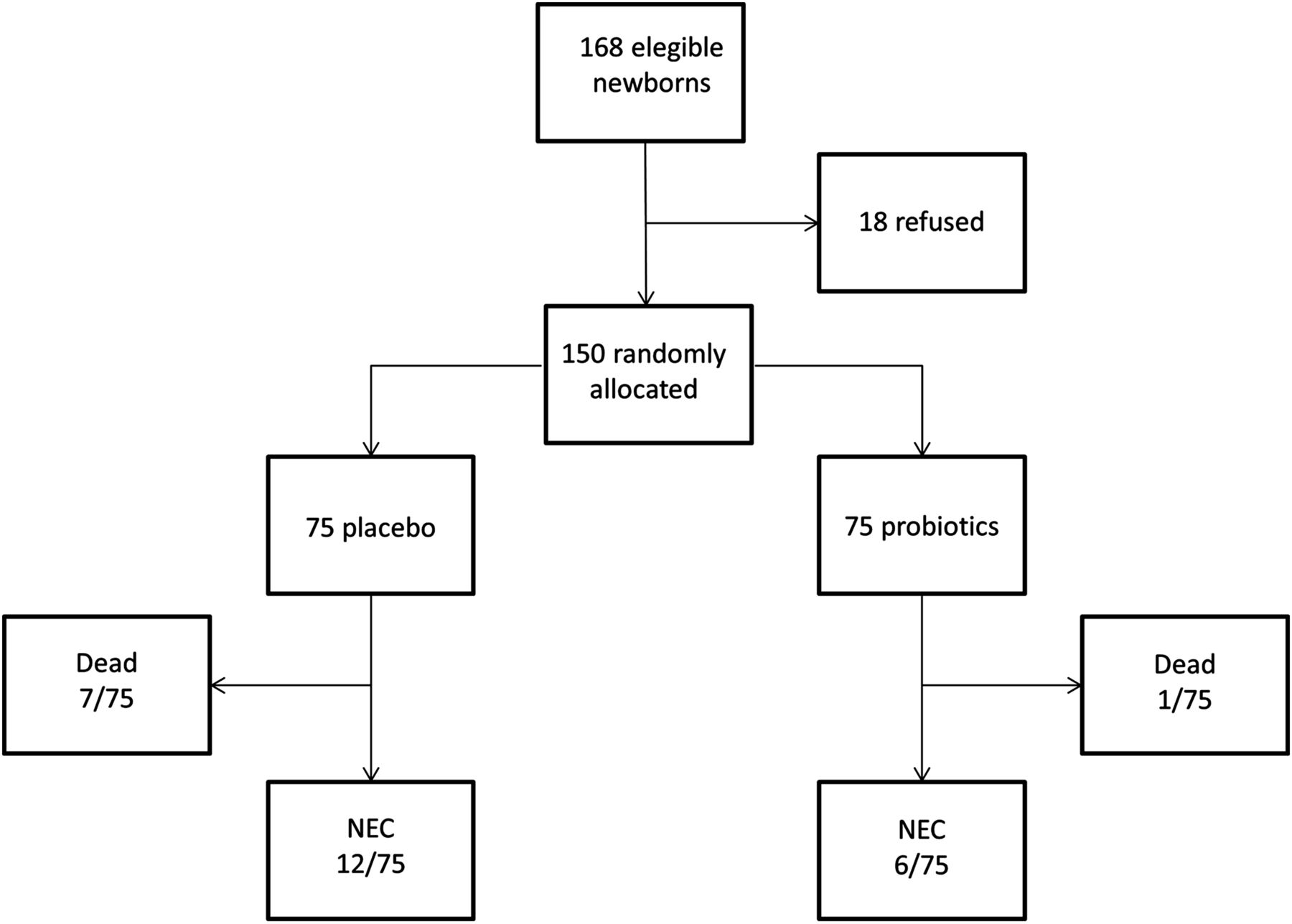{kind=link}
Trial profile.
Major maternal morbidities are described in table 1, showing no differences between the two groups.
Major maternal morbidities between groups
As for neonatal characteristics and type of management during hospitalisation, we did not find any differences. Prenatal steroids were used in 66.7% of the cases and 70.7% of the controls in our population. Regarding the type of feedings, 21.3% in the study group and 14.7% in the control group received exclusively human milk, without statistically significant differences. The vast majority of subjects (57.3% in the study group and 69.3% in the control group) received mixed formula (defined as 50% mother's milk, 50% premature formula) and a lower proportion received less than 50% of human milk from their mothers, with no differences observed between the two groups (table 2). We did not find differences in the incidence of any signs of feeding intolerance, such as diarrhoea, abdominal distension or vomiting between groups. Blood cultures obtained in the cases of sepsis or NEC did not show any Lactobacillus or Bifidobacteria growth.
Clinical characteristics, type of feeding and management of study infants
There were no differences in major neonatal morbidities. The vast majority of our population was SGA: 78.7% of the cases versus 77.3% of the controls. Apnoea was reported in 33.3% for the cases and 24% for the controls, PDA in 17.3% of the cases versus 12% of controls, anaemia in 13.3% of cases and 9.3% of controls and sepsis in 56% of the cases versus 58.7% of the control group, without statistically significant differences in any of them.
No difference was found in the reduction of NEC risk in the study group. We analysed the risk of developing NEC between the two groups and observed a lower proportion of NEC (8%) in the study group than in the control group (16%), but the difference was not statistically significant. We did not find a significant difference in mortality in the study group: 1 (1.3%) case in the probiotic group who died from sepsis versus 7 (9.3%) in the control group who died during the study period (four deaths were attributed to sepsis and the others were due to cardiac anomalies, bronchoaspiration and hydrocephalus, respectively; p<0.063). In addition, we also estimated the risk of mortality between the two groups and we could not find any difference: 0.14 (95% CI 0.01 to 1.13).
When the combined risk of mortality or NEC was analysed, we found that fewer infants in the probiotic group died or developed NEC compared with the control group, with a RR 0.39 (95% CI 0.17 to 0.87) (table 3).
Outcome variables after oral probiotics: combined risk of NEC and mortality for both groups
Discussion
NEC is related with greater morbidity and mortality in low birthweight preterm infants; probiotics may protect against NEC by shifting intestinal microflora from a potentially harmful environment to one that would be predominantly beneficial to the host.4,–,7
We analysed major maternal morbidities and we did not find any differences. Although many variables are associated with the development of NEC, only prematurity and low birth weight has been consistently identified in case-controlled studies. In this study, there was a high incidence of SGA patients in both groups and perhaps this could be one of the reasons for our high incidence of NEC, since our institution receives only high-risk pregnancies.2 ,3 Certain risk factors known to be associated with an increased risk of NEC, such as the need of mechanical ventilator support, exposure both to glucocorticoids and indomethacin during the first week of life, and a low Apgar score, among others, showed no differences in both groups.16
Regarding antenatal steroids exposure, Bauer et al17 noted a significant decrease in the incidence of NEC in infants who received antenatal steroids. However, Guthrie et al16 noted that the exposure to antenatal glucocorticoids was associated with an increased risk of NEC, explained by the increased survival of more immature infants. However, we failed to find such a difference in our population, even though a great proportion in both groups received them.
As for the type of feedings, human milk is a recognised factor for reducing the risk of NEC;18 ,19 in this study, we had a higher proportion of total human milk fed infants in the study group (21.3%) versus the control group (14.7%), but the difference was not statistically significant. More than half of the babies who participated in the study received mixed formula feeds. There is evidence of a 10-fold risk of NEC in preterm newborns fed with formula,19 although we could not find such a difference because, even in the case of the mixed formula (50% human milk, 50% formula) and in those who received less than 50% of human milk, the majority received at least some human milk, which contains oligosaccharides which may have had a protective effect in both groups.20
NEC incidence in the study group was 8% versus 16% in the control group, although the difference was not statistically significant (p=0.132). Some authors21,–,23 have reported a lower incidence of NEC or death in groups treated with probiotics; we did not find a statistical difference in the death rate between both groups (p<0.063), but when the combined incidence of NEC and/or mortality was compared, significantly more infants in the control group died or developed IIA–IIIB NEC stages compared with the study group, with a risk reduction for the study group: RR 0.39 (95% CI 0.17 to 0.87). Lin et al recommend combining both indicators, since death precludes the subsequent development of NEC.24
Recent systematic reviews of RCT on the use of probiotics for the prevention of NEC underline the significant effects of probiotics supplements in reducing death by any cause and disease in preterm neonates. The dramatic effect sizes, as well as overall evidence, indicate that additional placebo-controlled trials are unnecessary if suitable probiotics are available.25,–,30
Millar et al31 consider probiotics different from conventional drugs, with optimum production, transport, dosage and contraindications being unclear. There are other theoretical concerns that probiotics could enhance the transfer of antibiotic-resistant genes. However, any adverse effects associated with this possibility are likely to be outweighed by the substantial reduction in mortality and NEC.
Szajewska,32 in another systematic review, recognises probiotics as a useful tool in the prevention of NEC, but shows that there is still a lack of information on which products should be administered, at what dose and for how long they are required.
In a recent meta-analysis by Guthmann F et al,5 they report a relevant reduction of NEC incidence and mortality with the prophylactic administration of probiotics (p<0.00001), displaying a wide range of NEC incidences. They concluded that prophylactic probiotics appear to be safe and effective in reducing the rates of NEC by approximately 70% and mortality by approximately 50% in preterm infants <1500 g.
Although we were not able to find a reduction in the risk of NEC in preterm neonates fed with milk supplemented with probiotics, we did find that half the cases of NEC occurred in the study group with probiotics versus the control group without them. When the combined risk of mortality and NEC was analysed, we found a difference in favour of the use of probiotics.
Acknowledgments
The authors thank the nursing staff of the Instituto Nacional de Perinatología for their invaluable help in this research.
References
Footnotes
-
Competing interests None.
-
Ethics approval This study was conducted with the approval of the Instituto Nacional de Perinatología Investigation Comitee with the registration number 10231.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Fantoms