Article Text

Abstract
Objective To evaluate enteral feeding practices in neonatal units in different countries and on different continents.
Design A web-based survey of 127 tertiary neonatal intensive care units in Australia, Canada, Denmark, Ireland, New Zealand, Norway, Sweden and the UK.
Results 124 units (98%) responded. 59 units (48%) had a breast milk bank or access to donor human milk (Australia/New Zealand 2/27, Canada 6/29, Scandinavia 20/20 and UK/Ireland 31/48). The proportion of units initiating enteral feeding within the first 24 h of life was: 43/124 (35%) if gestational age (GA) <25 weeks, 53/124 (43%) if GA 25–27 weeks and 88/124 (71%) if GA 28–31 weeks. In general, Scandinavian units introduced enteral feeds the earliest, followed by UK/Ireland. Continuous feeding was routinely used for infants below 28 weeks' gestation in almost half of the Scandinavian units and in approximately one sixth of units in UK/Ireland, but rarely in Australia/New Zealand and Canada. Minimal enteral feeding for 4–5 days was common in Canada, but rare in Scandinavia. Target enteral feeding volume in a ‘stable’ preterm infant was 140–160 ml/kg/day in most Canadian units and 161–180 ml/kg/day or higher in units in the other regions. There were also marked regional differences in criteria for use and timing when human milk fortifier was added.
Conclusions This study highlights areas of uncertainty and demonstrates marked variability in feeding practices. It provides valuable data for planning collaborative feeding trials to optimise outcome in preterm infants.
Statistics from Altmetric.com
Introduction
Optimising the nutritional status of very preterm infants is of critical importance, but enteral feeding in this patient population remains challenging.1 Difficulties interpreting signs of feed intolerance and the perceived risk of necrotising enterocolitis (NEC) are common reasons for delaying the introduction and advancement of enteral feeds.2,–,4 This needs to be balanced against the risks and costs associated with prolonged duration of central lines, parenteral nutrition and gut disuse.5 Preterm infants have increased nutritional demands due to inadequate stores and rapid growth, but extrauterine growth restriction is common and may impair long-term growth and neurodevelopmental outcome.6 7
Human milk is recommended when initiating enteral feeds.8 Mother's own freshly expressed preterm milk has a relatively high protein and fat content and preserved anti-infective properties. Donor human milk (DHM) is an alternative option if mother's own milk is not available. If there is no access to human milk, cow's milk-based artificial formulas are used.9
What is already known on this topic
▶ Nutritional management in preterm infants affects key morbidities in the short (eg, sepsis), medium (eg, growth) and long term (eg, cognition).
▶ Barriers to the early introduction and advancement of enteral nutrition in very preterm infants include feed intolerance and the perceived risk of necrotising enterocolitis.
What this study adds
▶ This study demonstrates marked variability in neonatal feeding practices in four geographical regions.
▶ This variability is partly explained by differences in access to donor human milk.
▶ Variations in feeding practices also reflect a lack of evidence and thus a need for large scale collaborative studies.
Limited evidence to guide feeding strategies in preterm infants has led to a lack of consensus. Many systematic reviews include small numbers of infants in patient populations different to those considered high risk today.10,–,12 Some recent randomised controlled trials (RCTs) also have limited generalisability in units where practice falls outside the RCT study protocols.13,–,15
Enteral feeding practices for preterm infants have been previously surveyed,16,–,18 but practices between countries have not been compared. The objective of this survey was to evaluate and compare the clinical practices of enteral feeding in very preterm infants among neonatal units in four different geographical regions. This may inform the design of large, international multicentre RCTs.
Methods
Between March and May 2010, a web-based survey was sent by email to one senior consultant in all tertiary neonatal units in Australia (21), New Zealand (6), Canada (30), Denmark (3), Norway (9), Sweden (8), Ireland (8) and to 42 in the UK. The questionnaire, consisting of multiple-choice and open-ended questions, requested information about the demographics of the unit, presence of a milk bank or access to DHM, human milk analysis, initiation and advancement of enteral feeds, indications for and use of human milk fortifier (HMF), supplementation with oral vitamins and postdischarge feeding (see online supplementary appendix). Follow-up for non-responders was by email and telephone. A second consultant in the unit was approached if necessary.
Data analysis
Data were analysed using SPSS (v 16.0) statistical software. Descriptive results are expressed as numbers and proportions (%). When comparing feeding practices between the four different regions, a one-way analysis of variance was used with Bonferroni post hoc comparison. A p value <0.05 was considered significant.
Results
One hundred and twenty-four of 127 units (98%) responded; one Irish, one UK and one Canadian unit did not respond. The proportions of large units (>10 intensive care cots) were: Canada 23/29 (79%), Australia/New Zealand 18/27 (67%), UK/Ireland 22/48 (46%) and Scandinavia 7/20 (35%). All units in Scandinavia and approximately two thirds of units in UK/Ireland had access to DHM, which was less common in Canada and Australia/New Zealand (table 1). All Swedish units routinely analysed the protein and fat content in human milk, but outside Sweden only one unit in Denmark and one in Australia routinely used a human milk analyser.
Enteral nutrition strategies for very preterm infants in four geographical regions
Table 1 describes when enteral feeding is started, advanced and mode of feeding (bolus vs continuous), with marked differences between the four regions. In general, Scandinavia introduced enteral feeds the earliest, followed by UK/Ireland (figure 1). There were also marked differences in clinical indications for delaying the introduction of enteral feeds (table 2). Continuous feeding was routinely used for infants below 28 weeks' gestation in almost half of the Scandinavian units and in approximately one sixth of units in UK/Ireland, but rarely in Australia/New Zealand and Canada. In contrast, minimal enteral feeding was common in Canada but rare in Scandinavia. Target enteral feeding volume in ‘stable’ preterm infants was 140–160 ml/kg/day in most Canadian units and 161–180 ml/kg/day or higher in the other regions (table 1).

(A–C) Timing of start of enteral feeding depending on gestational age (GA)/birth weight (BW).
Specific clinical situations where units would usually delay onset of enteral feeding
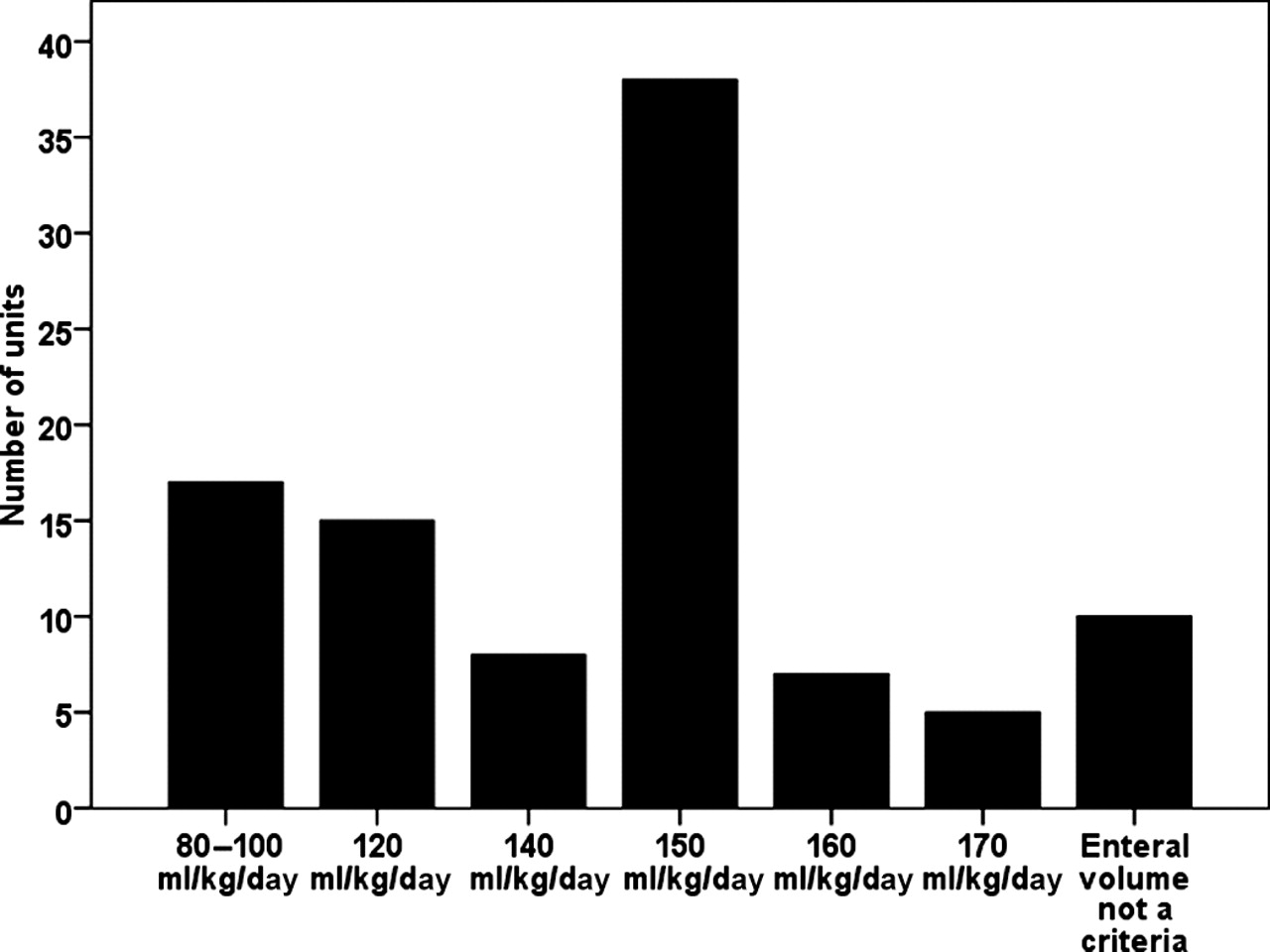
Differences in the use of HMF were not as large as with feeding strategies (table 3). Fifteen of 48 UK/Ireland units only added HMF to human milk when the infant ‘needed it’, for instance because of poor weight gain or low urea values. However, there was a large variation in the required enteral volume tolerated (ml/kg/day) before adding HMF (figure 2). In Canada approximately two thirds of the units added HMF when an enteral volume of 80–140 ml/kg/day was tolerated. In UK/Ireland approximately four fifths of the units added HMF only when an enteral volume ≥150 ml/kg/day was tolerated. In contrast, in UK/Ireland approximately two thirds of the units started with full strength HMF, whereas in Canada approximately two thirds of units commenced half strength HMF or less. Approximately two thirds of the units routinely using HMF provided additional vitamin supplementation even though most multi-component HMF products contain supplemental vitamins.

{kind=link}
{kind=link}
Enteral volume tolerated before adding human milk fortifier (HMF) to human breast milk.
Human milk fortification (HMF) practices in preterm infants
Most units did not recommend protein or fat supplements after discharge to infants who were receiving breast milk exclusively at discharge (table 4). In Canada and UK/Ireland, specific postdischarge formulas were frequently recommended in infants who were not breast fed at discharge. ‘Standard’ term infant formula was more commonly used in Australia/New Zealand and Scandinavia.
Postdischarge enteral nutrition practices
Discussion
This survey demonstrates large differences in feeding practices for preterm infants in four separate geographical regions. Access to DHM may be an important factor. Differences in feeding intervals, target volumes, vitamin supplementation and the use of HMF seem to reflect the lack of clear evidence.
Many mothers of preterm infants struggle to initiate lactation.19 Most units with access to DHM commenced enteral feeding on the first day of life, even in the most immature infants, and advanced more rapidly than units without access to DHM. Units without access to DHM frequently delayed the introduction of enteral feeds until mother's own milk was available. Our survey shows a low use of DHM for preterm infants in Canada and only two units in Australia/New Zealand had access to DHM, in contrast to Scandinavia, where all surveyed units had access to DHM.
Systematic reviews assessing timing of the introduction and advancement of enteral feeds in preterm infants have shown neither clear benefits nor obvious harm with any strategies.10 11 Units included in two recent RCTs assessing prolonged minimal enteral feeding13 15 commenced enteral feeding much later (median 9 days of life)13 than units responding to our survey, or achieved full feeds very late (median 32 days of life).15 Large cohort studies of extremely low birthweight (ELBW) infants exclusively fed human milk indicate that early introduction and rapid advancement of feeds are not associated with high rates of NEC,20,–,22 and that it is possible to establish full enteral feeds by the third week of life in the majority of ELBW infants.23 In contrast, delayed enteral feeding and reduced use of human milk are associated with increased late onset sepsis and NEC.9 23 24
Differences in feeding mode may reflect Scandinavian studies that suggested possible benefits from continuous feeding.25 26 In contrast, a systematic review suggested that infants fed by continuous feeding took longer to reach full feeds.27 However, all studies comparing feeding mode are small and evidence of benefit for a particular feeding mode is limited.
Rapidly growing preterm infants have high protein and energy requirements. Recent European guidelines recommend enteral protein intakes of 4.0–4.5 g/kg/day for infants less than 1000 g and 3.5–4.0 g/kg/day for infants from 1000 to 1800 g.6 After the first 3–4 weeks, the protein content of expressed breast milk is ∼1.1–1.3 g/100 ml. Commercial HMF increases protein content by 0.8–1.0 g/100 ml,28 meaning that an enteral volume of 180 (160–200) ml/kg/day is required to approach a protein intake of 4.0 g/kg/day.29 Most units in this survey aimed for similar target volumes, although some Canadian units had lower target volumes. While fortification can be individualised to improve protein intake and growth when volumes are 150–160 ml/kg/day,30 increasing the daily enteral volume to 180 ml/kg/day29 31 may be a simpler way to achieve the same goal.
Adding HMF to human milk increases its osmolality and may delay gastric emptying.32 Some clinicians believe that HMF increases feed intolerance, which may explain why some units delay its introduction. However, feed intolerance is a poorly defined symptom in preterm infants2 and has no clear relationship with NEC. Clinically, significant gastrointestinal adverse effects are not more common in preterm infants receiving HMF.33 A recent study reported that human milk-based HMF reduced the risk of NEC.14 Caution is needed when interpreting this study, as the incidence of NEC was very high (15%) in the control group and the incidence of NEC in the human-milk based HMF group was similar to reports from units using cow's-milk based HMF.20,–,22
Optimal nutritional management of preterm infants after discharge is a dilemma. Poor growth is associated with worse cognitive outcome,34 but feeding breast milk after discharge has beneficial effects on cognition and longer term health.35 Postdischarge formula was widely used in Canada and UK/Ireland, despite no evidence of benefit.36
Our survey asked specifically for the ‘policy of the unit’. However, as a single neonatologist responded, personal bias cannot be excluded. Our survey does not describe actual enteral nutrition received, so some caution is needed when comparing our results with studies that have reported specific intakes. The strength of this study is the high response rate from four distinct geographical regions. We believe the responses reflect true differences in enteral feeding strategies and that this survey gives an updated overview of the breadth of enteral nutrition practices in developed countries in 2010.
Conclusion
This study highlights enormous variability in neonatal feeding practice in four different geographical regions reflecting both lack of evidence and strong local traditions. There is a need for evidence-based enteral feeding strategies that optimise enteral nutrition (both in hospital and after discharge) while minimising the risk of NEC. Future multicentre trials comparing different feeding practices should be sufficiently powered to examine important long term (growth and development) as well as more immediate outcomes (eg, death, NEC and nosocomial infection).
Acknowledgments
The authors thank the neonatal units in the following hospitals and centres for providing data for this survey.
In Australia Royal Darwin Hospital, Darwin; The Townsville Hospital, Townsville; Mater Mothers' Hospital, Brisbane; Royal Brisbane and Women's Hospital, Brisbane; John Hunter Children's Hospital, Newcastle; Royal Prince Alfred Hospital, Sydney; Liverpool Hospital, Liverpool; Nepean Hospital, Sydney; Royal Hospital for Women, Sydney; Royal North Shore Hospital, Sydney; Westmead Hospital, Sydney; The Children's Hospital at Westmead, Sydney; The Canberra Hospital, Canberra; Mercy Hospital for Women, Melbourne; Monash Medical Centre, Melbourne; The Royal Women's Hospital, Melbourne; Royal Children's Hospital, Melbourne; Royal Hobart Hospital, Hobart; Flinders Medical Centre, Adelaide; Women's and Children's Hospital, Adelaide; King Edward Memorial Hospital for Women and Princess Margaret Hospital for Children, Perth.
In Canada Children's Hospital of Eastern Ontario, Ottawa; The Ottawa Hospital, Ottawa; IWK Health Centre, Halifax; Children's Women's Health Centre of BC, Vancouver; BC Children's Hospital, Vancouver; Foothills Medical Centre, Calgary; Royal Alexandra Hospital, Edmonton; Janeway Children's Health & Rehabilitation Centre, St. John's; Kingston General Hospital, Kingston; McMaster Children's Hospital, Hamilton; Royal Columbian Hospital, New Westminster; St. Boniface General Hospital, Winnipeg; St. Joseph's Health Care, London; Sunnybrook & Women's College Health Sciences Centre, Toronto; The Moncton Hospital, Moncton; University of Manitoba Health Sciences Centre, Winnipeg; Victoria General Hospital, Victoria; Hospital for Sick Children, Toronto; Mount Sinai Hospital, Toronto; Universite de Montreal Hospital Sainte-Justine, Montreal; Centre Hospitalier Universitaire de Quebec, Quebec City; Jewish General Hospital, Montreal; Royal Victoria Hospital, McGill University Health Centre, Montreal; Centre Hospitalier Universitaire de Sherbrooke, Sherbrooke; Royal University Hospital, Saskatoon; Regina General Hospital, Regina; Dr. Everett Chalmers Regional Hospital, Fredericton; Cape Breton Regional Hospital, Sydney; Surrey Memorial Hospital (Level 2), Surrey.
In Denmark Odense University Hospital, Odense; Rigshospitalet, Copenhagen; Århus University Hospital, Århus.
In New Zealand National Women's Health, Auckland; Middlemore Hospital, Auckland; Waikato Hospital, Hamilton; Wellington Regional Hospital, Wellington; Christchurch Women's Hospital, Christchurch; Dunedin Hospital, Dunedin.
In Ireland The Rotunda Hospital, Dublin; National Maternity Hospital, Dublin; Coombe Women's Hospital, Dublin; Cork University Maternity Hospital, Cork; Our Lady of Lourdes Hospital, Drogheda; St. Munchin's Regional Maternity Hospital, Limerick; University College Hospital, Galway.
In Norway Oslo University Hospital-Rikshospitalet, Oslo; Oslo University Hospital-Ullevål, Oslo; Akershus University Hospital, Lørenskog; Stavanger University Hospital, Stavanger; Haukeland University Hospital, Bergen; Health Sunnmøre Trust, Ålesund; St. Olav University Hospital, Trondheim; Nordland Central Hospital, Bodø; University Hospital of North Norway, Tromsø.
In Sweden Örebro University Hospital, Örebro; Karolinska University Hospital-Astrid Lindgren Solna, Stockholm; Karolinska University Hospital-Huddinge, Stockholm; Sahlgrenska University Hospital, Gothenburg; Linköping University Hospital, Linköping; Norrland University Hospital, Umeå; Uppsala University Hospital, Uppsala; Lund University Hospital, Lund.
In the UK Aberdeen Maternity Hospital, Aberdeen; Royal Infirmary of Edinburgh, Edinburgh; Royal Hospital for Sick Children, Glasgow; Royal Victoria Infirmary, Newcastle upon Tyne; Leeds General Infirmary, Leeds; Addenbrooke's Hospital, Cambridge; Birmingham Heartlands Hospital, Birmingham; Birmingham Women's Hospital, Birmingham; Chelsea & Westminster Hospital, London; Derriford Hospital, Plymouth; University College London Hospital, London; Homerton University Hospital, London; James Cook University Hospital, Middlesbrough; Southampton General Hospital, Southampton; John Radcliffe Hospital, Oxford; Leicester Royal Infirmary, Leicester; Norfolk and Norwich University Hospital, Norwich; Queen's Medical Centre, Nottingham; Nottingham City Hospital, Nottingham; Peterborough District Hospital, Peterborough; Queen Alexandra Hospital, Portsmouth; Royal Hallamshire Hospital, Sheffield; Royal Shrewsbury Hospital, Shrewsbury; Southmead Hospital, Bristol; St George's Hospital, London; St Mary's Hospital, Manchester; St Michael's Hospital, Bristol; Bradford Royal Infirmary, Bradford; Women and Children's Hospital, Hull; Liverpool Women's Hospital, Liverpool; Royal Preston Hospital, Preston; University Hospital of North Tees, Stockton; William Harvey Hospital, Kent; York Hospital, York; Forth Park Hospital, Kirkcaldy; Royal Maternity Hospital, Belfast; City Hospitals Sunderland, Sunderland; King's College Hospital, London; St Peter's Hospital, Chertsey; Queen Charlottes and Chelsea Hospital, London; Royal London Hospital, London.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.