Article Text

Abstract
Objective To conduct a comprehensive global systematic review and meta-analysis on the association between Helicobacter pylori infection and IBD. As bacterial antigen cross-reactivity has been postulated to be involved in this association, published data on enterohepatic Helicobacter spp (EHS) and Campylobacter spp and IBD was also analysed.
Design Electronic databases were searched up to July 2015 for all case-control studies on H. pylori infection/EHS/Campylobacter spp and IBD. Pooled ORs (P-OR) and 95% CIs were obtained using the random effects model. Heterogeneity, sensitivity and stratified analyses were performed.
Results Analyses comprising patients with Crohn's disease (CD), UC and IBD unclassified (IBDU), showed a consistent negative association between gastric H. pylori infection and IBD (P-OR: 0.43, p value <1e-10). This association appears to be stronger in patients with CD (P-OR: 0.38, p value <1e-10) and IBDU (P-OR: 0.43, p value=0.008) than UC (P-OR: 0.53, p value <1e-10). Stratification by age, ethnicity and medications showed significant results. In contrast to gastric H. pylori, non H. pylori-EHS (P-OR: 2.62, p value=0.001) and Campylobacter spp, in particular C. concisus (P-OR: 3.76, p value=0.006) and C. showae (P-OR: 2.39, p value=0.027), increase IBD risk.
Conclusions H. pylori infection is negatively associated with IBD regardless of ethnicity, age, H. pylori detection methods and previous use of aminosalicylates and corticosteroids. Antibiotics influenced the magnitude of this association. Closely related bacteria including EHS and Campylobacter spp increase the risk of IBD. These results infer that H. pylori might exert an immunomodulatory effect in IBD.
- INFLAMMATORY BOWEL DISEASE
- HELICOBACTER PYLORI
- CAMPYLOBACTER
- META-ANALYSIS
Statistics from Altmetric.com
Significance of this study
What is already known on this subject?
In developed countries, the prevalence of IBD is steadily increasing while the prevalence of Helicobacter pylori infection is in decline.
A negative association between H. pylori infection and IBD has been suggested.
The effect of common medications used in IBD, such as sulfasalazine and antibiotics, on the association between H. pylori infection and IBD, is controversial.
No recent global comprehensive systematic synthesis of data in relation to H. pylori infection and IBD has been published, and no meta-analysis on enterohepatic Helicobacter spp (EHS) and Campylobacter spp and IBD has been conducted to date.
What are the new findings?
The current comprehensive meta-analysis, including 80 789 individuals, showed that there is a consistent negative association between H. pylori infection and IBD. In contrast, EHS (in particular non-H. pylori-like EHS) and Campylobacter spp (in particular C. concisus and C. showae) increase the risk of IBD.
The negative association between H. pylori infection and IBD is present irrespective of age, ethnicity and H. pylori detection method.
H. pylori infection is negatively associated with Crohn’s disease and UC and with IBD unclassified.
Medications commonly used in IBD such as sulfasalazine, mesalazine and corticosteroids do not influence the negative association between H. pylori infection and IBD. Antibiotics, however, appear to amplify this negative association.
How might it impact on clinical practice in the foreseeable future?
The results obtained by the current meta-analysis provide insights into the true direction of the association between H. pylori infection and IBD. If H. pylori infection indeed protects against IBD, selective treatment and surveillance of individuals at high risk of developing serious H. pylori-related gastric pathologies would be more relevant than a population-wide eradication approach, which has currently been proposed in some Asian countries.
Introduction
Helicobacter pylori infection has been associated with the development of a range of diseases, including peptic ulcer disease (10%), non-cardia gastric cancer (1–3%) and gastric mucosa associated lymphoid tissue lymphoma (<0.1%).1 Furthermore, H. pylori was classified as a class 1 carcinogen by WHO in 1994. Paradoxically, the falling prevalence of H. pylori infection has been associated with the development of IBD, chronic relapsing inflammatory conditions of the GI tract that are known to predispose to colon cancer.2 Over the last four decades, a dramatic increase in the incidence of IBD has been observed, especially in developed countries,3 ,4 with more recent studies reporting rising incidence rates of IBD in Asia that parallel westernisation.5 Interestingly, the opposite trend has been observed in H. pylori infection, with the latest epidemiological studies showing a significant decline in the industrialised world and in countries undergoing westernisation.6 Both phenomena have been associated with improved socioeconomic conditions and widespread use of antimicrobial treatments for common infections in childhood.1 ,5
The major forms of IBD are Crohn's disease (CD), UC, and IBD unclassified (IBDU). IBDU is a term suggested for patients in whom there is clinical and endoscopic evidence of IBD affecting the colon, without small bowel involvement, and no definitive histological or other evidence to favour either CD or UC.7 The aetiology of IBD is yet to be elucidated; however, studies would suggest that they are multifactorial diseases involving the interplay between host genetic factors, the immune response, the environment and the intestinal microbiome.5 Currently, it is hypothesised that intestinal micro-organisms, in association with a disruption of the GI epithelium, stimulate and subsequently drive a dysregulated immune response in genetically predisposed individuals, which results in chronic intestinal inflammation.8 How H. pylori infection fits in this hypothesis is unknown, however, a range of immunological and microbial mechanisms have been postulated (figure 1). An alternative hypothesis that cannot be discounted, however, is that IBD is a protective factor against H. pylori infection, with specific host genetic factors, IBD-associated gastric mucosal alterations and the use of certain medications, playing a significant role in this scenario (figure 1).
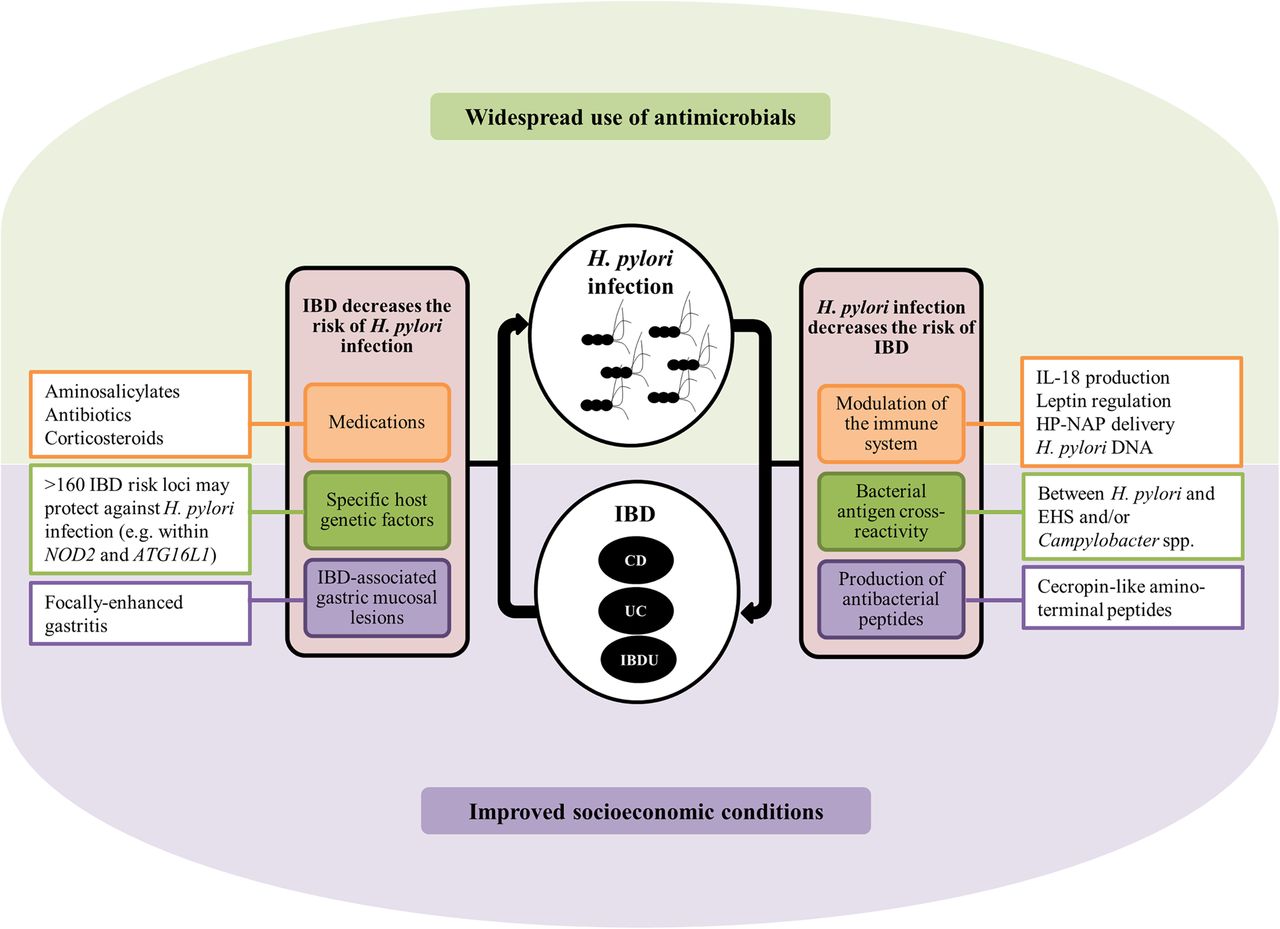
Improved socioeconomic conditions and widespread use of antimicrobials have been associated with the reduction of Helicobacter pylori infection and the increase of IBD. However, it is plausible that the increased risk of IBD is, in part, due to a decrease in the prevalence of H. pylori infection. The immunological mechanisms involved in this scenario include the accumulation of dendritic and regulatory T cells through an increased production of interleukin (IL)-18 and the satiety hormone leptin, exposure to H. pylori neutrophil-activating protein (HP-NAP) and H. pylori chromosomal DNA, two presumptive anti-inflammatory molecules, and cross-reactivity between antigens from H. pylori and enterohepatic Helicobacter spp (EHS) and/or Campylobacter spp. An additional mechanism is the production of antibacterial peptides by H. pylori that may have an impact on the abundance of other micro-organisms in the GI tract,9 and thus influence GI dysbiosis. Alternatively, IBD could be a protective factor against H. pylori infection through: (1) specific host genetic factors that increase the susceptibility to IBD10 but may protect against H. pylori infection, (2) the use of common medications in IBD such as aminosalicylates, antibiotics and corticosteroids that might impact on H. pylori infection per se by yet unknown mechanisms, and/or (3) the presence of IBD-associated gastric mucosal lesions that may create an inhospitable environment for H. pylori colonisation. CD, Crohn's disease; IBDU, IBD unclassified.
In addition, other bacterial species that are closely related to H. pylori, including enterohepatic Helicobacter spp (EHS) and Campylobacter spp, have been postulated to be micro-organisms involved in IBD pathogenesis. In the case of Helicobacter spp, the association between Helicobacter fennelliae and Helicobacter cinaedi and homosexual proctitis provides the most convincing evidence of Helicobacter-related human GI disease to date, potentially fulfilling Koch's second, third and fourth criteria.11 The first study to examine the possible association between Campylobacter spp and IBD was conducted in 1984.12 While this and later studies failed to provide evidence for an association,12–14 a more recent study by Gradel et al15 has reported C. jejuni infection to be associated with an increased risk of IBD and flare-ups of IBD. More recently, studies investigating the role of other emerging Campylobacter spp in IBD have provided compelling evidence that supports a role for C. concisus in the pathogenesis of these GI disorders.8
In an attempt to clarify this complex setting, we conducted a comprehensive meta-analysis on the association between H. pylori infection and IBD to estimate true pooled effect sizes, to identify potential causes for previous conflicting results and to determine the true direction of this association. Further, novel meta-analyses addressing the association between EHS and Campylobacter spp and IBD, were also conducted.
Materials and methods
The current systematic review and meta-analysis met the Preferred Reporting Items for Systematic Reviews and Meta-analysis statement requirements.16
Search strategy
Electronic databases, including PUBMED, Ovid, Scopus, ScienceDirect, CINAHL, LILACS, IMBIOMED, Scielo, IngentaConnect, Nature Publishing Group and Cochrane database, were searched up to July 2015 for all case-control studies assessing H. pylori infection and/or EHS and/or Campylobacter spp in IBD. Further hand-searching was also conducted. The search strategy included the Medical Subject Headings terms and/or text words outlined in table 1. No other limits or advanced features (eg, explosion) were used.
Medical Subject Headings (MeSH )and text words used in the literature search strategy
Study selection
Studies were selected if they met the following criteria: patients were clearly diagnosed with IBD (including CD, UC and IBDU), the study had a case-control design, H. pylori infection was detected by at least one highly sensitive and specific method (histology, culture, rapid urease test (Campylobacter-like organism (CLO) test), serology and/or urea breath test (UBT)) or detection of EHS and Campylobacter spp was conducted by standard methods (culture, serology and/or molecular techniques), sufficient information to calculate the effect size was available, and the manuscript was published in a peer-reviewed journal as a full paper.
Data extraction and quality assessment
The following information was collected from each study by two investigators independently: author, year of publication, journal, study population, H. pylori and/or EHS and/or Campylobacter spp detection method, EHS and/or Campylobacter spp identified, IBD subtype (CD, UC and IBDU), total cases, total non-IBD controls, previous/current use of medications (sulfasalazine, mesalazine, corticosteroids and/or antibiotics) and number of H. pylori/EHS/Campylobacter spp-positive and H. pylori/EHS/Campylobacter spp-negative individuals in each subgroup. Any disagreements regarding the retrieved information were resolved by consensus. In addition, the quality of the included studies was assessed using the Newcastle-Ottawa scale, which judges the selection of the study groups, the comparability of the groups and the ascertainment of the exposure of interest, to assign a maximum score of 9 stars.
Statistical analysis
The pooled odd ratios (P-ORs) in the meta-analysis were calculated by weighting individual ORs by the inverse of their variance. Since outcomes were relatively rare, ORs were considered approximations of risk ratios (RRs). The ORs as well as 95% CIs were calculated using the random-effects model as it assumes that the true effect might vary from study to study and thus, estimates the mean of a distribution of true effects, assigning a more balanced weight to each study. Analysis using the fixed-effects model was carried out in the absence of heterogeneity, as a sensitivity analysis. All tests were two-tailed with a p value <0.05 considered statistically significant. The Cochran’s Q test was used to test for heterogeneity (p value <0.10 is indicative of heterogeneity). Given that the power of this statistical test is low when a meta-analysis includes a small number of studies, the Higgins test (I2) was also used, which describes the percentage of total variation across studies that is due to heterogeneity rather than chance (low heterogeneity: <25%, moderate heterogeneity: 25–75% and high heterogeneity: >75%).17 Leave-one-out sensitivity as well as stratified analyses were conducted to assess statistical robustness and to detect the possible causes of heterogeneity between studies. Funnel plots and Egger's regression asymmetry tests were used to assess publication bias. Analyses were performed using the Comprehensive Meta-Analysis program V. 2.0 (Biostat, Englewood, New Jersey, 2004).
Results
Search results
The search strategy for the meta-analysis on gastric H. pylori infection and IBD yielded 447 publications (figure 2). Sixty studies addressing the association between H. pylori infection and the risk of IBD were identified for their potential inclusion in the current meta-analysis. Of these, 40 studies fulfilled the inclusion criteria after detailed evaluation. Thirty-seven of these studies included patients with CD,18–54 31 studies included patients with UC19–26 ,28–31 ,35 ,38–51 ,54–57 and 6 studies included patients with IBDU (table 2).26 ,29 ,45 ,48 ,49 ,51 Given that the two selected studies by Oliveira et al36 ,57 used different case subjects (CD vs UC) but the same control group, only the control group data from the latest publication was used for the meta-analysis as this corresponded to revised results according to the authors. In addition, two publications by Parente et al38 ,39 were included in the current meta-analysis as patients and controls were completely independent and were recruited in two different time points.
Main characteristics of the included studies in the meta-analysis on Helicobacter pylori infection and IBD

Flow diagram of the systematic review of the literature. EHS, enterohepatic Helicobacter spp.
For the meta-analysis on the association between EHS and IBD, 25 studies were identified for potential inclusion and 15 fulfilled the selection criteria.29 ,36 ,54 ,57–68 For the meta-analysis on the association between Campylobacter spp and IBD, 22 studies were identified for potential inclusion and 9 fulfilled the selection criteria.12 ,13 ,29 ,69–74 Three of the studies included in the meta-analysis on EHS and IBD,60 ,63 ,68 and two included in the meta-analysis on Campylobacter spp and IBD,71 ,74 were conducted by our research group, however, they were suitable for inclusion given that they comprised independent study samples and tested different biological specimens. Search strategy results are outlined in figure 2. The general characteristics of all the studies included in the current meta-analysis are outlined in table 2⇓–4.
Main characteristics of the included studies in the meta-analysis on enterohepatic Helicobacter species and IBD
Main characteristics of the included studies in the meta-analysis on Campylobacter species and IBD
Study quality
More than half of the studies obtained high scores (61%, 39/64), defined as ≥6 stars, in the Newcastle-Ottawa scale assessment (table 2⇑–4). When leave-one-out sensitivity analyses were conducted, all the results remained significant in the overall (H. pylori and IBD, EHS and IBD, and Campylobacter spp and IBD) and stratified analyses (by IBD subtype, age, ethnicity, use of medications, detection methods, H. pylori-like (HPL)-EHS vs non-HPL-EHS and Campylobacter spp), inferring statistical robustness.
Association between gastric H. pylori infection and IBD
The total study sample included 6130 patients with IBD and 74 659 non-IBD controls. Overall analysis comprising all patients with IBD, including patients with CD, UC and IBDU, showed a negative association between H. pylori infection and IBD (P-OR: 0.43, 95% CI 0.36 to 0.50, p value <1e-10) (figure 3). Stratified analyses by IBD subtype included 2938 patients and 74 012 non-IBD controls in the CD analyses, 2520 patients and 73 087 non-IBD controls in the UC analyses, and 286 patients and 70 247 non-IBD controls in the IBDU analyses. The remaining 386 patients with IBD were excluded from these analyses given that it was not clear with which IBD subtype they presented. These stratified analyses consistently showed a negative association in patients with CD (P-OR: 0.38, 95% CI 0.31 to 0.47, p value <1e-10), UC (P-OR: 0.53, 95% CI 0.44 to 0.65, p value <1e-10) and IBDU (P-OR: 0.43, 95% CI 0.23 to 0.80, p value 0.008) (see online supplementary figure S1). Heterogeneity was moderate in the overall analysis (figure 3) and very low to moderate in the stratified analyses by IBD subtype (see online supplementary figure S1), with no evidence of publication bias (see online supplementary table S1).

Forest plots of the meta-analysis of Helicobacter pylori infection and IBD. The pooled ORs with 95% CIs were calculated using the random effects model (diamond). The filled squares represent the studies in relation to their weights. Q, Cochran's Q test; I2, Higgins test.
Consistent negative association between gastric H. pylori infection and IBD irrespective of age, ethnicity and detection techniques
Stratified analyses by age, in which the studies were divided into two categories termed paediatric (those including subjects ≤16 years old, n=5 studies, 671 patients with IBD and 5878 non-IBD controls) and adult (those including subjects >16 years old, n=35 studies, 5459 patients with IBD and 68 781 non-IBD controls), showed a negative association in paediatric (P-OR: 0.24, 95% CI 0.14 to 0.43, p value <1e-10) and adult (P-OR: 0.45, 95% CI 0.38 to 0.53, p value <1e-10) patients with IBD, however, this negative effect was clearly stronger in paediatric individuals (figure 4). Heterogeneity was low in the stratified analyses including paediatric studies and moderate in the analyses including adult studies (figure 4), with no evidence of publication bias (see online supplementary table S1).
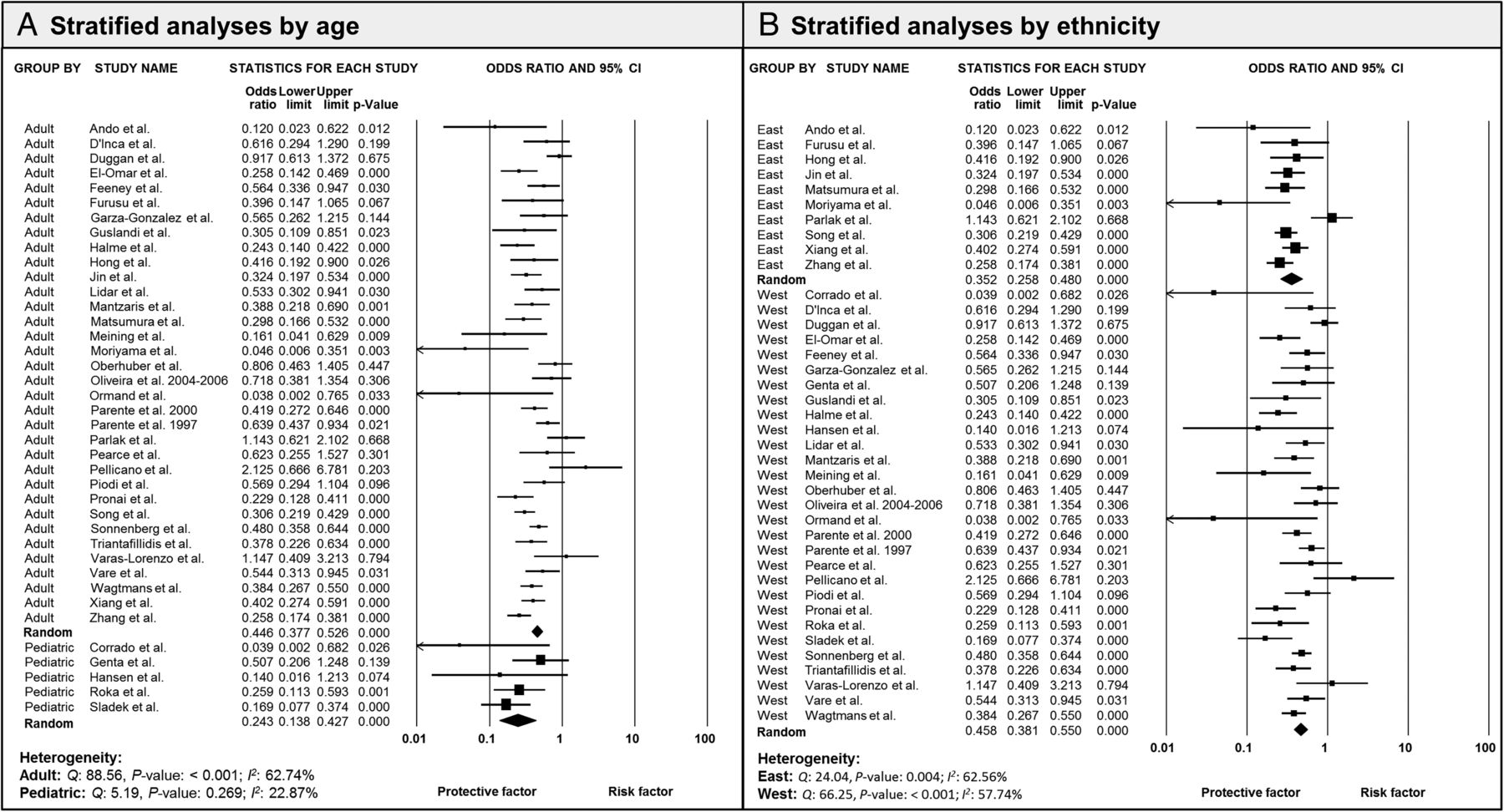
Forest plots of stratified analyses by (A) age and (B) ethnicity. The pooled ORs with 95% CIs were calculated using the random effects model (diamond). The filled squares represent the studies in relation to their weights. Q, Cochran's Q test; I2, Higgins test.
Ten studies addressing the association between H. pylori infection and IBD in Eastern populations (1304 patients with IBD and 1788 non-IBD controls) and 30 studies addressing this association in Western populations (4826 patients with IBD and 72 871 non-IBD controls), were included in the stratified analyses by ethnicity. These analyses showed a strong negative association between IBD and H. pylori infection in individuals from Eastern (P-OR: 0.35, 95% CI 0.26 to 0.48, p value <1e-10) and Western populations (P-OR: 0.46, 95% CI 0.38 to 0.55, p value <1e-10) (figure 4). Heterogeneity was moderate in these analyses (figure 4), with no evidence of publication bias (see online supplementary table S1).
Given that differences in the H. pylori detection techniques used in the individual studies could potentially bias the current meta-analysis, stratified analyses by detection methods (histology vs serology vs UBT vs multiple (more than one technique)) were also conducted. Eight studies using histology (1830 patients with IBD and 69 113 non-IBD controls), 11 studies using multiple techniques (1405 patients with IBD and 2528 non-IBD controls), 12 studies using serology (1925 patients with IBD and 1842 non-IBD controls) and 9 studies using UBT (970 patients with IBD and 1176 non-IBD controls), were included in these analyses. Interestingly, the negative association between H. pylori infection and IBD was found to be significant regardless of the H. pylori detection technique employed (P-OR: 0.56, 95% CI 0.38 to 0.81, p value=0.002 for histology; P-OR: 0.43, 95% CI 0.34 to 0.53, p value <1e-10 for multiple techniques; P-OR: 0.43, 95% CI 0.33 to 0.57, p value <1e-10 for serology; and P-OR: 0.34, 95% CI 0.22 to 0.54, p value <1e-10 for UBT) (see online supplementary figure S2). Heterogeneity was moderate in these analyses (see online supplementary figure S2).
The effect of common medications on the association between gastric H. pylori infection and IBD
The effect of medications commonly used by patients with IBD on H. pylori infection was also investigated through stratified analyses. For this, patients with IBD were stratified by use of sulfasalazine (702 patients with IBD), mesalazine (557 patients with IBD), corticosteroids (268 patients with IBD) and antibiotics (117 patients with IBD), and compared with their respective non-IBD controls (table 5). To complement these results, stratified analyses including patients with IBD who were not given medications, were also conducted. For this, patients who did not use some or any medications were divided into two subgroups: (1) not using sulfasalazine but with unclear previous or current use of other medications (NOSASP), and (2) not using medications at all (NOMED). Patients with IBD in the NOSASP subgroup were compared with patients with IBD using sulfasalazine and non-IBD controls. Patients with IBD in the NOMED subgroup were compared with non-IBD controls only (table 5). Individual stratified analyses including patients with IBD not using mesalazine, antibiotics or corticosteroids were not conducted given the limited and unclear data available.
Patients included in the stratified analyses by medication
The effect sizes in the sulfasalazine (P-OR: 0.41, 95% CI 0.26 to 0.65, p value <1e-10) and mesalazine (P-OR: 0.51, 95% CI 0.33 to 0.80, p value=0.003) subgroup analyses were comparable to the overall results (see online supplementary figure S4). In contrast, the negative association between H. pylori infection and IBD in patients taking antibiotics (P-OR: 0.22, 95% CI 0.12 to 0.40, p value <1e-10) and corticosteroids (P-OR: 0.30, 95% CI 0.22 to 0.42, p value <1e-10) appeared to be increased (see online supplementary figure S4). However, analyses in the NOMED subgroup were also statistically significant (P-OR: 0.36, 95% CI 0.18 to 0.74, p value=0.005) and comparable to the corticosteroids subgroup results (see online supplementary figure S5). Further, analyses comparing the NOSASP subgroup and non-IBD controls showed comparable results to the overall analyses (P-OR: 0.45, 95% CI 0.26 to 0.81, p value=0.007), and analyses comparing the NOSASP subgroup and patients with IBD using sulfasalazine did not reach statistical significance (P-OR: 0.59, 95% CI 0.25 to 1.40, p value=0.233) (see online supplementary figure S5). Heterogeneity was moderate to high in the sulfasalazine, mesalazine and NOSASP subgroup analyses, and very low in the antibiotics, corticosteroids and NOMED subgroup analyses (see online supplementary figures S4 and S5). No significant publication biases were identified in these stratified analyses based on examination of funnel plots and Egger's test (see online supplementary table S1).
Association between enterohepatic Helicobacter species and IBD
Given that a number of studies have reported the presence of HPL and other Helicobacter spp (H. bilis, H. canis, H. ganmani, H. hepaticus, H. trogontum, ‘H. rappini,’ H. cinaedi, H. canadiensis, H. cholecystus, H. pullorum, H. brantae, H. fennelliae and H. muridarum) in the lower GI tract of patients with IBD, we conducted a meta-analysis to elucidate the association between these EHS and IBD. HPL-EHS are defined as H. pylori strains showing high 16S rRNA gene similarity to gastric H. pylori strains on Basic Local Alignment Search Tool (BLAST) searches (98–100% using 360–1482 bp fragments), but detected in the colon.
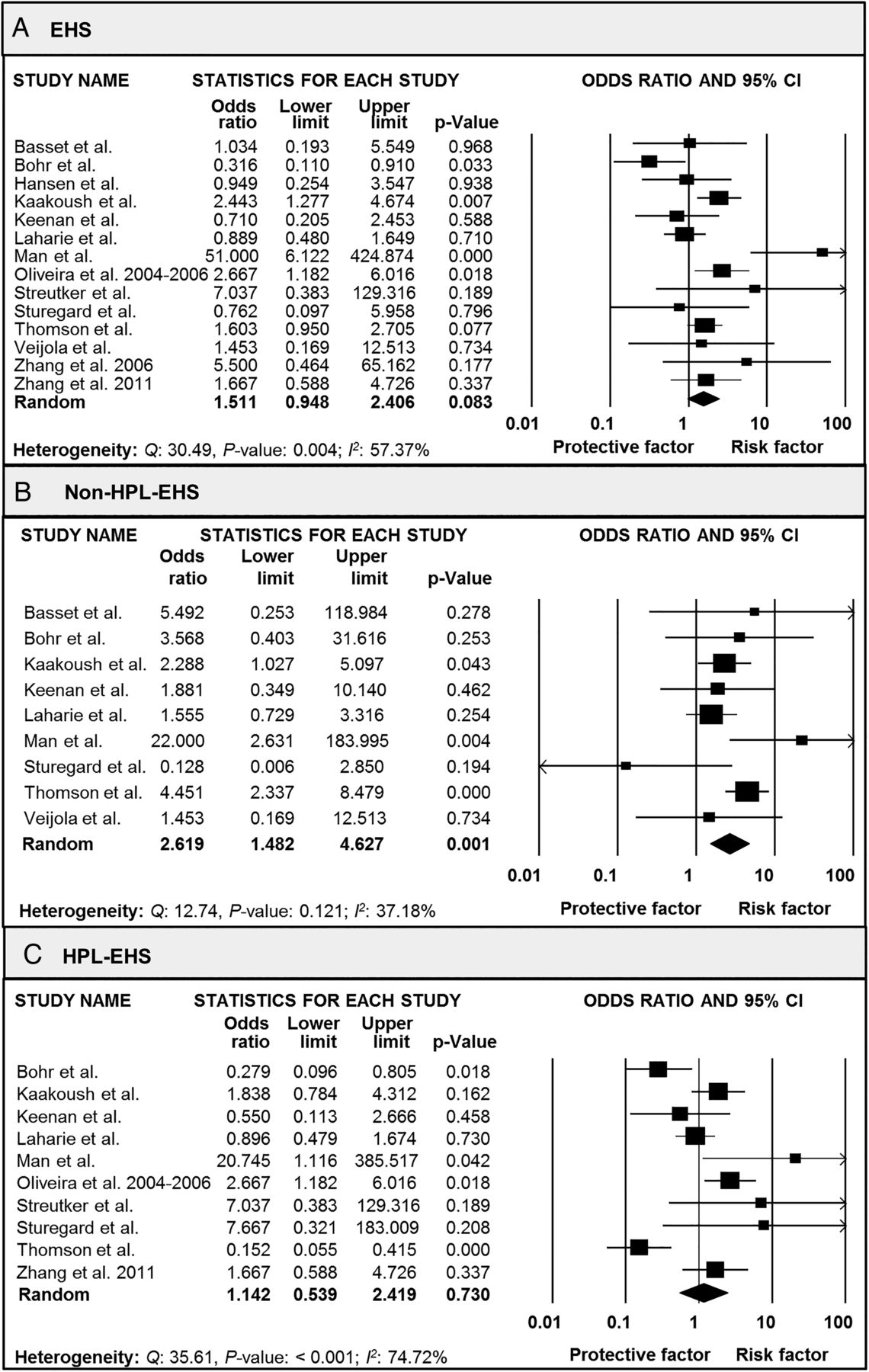
Overall analyses, which included 15 studies comprising 906 patients with IBD and 758 non-IBD controls, showed a borderline association between EHS and IBD (P-OR: 1.51, 95% CI 0.95 to 2.41, p value=0.083) (figure 5). The overall prevalence of EHS was found to be 26% in patients with IBD and 24% in non-IBD controls. Interestingly, when stratified analyses were conducted to compare non-HPL-EHS (545 patients with IBD and 524 non-IBD controls) with HPL-EHS (684 patients with IBD and 642 non-IBD controls), a consistent association was found between non-HPL-EHS and IBD (P-OR: 2.62, 95% CI 1.48 to 4.63, p value=0.001) while no significant association was found between HPL-EHS and IBD (P-OR: 1.14, 95% CI 0.54 to 2.42, p value=0.730) (figure 5). The prevalence of HPL-EHS was found to be 17.1% in patients with IBD and 20% in non-IBD controls while non-HPL-EHS were detected in 21.8% of patients with IBD and 10.5% of non-IBD controls. Heterogeneity was moderate in these analyses (figure 5), with no evidence of publication bias (see online supplementary table S1).

Forest plots of the meta-analysis of (A) enterohepatic Helicobacter spp (EHS) and IBD, (B) non-Helicobacter pylori-like (HPL)-EHS and IBD, and (C) HPL-EHS and IBD. The pooled ORs with 95% CIs were calculated using the random effects model (diamond). The filled squares represent the studies in relation to their weights. Q, Cochran's Q test; I2, Higgins test.
Further stratification by EHS detection techniques in which studies were divided into biopsy-based (studies using biopsy specimens, n=13 studies) and non-biopsy-based (studies using stool specimens or serology, n=2 studies) subgroups, also failed to show statistical significance when analysing all EHS and HPL-EHS (see online supplementary figure S3). Interestingly, when analysing non HPL-EHS, significant results were only obtained with biopsy-based studies (P-OR: 2.41, 95% CI 1.40 to 4.13, p value=0.001) (see online supplementary figure S3). Heterogeneity was moderate to high in these analyses (see online supplementary figure S3).
Association between Campylobacter species and IBD
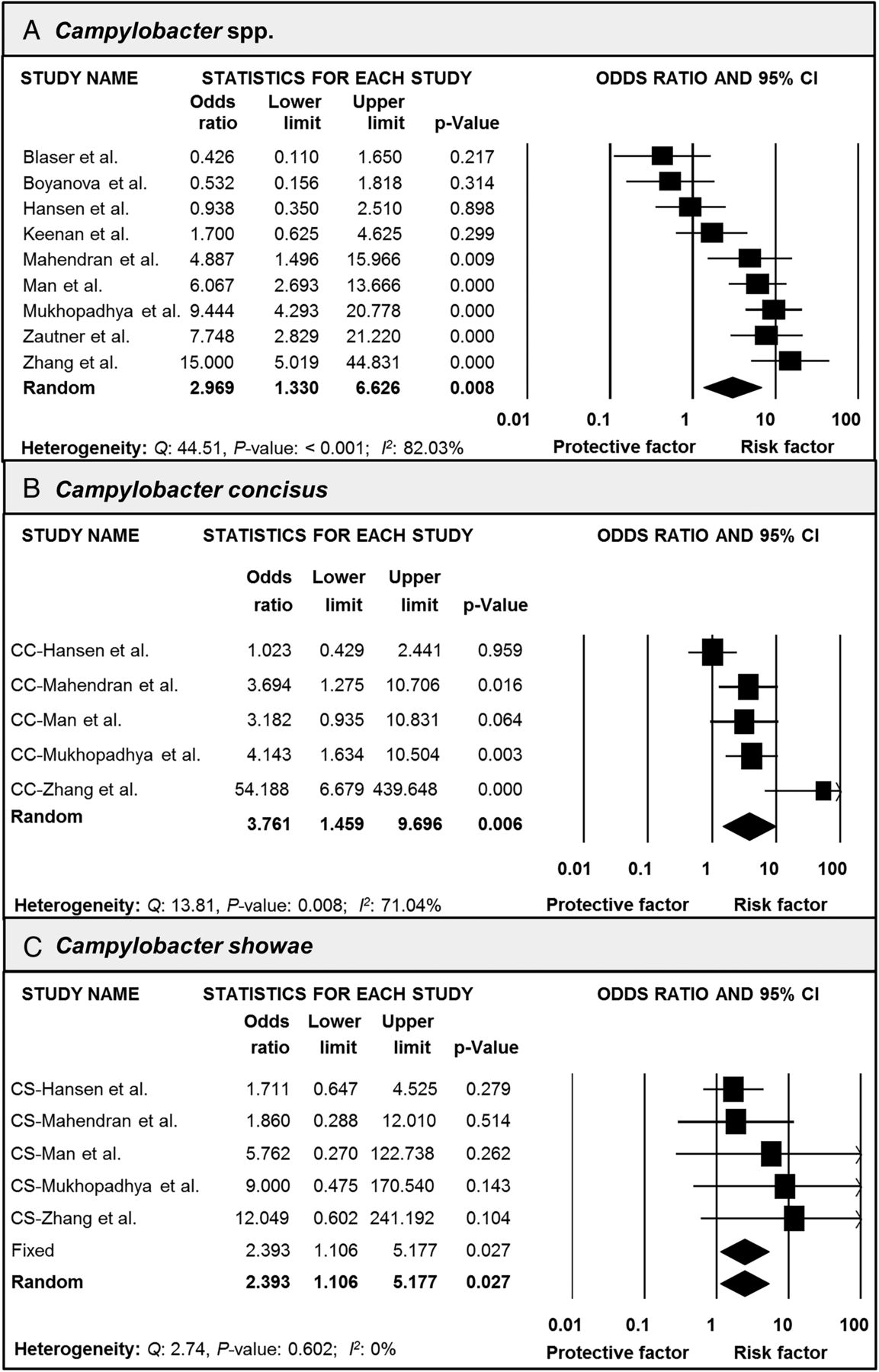
Recent findings suggest that a number of Campylobacter spp might be involved in the pathogenesis of IBD (please refer to the comprehensive review by Kaakoush et al75 for more information on this topic). Thus, the association between IBD and Campylobacter spp, including C. jejuni, C. coli, C. concisus, C. lari, C. curvus, C. showae, C. hominis, C. ureolyticus, C. hyointestinalis, C. rectus, C. gracilis and C. upsaliensis was also investigated in the current meta-analysis. The total sample included 519 patients with IBD and 1133 non-IBD controls. Overall analyses showed a significant association between Campylobacter spp and IBD, with a P-OR of 2.97 (95% CI 1.33 to 6.63, p value=0.008) (figure 6). In total, Campylobacter spp were detected in 39% of patients with IBD and 13% of non-IBD controls. Further stratified analyses by Campylobacter spp were conducted when sufficient information was available, which was the case for C. jejuni, C. concisus, C. hominis, C. showae, C. ureolyticus, C. rectus and C. gracilis. Strikingly, these analyses showed that C. concisus (P-OR: 3.76, 95% CI 1.46 to 9.70, p value=0.006) and C. showae (P-OR: 2.39, 95% CI 1.11 to 5.18, p value=0.027) were the Campylobacter spp mainly responsible for the observed association with IBD (figure 6). Further, C. hominis (P-OR: 1.58, 95% CI 0.91 to 2.75, p value=0.108) and C. ureolyticus (P-OR: 2.34, 95% CI 0.77 to 7.16, p value=0.136) showed borderline results, while C. jejuni, C. rectus and C. gracilis failed to show significant associations (data not shown). Heterogeneity was high in the overall analysis but very low for the majority of the stratified analyses (figure 6), with no evidence of publication bias (see online supplementary table S1).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plots of the meta-analysis of (A) Campylobacter spp and IBD, (B) Campylobacter concisus and IBD, and (C) Campylobacter showae and IBD. The pooled ORs with 95% CIs were calculated using the random effects model (diamond). The filled squares represent the studies in relation to their weights. Q, Cochran's Q test; I2, Higgins test.
Stratification by detection (biopsy-based (n=4 studies) versus stool-based (n=2 studies) versus serology-based (n=3 studies)) methods showed significant results for stratified analysis including biopsy-based studies (P-OR: 5.05, 95% CI 1.51 to 16.83, p value=0.008) but not stool or serology-based studies (P-OR: 1.87, 95% CI 0.39 to 8.92, p value=0.432; and P-OR: 1.88, 95% CI 0.17 to 20.39, p value=0.604, respectively) (see online supplementary figure S3). Heterogeneity was high in these analyses (see online supplementary figure S3).
Discussion
The current meta-analysis collected data from all available studies that report the prevalence of H. pylori infection in patients with IBD and non-IBD controls, and fitted the selection criteria. The final selection included 40 studies conducted in 17 countries worldwide, with a total sample size of 80 789 individuals. Overall analyses showed a consistent negative association between H. pylori infection and IBD. This negative association persisted in CD, UC and IBDU subgroup analyses. Interestingly, the effect size appeared to be stronger in patients with CD and IBDU when compared with patients with UC. The novel association between H. pylori infection and IBDU requires further investigation as it is difficult to establish purely on the basis of the current study if this is a true association or just an artefact due to lack of a universally accepted definition of IBDU that leads to misdiagnosis.
In relation to CD and UC, these entities have been postulated to involve different immunological backgrounds. Activated innate and acquired immune responses and loss of tolerance to enteric commensal bacteria are present in CD and UC, however, type 1 T helper lymphocyte (Th1) and Th17-related cytokines involved in innate immunity (eg, interleukin (IL) 12, IL-23 and IL-27) are selectively activated in CD.76 H. pylori infection has been shown to be negatively associated with IBD and asthma, eczema, oesophageal adenocarcinoma, and possibly, other T cell driven immunological or metabolic disorders.77 ,78 The mechanisms behind this apparent protective effect include accumulation of tolerogenic dendritic cells and highly suppressive regulatory T cells (Tregs) through IL-18 production.79 In addition, H. pylori has been shown to regulate the gastric secretion of the satiety hormone leptin,80 ,81 a proinflammatory adipocytokine that has been shown to be increased in patients with IBD,82 ,83 and experimental colitis in mice, in which it was correlated with disease severity.84 Consistently, a recent study has shown that the use of a leptin blocker, pegylated leptin antagonist, enhances systemic and mucosal Tregs and CD39+ Tregs in mice with colitis.85 Interestingly, it has also been demonstrated that human Tregs are capable of producing substantial amounts of leptin that are responsible for an autocrine inhibitory loop that constrains their expansion.86 In addition, delivery of H. pylori neutrophil-activating protein, which has been shown to reduce inflammation through agonist ligation of toll-like receptor 2 and increased IL-10 production,87 ,88 and H. pylori chromosomal DNA, which has been shown to be sufficient to prevent sodium dextran sulfate-induced colitis in mice through inhibition of type I interferon and IL-12 production,89 are also proposed immunoregulatory mechanisms.
Given that age (due to differences in the immune response) and ethnicity (due to differences in H. pylori strains and/or host genetic factors) might be involved in the association between H. pylori infection and IBD, further stratified analyses were performed. A negative association between H. pylori infection and IBD in paediatric and adult subjects was found. This association appears to be stronger in paediatric individuals, which is consistent with previous murine models showing that early exposure to H. pylori induced immune tolerance while Tregs from uninfected or adult infected mice failed to confer the same protection.90 ,91 Further, Treg-predominant T cell responses have been shown to be responsible for the mild gastritis typical of H. pylori-infected children.92
In addition, when the data was stratified according to ethnicity, significant associations were found in Eastern and Western populations. Numerous studies have shown that H. pylori cag pathogenicity island-positive strains are particularly associated with an increased risk of gastric diseases.77 ,93 Furthermore, it has been recently shown that H. pylori infection downregulates the expression of the T cell co-inhibitory molecule B7-H1 in gastric epithelial cells in a CagA-dependent manner, which might contribute to the hyporesponsiveness of CD4(+) effector T cells and accumulation of Tregs.94 Also, H. pylori infection has been shown to induce the production of the chemokine CCL20 in gastric epithelial cells via cag pathogenicity island-dependent nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) signalling, a phenomenon believed to be involved in Tregs homing to the gastric mucosa as the majority of Tregs express its receptor CCR6.95 H. pylori strains expressing CagA represent 60–70% of Western strains and approximately 100% of East-Asian strains.96 Interestingly, the negative association between H. pylori infection and IBD was shown to be more significant in Eastern populations in the current meta-analysis, suggesting that CagA may be a determining factor. Consistently, a recent meta-analysis on H. pylori infection and risk of oesophageal cancer has shown that the negative association observed in these patients is only present in individuals colonised with H. pylori CagA-positive strains.97 Given the current limited data, further studies investigating the prevalence of H. pylori infection and H. pylori´s main virulence factors in patients with IBD, are required.
While host genetic factors might also be associated with the differences found between human populations in the current analyses, the most widely studied susceptibility gene for IBD, NOD2 (also known as CARD15), is unlikely to be responsible for these findings given that polymorphisms in this gene are uncommon in Asian populations.98 ,99 In contrast, studies investigating the role of ATG16L1 polymorphisms (eg, rs2241880) in this context might be worth pursuing as recent evidence suggests that genetic variants in this autophagy gene might modulate the risk of IBD and H. pylori infection per se in Caucasian and Asian populations.100–103
While current evidence shows that H. pylori might be a protective factor against IBD, a number of human studies and animal models have suggested that EHS,11 and Campylobacter spp,8 increase the risk of IBD development. Given the similarities between these bacterial species, the development of adaptive immunity against a particular Helicobacter spp might confer protection against other Helicobacter or Campylobacter organisms. Indeed, Lemke et al104 have shown that co-infection with H. bilis and H. pylori attenuates H. pylori related gastritis in mice, which was attributed to H. bilis primed Tregs in the intestine that migrated to the gastric compartment and inhibited Th1 responses to subsequent H. pylori infection. Further, anti-H. pylori antibodies have been shown to confer a degree of protective immunity against a subsequent Campylobacter infection, indicating antigenic cross-reactivity between these two bacterial species.105 ,106 Thus, it is plausible that H. pylori infected individuals might mount a characteristic immune response against other Helicobacter or Campylobacter spp, which may decrease the likelihood of chronic intestinal inflammation.
To elucidate this, novel meta-analyses on the association between EHS and Campylobacter spp and IBD were conducted. Strikingly, significant associations between non-HPL-EHS and IBD as well as Campylobacter spp and IBD were found, while HPL-EHS analyses failed to show significance. A recent study reporting a phylogenetic analysis combining HPL-EHS detected in the colon of patients with IBD, and other gastric and extragastric (from oesophagus, gall bladder and liver) H. pylori strains, showed that most HPL-EHS clustered with other extragastric H. pylori strains, suggesting that certain strains of H. pylori may be adapted to extragastric colonisation.60 Thus, it is conceivable that as a result of this adaptation, these strains do not interact with the host or other microbes in the same manner as gastric H. pylori strains do, which would have an impact on the association with IBD.
The novel finding from the current meta-analysis that C. concisus and C. showae are responsible for the observed association between Campylobacter spp and IBD is in line with extensive previous research conducted by our group and others. The first report of emerging Campylobacter spp (C. concisus, C. showae, C. hominis, C. gracilis, C. rectus and C. ureolyticus) in patients with CD was conducted by the Mitchell group, in which 82% of the intestinal biopsy specimens from newly diagnosed paediatric patients with CD were found to be positive by PCR for Campylobacter as compared with 23% of controls.74 Consistently, of these emerging Campylobacter spp detected, only C. concisus was found to be significantly more prevalent in patients with CD (51%) than in controls (2%) (p value <0.0001).74 Further studies conducted by us and others, have supported this finding in patients with CD71 ,107 ,108 and UC.29 ,70 ,72 ,109 Moreover, recent advances suggest that C. concisus is an immunogenic micro-organism as C. concisus flagellin B, ATP synthase F1 α subunit and outer membrane protein 18 have been shown to be consistently recognised by all patients with CD110 while Campylobacteraceae DNA has been found in the lymph nodes of patients with CD.111
Despite comprehensive evidence supporting an association between C. concisus and IBD, the fact that C. concisus is detected in the intestine of a third of non-IBD subjects has generated controversy. A possible explanation is the existence of specific genomospecies that might be associated with diverse disease outcomes.112–117 Indeed, our group recently proposed that C. concisus strains can be subdivided into two pathotypes that are distinct from non-pathogen strains: (1) adherent and invasive C. concisus, which possess greater ability to survive intracellularly within host cells, and (2) adherent and toxigenic C. concisus, which produce a zonula occludens toxin with the potential to target tight junctions of host cells.75
Evidence is less concrete regarding the association between C. showae and IBD, however, early studies by our group detected this bacterium in 4–9% of patients with CD from two independent cohorts.71 ,74 Further studies on CD and UC were supporting of this finding.29 ,70 ,72 Interestingly, this bacterium has also been detected in patients presenting with other GI conditions such as cholangitis118 and hepatolithiasis.119 Overall, while further investigations are required to reach conclusive remarks on the aetiology of IBD, the current findings suggest that emerging Campylobacter spp, predominantly C. concisus and C. showae, could play a role in the pathogenesis of a subset of these GI disorders.
As mentioned previously, a further scenario could be that patients with IBD are protected against H. pylori infection. However, this alternative hypothesis is unlikely for a number of reasons. First, it is well established that IBD shows a binomial distribution that includes one peak in late teenage-early adult years (mainly for CD) and a second in late adulthood (mainly for UC),5 while H. pylori infection is characteristically acquired in early childhood.120 Thus, H. pylori infection normally occurs prior to the onset of IBD. While early studies suggested that common medications used in the treatment of IBD may be involved in the protective effect against H. pylori infection, this view has been refuted by a significant number of studies20 ,23 ,27 ,35 ,40 ,49 ,51 as well as the current meta-analysis. Stratified analyses by medication showed that the use of antibiotics and corticosteroids might intensify the negative association between H. pylori infection and IBD. However, in the case of corticosteroids, the finding that patients with IBD who did not use any type of medication showed a comparable effect size as those individuals in the corticosteroids subgroup, would argue against this view. In the case of antibiotics, further functional studies are required to establish their exact role in this matter. It is important to note, however, that the prevalence of H. pylori infection in patients with chronic obstructive lung disease, who are also exposed to long-term antimicrobial therapies, has been found to be comparable to controls.44 In addition, no significant difference was obtained when comparing the risk of H. pylori infection in patients with IBD using sulfasalazine and those who were not, suggesting that medications commonly used in IBD, apart from antibiotics, have only a limited effect on the risk of H. pylori infection, if any. These findings are in agreement with a study conducted by El-Omar et al,22 which did not identify any antimicrobial properties of sulfasalazine in vitro and also showed that 14-day treatment with this medication only minimally suppressed the 14C UBT in H. pylori-infected healthy volunteers. Further studies investigating the prevalence of H. pylori infection in patients taking sulfasalazine for other conditions such as rheumatoid arthritis have failed to provide consistent results.121 ,122
To date, only three meta-analyses have been published on the association between H. pylori infection and IBD.123–125 Luther et al,123 through a meta-analysis that comprised 5903 individuals, showed a statistically significant association between this bacterium and IBD (RR: 0.64, 95% CI 0.54 to 0.75). Wu et al,124 and Rokkas et al125 conducted further meta-analyses, which confirmed the results obtained by Luther et al,123 showing an RR of 0.48 (95% CI 0.43 to 0.54) and 0.62 (95% CI 0.55 to 0.71), respectively. Although the current meta-analysis is consistent with these previous results, some differences can be clearly identified between these studies. First, as a significant number of critical studies have been published since the meta-analysis by Luther et al,123 the current meta-analysis, which included 18 additional studies, comprising 75 418 additional individuals, provides markedly increased statistical power. Furthermore, although recently published, the meta-analysis by Wu et al124 included only 10 studies conducted in Asian populations with a very limited total study sample size (1299 patients with IBD and 1817 controls) while the global meta-analysis by Rokkas et al125 included only 33 studies (4400 patients with IBD and 4763 controls) and provided limited stratified analyses (only by IBD subtype, study design and H. pylori diagnosis). In contrast to Luther et al,123 Wu et al124 and Rokkas et al,125 the current meta-analysis also included patients with IBDU. In addition, for the first time, the current meta-analysis included stratified analyses by use of common medications in patients with IBD, allowing insights into the true direction of the association between H. pylori infection and IBD.
The current meta-analysis is not without limitations. Individuals in the non-IBD control group ranged from healthy volunteers to patients with severe pathology such as GI malignancies, which could introduce potential biases. Further, heterogeneity was found to be moderate to high in some of the analyses even though the data were stratified by IBD subtype, age, ethnicity, use of medications, EHS and Campylobacter spp. Stratified analyses by use of medication, however, should be considered with caution given that a number of potential biases exist including the interpretation of retrospective medication use, summation of prior medication exposure and the potential effect of overlapping medications. Given that a number of methodological differences might also account for the observed heterogeneity including detection techniques and specimen characteristics, further stratified analyses were conducted. Based on these analyses, biopsy-based methods that involve PCR and DNA sequencing appear to be superior to other forms of detection for EHS and Campylobacter spp. However, it was not possible to assess the effect of other methodological differences such as specimen processing times, specific PCR primer sets, reliability of serological assays and bowel preparation prior to colonoscopy due to the limited information available. In addition, it is important to note that the power of funnel plots and Egger's test is limited to distinguish chance from real asymmetry when less than 10 studies are included in a meta-analysis,126 leading to the possibility that publication biases might have been present in some of the current analyses. Furthermore, the role of improved socioeconomic conditions could not be assessed in the current meta-analysis given the limited data available and the methodological differences between studies investigating this factor.
In conclusion, the current comprehensive meta-analysis has demonstrated a significant negative association between H. pylori infection and IBD, particularly CD and IBDU. This association seems to be a global phenomenon that affects paediatric and adult individuals, and appears to be amplified by the use of antibiotics. In contrast, the use of other medications such as sulfasalazine, mesalazine and corticosteroids, do not appear to be influential. Furthermore, this is the first meta-analysis to show that non-HPL-EHS and Campylobacter spp, in particular C. concisus and C. showae, might increase the risk of IBD, a finding that is in favour of a role for bacterial antigen cross-reactivity in IBD pathogenesis (figure 1). As H. pylori is known to be a successful pathogen and immunomodulator that if not treated persists for the lifetime of the host, the current data would suggest that the simplistic path of eradicating this bacterium from human populations is unlikely to be beneficial to the host given that loss of H. pylori may increase the risk of other T cell driven immunological disorders.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online figures
- Data supplement 2 - Online table
Footnotes
Contributors NC-R, NOK, WSL and HMM contributed to conception and design of the study. NC-R and NOK contributed to data acquisition, analysis and interpretation of the data. NC-R drafted the initial version of the manuscript. NC-R, NOK, WSL and HMM commented on drafts of the paper and have approved the final draft of the manuscript.
Funding WSL receives funding from the Ministry of Higher Education, Malaysia (UM.C/625/HIR/MOHE/CHAN/13/1).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.