Article Text

Abstract
Sleep disorders are common in children with neurodisability. Their presentation is often complex. This complexity of presentation can make sleep disorders in children with neurodisability daunting to diagnose and manage. Both parents and healthcare professionals have identified sleep disorders as a healthcare outcome that they prioritise in children with neurodisability. We aim to explore the challenges of diagnosing sleep problems, discuss common difficulties with sleep in children with neurodisability and will touch on how to set up a service to support and manage sleep, working through case examples.
- neurodisability
- sleep
- paediatric practice
- medical education
- multidisciplinary teamcare
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Sleep difficulties are common in both typical developing children and those with neurodisability. Approximately 30%1 of preschool-aged children have sleep-related problems, whereas the prevalence of sleep disorders in children with neurodisability of any age can be as high as 80%.2 3
Difficulties with sleep can be complex with many contributing factors including muscle weakness, orofacial anomalies, chest wall issues, as well as abnormalities with the brainstem, hypothalamus, spinal cord or the airway, dependent on the neurodisability condition.4 A condition can predispose to sleep problems and medical interventions can make them worse. Treatment such as growth hormone used in Prader-Willi syndrome can exacerbate obstructive sleep apnoea (OSA). Insertion of vagal nerve stimulators can also lead to undetected respiratory events in patients with epilepsy. We have summarised some of the conditions to be aware of and their associated sleep difficulties in table 1.
Examples of associated sleep disorders in paediatric neurodisability clinical practice
This complexity of presentation can make sleep disorders in children with neurodisability daunting to diagnosis and manage. Sleep disorders have been identified by both parents and healthcare professionals as a healthcare outcome that they prioritise in children with neurodisability.5–7
We aim to explore the challenges of diagnosing sleep problems, discuss common difficulties with sleep in children with neurodisability and will touch on how to set up a service to support and manage sleep, working through case examples.
Baseline knowledge in sleep medicine
Despite the high prevalence of sleep disorders in paediatric neurodisability, exposure to sleep medicine in paediatric neurodisability training is at best sparse. A US study showed the average time dedicated to sleep in the curriculum was only 2.1 hours in sleep.8 A wider study of sleep education in over 400 medical schools in Australasia, India and Northern America showed a similar average. However,9 paediatric topics were covered in only 17 min compared with 2 hours on adult-related topics.
The picture in the UK is not much better. Unlike some of the countries listed above who offer specialist sleep medicine fellowship programmes, similar opportunities are not routinely available in the UK. There is ongoing work to improve this, with sleep medicine being introduced to the paediatric postgraduate curriculum in the UK from August 2018.10
In the Evelina London Children’s Hospital in early 2018, a local survey of 40 doctors including qualified paediatricians and trainees, involving 18 specialty groups, found 55% regularly see children with sleep difficulties. In terms of method, the survey on sleep education was performed by an email survey of paediatricians of all grades in the Evelina London Children’s Hospital. Further information on this is available on request from the authors. Most doctors reported no formal teaching in sleep medicine or at best one undergraduate lecture (70%). Just 33% felt confident or very confident discussing sleep difficulties, 55% were not at all confident in knowing what sleep studies are available and when to order them. Results are further detailed in table 2. These data suggest that many doctors are not confident in managing sleep difficulties, therefore require specialist support and further education in sleep medicine.
Paediatricians and trainees’ confidence in managing and diagnosing sleep difficulties
Sleep medicine is an area in which the management is best performed as part of a robust multidisciplinary team. A comprehensive sleep service should ideally include access to: doctors with sleep expertise, sleep physiologists, sleep practitioners (professionals with expertise in management of specific sleep disorders by behavioural/environmental approaches), specialist nurses and clinical psychologists. Psychology support particularly is key. However, there is significant variability in local service provision leading to vastly different experience for children and young people across the UK. In box 1 we have outlined sleep resources and training available to up-skill services.
Sleep resources and training
Training and support in sleep medicine
Sleep Scotland offers sleep counsellor training (local service management sign-off) plus teen sleep education package and parent/carer support hot line: http://www.sleepscotland.org
The Children’s Sleep Charity offers sleep practitioner training, school and parent education package, continuing professional development (CPD) updates, sleep success workshops for autism spectrum disorder (ASD) and attention deficit and hyperactivity disorder (ADHD) and residential staff training. There is also a parent/carer support hot line: http://www.thechildrenssleepcharity.org.uk
Cerebra offers parent telephone support and parent sleep workshops: http://www.cerebra.org.uk
SCOPE offers parent workshops and parent support: http://www.scope.org.uk/support/services/sleep-solutions
Southampton Sleep Training offers a 4-day course in ‘Managing children’s sleep disorders in clinical practice’, a 1-day course in ‘Essentials of Sleep Medicine for the busy doctor’, a 1-day course in ‘Behavioural insomnia’ and an update day with hot topics.
Training for Doctors and Sleep Physiologists Basic and Advanced Sleep Courses are a 1-day and 2-day course mainly theory based which includes neurological sleep disorders. Hosted by Association for Respiratory Technology and Physiology: http://www.artp.org.uk
International Sleep Medicine Course (Europe-wide recognition) is a theory based that includes an introduction to sleep scoring of polysomnography. Hosted by British Sleep Society: http://www.sleepsociety.org.uk
European Somnologist Exam covers comprehensive knowledge and skills base for more experienced sleep physician and physiologist. Hosted by European Sleep Research Society: http://www.esrs.eu
A-STEP Course is a practical online course for sleep physiologists. Hosted by American Academy of Sleep Medicine: http://www.aasm.org
Graduate Diploma in Pediatric Sleep Science: Practical online for scoring cardiorespiratory studies mainly. Hosted by the University of Western Australia: http://www.meddent.uwa.edu.au
MSc in Sleep Medicine: Theory and practical with neurology/behaviour emphasis. Hosted by Oxford University: http://www.ox.ac.uk
Improving access to services and knowledge regarding sleep disorders for children with neurodisability
A clear history is key to the identification and management of sleep disorders. Our colleagues have already outlined key questions in a previous paper.11 There are a number of simple paper-based assessments that can be included in a sleep ‘toolkit’ that can be put together with a degree of ease by the paediatrician to improve the management of sleep disorders. We have outlined these resources in box 2.
Toolbox for physicians
Listed tools should be available in a secondary care service (assessment to be done locally)
Sleep history sheet, for example, Sleep Evaluation Questionnaire can be found in ‘A clinical guide to Pediatric Sleep’ by Jodi Mindell and Judith Owens.
Visual sleep diaries, for example, American Academy of Sleep Medicine Diary—available for free online.
Sleep hygiene leaflet, for example, Encouraging Good Sleep Habits leaflet which can be found on Research Autism website.
Sleep questionnaires, for example, Sleep Disturbance Questionnaire for Children (SDQC) by Bruni (further details in review by Karen Spruyt, 2011).17
Outcome data, for example, Sleep Composite Score Questionnaire (Lucy Wiggs, Oxford).
Mental health screening, for example, Strengths and Difficulties Questionnaire, Revised Children Anxiety and Depression (RCAD) scale.
Specialist sleep questionnaires, for example, Morning Evening Questionnaire (MEQ) for possible circadian rhythm disturbance; Epworth Sleepiness Score for possible hypersomnolence.
Local expertise
Local disabled children’s social services to assist with organisation of appropriate respite.
Disabled children’s occupational therapy to consider bed adaptations such as safe sleep spaces or sleep pod from Creative Care.
Local baseline sleep investigations
Oximetry to look for clusters of desaturation with possible increased heart rate variability suggesting possible sleep disordered breathing.
Capnography looks for possible hypoventilation.
Available at sleep lab
Respiratory polygraphy includes measure of respiratory effort, rate, heart rate data and body position/movements to look at and determine presence or absence of sleep disordered breathing.
Polysomnography (PSG) is an overnight sleep study which measures body physiological parameters including sleep staging (from a variety of signals) as well as cardiorespiratory data and leg movements to determine quality of sleep.
Combined video telemetry and polysomnography is rarely used but sometimes helpful combined electroencephalogram (EEG) with PSG for specialist assessment of paroxysmal stereotypical events to try to distinguish between possible epilepsy such as frontal lobe epilepsies and parasomnia.
Multiple sleep latency test (MSLT) offers objective testing of daytime sleepiness which is useful in cases of suspected narcolepsy.
Actigraphy is a recording from a wrist-like device which has an accelerometer which estimates rest–wake cycles.
Clinical vignettes
We will now outline two interesting clinical vignettes to work through and consider how you would manage them.
Case 1
Presenting complaint (PC): Caitlyn is a 9-year-old girl who has cerebral palsy, epilepsy (focal and generalised seizures), visual impairment, hydrocephalus and significant learning disability (LD) secondary to prematurity. In the daytime she sometimes displays challenging behaviour including head banging.
History of presenting complaint (HPC): She has a history of frequent night waking, short sleep duration and daytime naps. Caitlyn’s bedtime (BT) is 20:30 and she falls asleep independently within 10 min. However, she wakes up to seven times a night. She repeatedly tries to get into her parent’s bed or wanders around the house. If the door is closed she bangs it, head butts or kicks her door. Her estimated total sleep, as well as mum’s, is 4 hours per night. There is no history suggestive of snoring, apnoea or reflux, no confusional arousals, bruxism or leg pain.
Social: Mum’s sleep is severely disturbed and there are concerns about her mental and emotional well-being due to prolonged severe sleep deprivation, the family is going into crisis.
Q1. Which sleep disorders might you need to consider? (Think Brain, Breathing, Behaviour). (Answer: A, B, C, D)
Central apnoea
Obstructive sleep apnoea
Behavioural insomnia
Restless legs syndrome
Circadian rhythm disorder
Narcolepsy or other central cause of hypersomnolence
Answer: Apnoea should be considered in children and young people with severe disability. These may be central events related to underlying brain malformation. Certain developmental diagnoses predispose to the child having obstructive events. The main differential is behavioural insomnia. Restless legs syndrome (RLS) is a compelling feeling to move legs; associated with sensory symptoms, for example, skin crawling, itching (difficult for a child to describe), this should be screened for. However, as she is non-verbal she is unable to report symptoms so often caregivers are asked about general restlessness. Prevalence in the general population is 5%–25%.12 13 In some groups with special needs up to 30%–50% can have reported restlessness and screening for low ferritin, which is thought to be linked is often undertaken and low values <50 μg/L treated based on research on RLS.14 The daytime naps may be due to insufficient sleep overnight. They could also be related to her anticonvulsant medication or seizures.
Q2. What sleep tests might be useful? (Answer: C, E, F)
Oximetry
Respiratory Polygraphy
Polysomnography
Multiple sleep latency test
Visual sleep diary
Actigraphy
Answer: A visual sleep diary is likely to be useful in the first instance if there is no access to lab-based sleep investigations (eg, American Academy of Sleep Medicine diary). Actigraphy can be additive, this gives more information but is not essential to be able to make a diagnosis. Due to the frequency of the night wakings it would be reasonable to look for triggers using polysomnography. This will rule out central apnoea and restless legs, and quantify the number of arousals as well as delineate sleep architecture.
Caitlin had polysomnography, which showed fragmented sleep with some leg movements with frequent arousals, no evidence of sleep-disordered breathing. Ferritin was <50 μcg/L and Caitlin was commenced on iron supplementation.
Q3. How would you interpret this sleep diary (figure 1)? What clues can you get from it? (Answer: see text)
Answer:
Total sleep time (TST): Count the number of shaded squares per night and divide by the number of nights = 5.5 hours.
Average BT: On average, at what time has family entered B for Bedtime on the sleep diary? Consistent or irregular? BT is Consistent at 20:30.
Sleep latency (SL): What is the time between the straight line ‘I’ entered for Bedtime on diary? <30 min.
Time in bed (TIB): Is there a big difference between the time the patient goes to sleep and lies in bed and the actual amount of time sleep = 7.5 hours.
Night waking: Count the number of blank squares or half squares over the sleep period that represent either a full hour of night waking or part of an hour (number of night waking average =1-3x prolonged wakings per night).
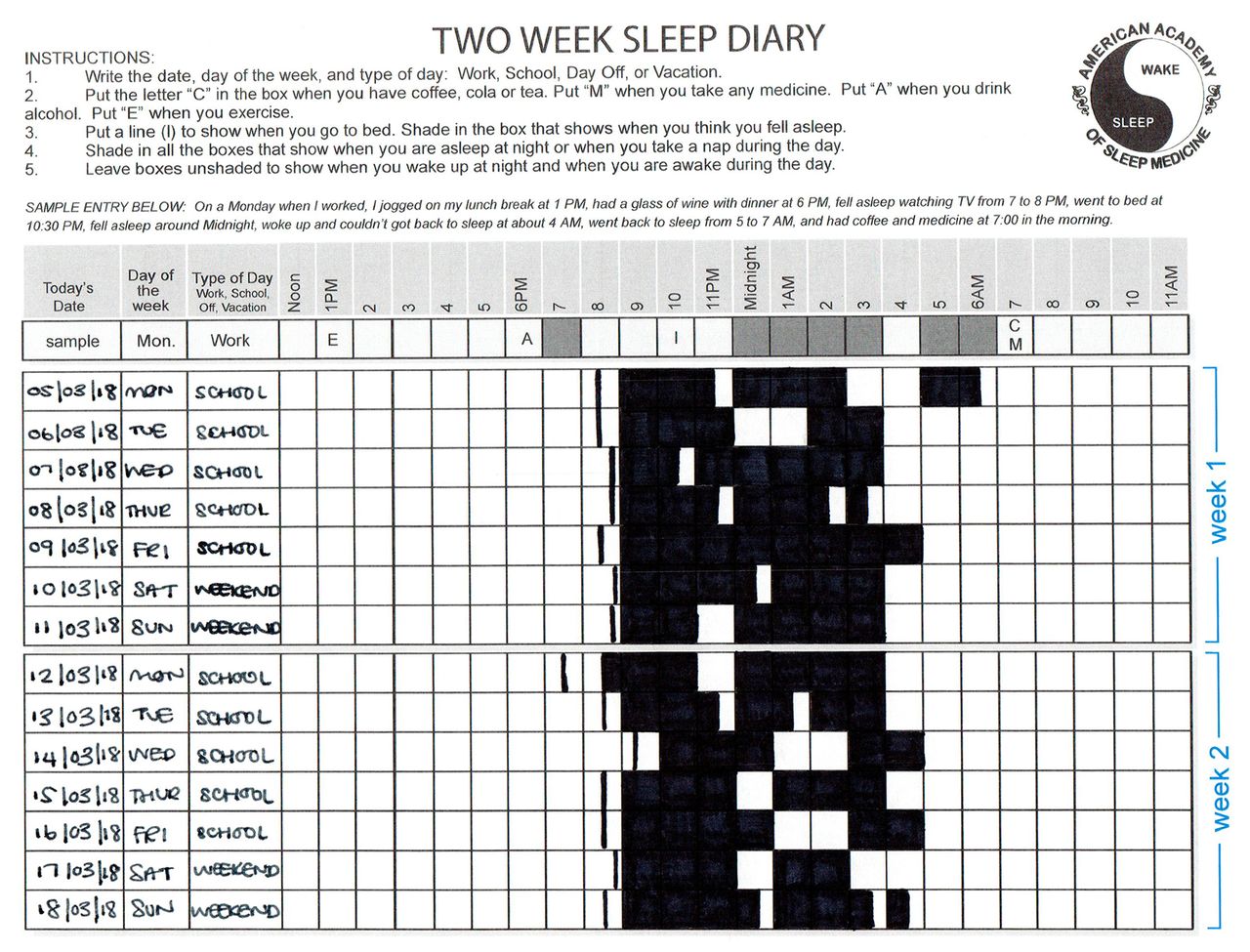
Sleep diary for case 1–Caitlyn.
Q4. What should be considered next? (Answer: A, B, E)
Behavioural intervention
Alimemazine
Chloral hydrate
Melatonin
Clonidine
Answer: In managing sleep difficulties behavioural intervention should always be the first port of call. It should be instigated ideally before medication is considered depending on the severity of the sleep disturbance but should always be addressed. We have outlined some behavioural strategies in box 3.
Behavioural sleep interventions
For children with learning disability increasing social cues and using sensory sleep signals may help.
The key is always to aim for self-soothing at the beginning of the night and then to extend to night wakings.
White noise and pink noise apps; pillow with iPod-type devices all allow sound to be played throughout the night as a sleep signaller.
Aromatherapy oils such as Bergamot and Lavender can be helpful.
Using an object of reference (eg, placing a teddy sprayed with mum’s perfume or using a pair of dad’s old pyjamas) may help if there are sleep association difficulties and cosleeping. Families can use techniques such as gradual extinction/withdrawal to help with night-time separation.
There are night-time indicator clocks such as Gro-Clock or products such as a sunrise lamp available on the market. These can be used in conjunction with a reward system such as a bedtime passport to help the child self-settle after a natural night waking and indicate when it is okay to get up.
A final consideration is a bed adaptation such as a safe space or Creative Care sleep pod, which are made by specialist manufacturers and may be funded by charity with referral from a disabled social service occupational therapist.
Our approach and treatment: Initially melatonin was tried. She was however able to fall asleep quickly independently and so may not have been indicated in the first instance (see box 4). In this case, high-dose alimemazine (an antihistamine) was prescribed due to the frequent night waking. This decision was made in the circumstance as the family had gone into crisis. Mum was asked to see her general practitioner (GP) and seek urgent help. Promethazine can be used as an alternative. Night sedation should be used as an emergency in the short term only, used with caution while other sleep solutions are explored and primarily in children with severe disability not in typically developing children. Clonidine is a medium-term medication for this degree of night waking at very low dose for children with significant disability, however there is possibility of build-up of tolerance so other support is needed (behavioural) in conjunction. Use of clonidine is outlined in box 5.
Melatonin
Melatonin (N-acetyl-5-methoxytryptamine) is the primary hormone produced by the pineal gland during nocturnal periods in response to darkness, to properly time circadian sleep/wake rhythms and enhance sleepiness. It is available in a prolonged release preparation.
Melatonin prescribing should be limited to those who have a confirmed diagnosis of insomnia. It is best to avoid prescribing for children mid-assessment who do not have a proven neurodisability condition that would imply abnormal melatonin production. These are conditions that should be considered early on. This may include children with:
Cortical blindness.
Midline brain defects such as septo-optic dysplasia or pituitary tumours.
Neurodegenerative disorders.
Hypoxic ischaemic encephalopathy.
Acquired brain injury.
(Adapted from Northamptonshire Prescribing Advisory Group Sleep Disorders Guideline 2013)
In addition, melatonin may be helpful in treating delayed sleep onset in autism (if assessed as not being bedtime resistance) after appropriate behavioural intervention. There are new preparations coming to market especially for autism with longer action such as Neurim which may have benefit maintaining sleep.18
Sleep hygiene, environmental factors and behavioural measures should be considered and changes implemented prior to prescribing. Regular monitoring with the use of sleep diaries should occur prior to and following the commencement of therapy.
Treatment should be established at the lowest effective dose. Commence at 2 mg once daily (20 min before current bedtime). This can be moved earlier once bedtime routine established. Avoid dose escalations without objective measures. It is important to engage in regular monitoring while child is on melatonin should occur with trials off medication. For some children, withdrawal is not successful and treatment may be necessary for the longer term.
Melatonin is widely used as a medication to aid sleep. An evidence summary published by the National Institute for Health and Care Excellence (NICE) showed that a considerable amount was spent on melatonin preparations. Double-blinded randomised placebo-controlled phase III trial showed that children gained little additional sleep on melatonin; though they fell asleep significantly faster, waking times became earlier. Family function and parent quality of life also improved. Child behaviour and family functioning outcomes did not significantly improve. Cost benefit should be considered and local spend may be used to help support business case development for local sleep services including increased access to trained sleep practitioners.
Clonidine and other medication choices
Clonidine is a central alpha2-adrenergic receptor agonist, with a half-life of 6–24 hours. Onset of action is within 1 hour, with peak effects at 2–4 hours. It has been considered to act mainly on the autoreceptors of presynaptic noradrenergic neurons to reduce their release of norepinephrine. The mechanism of action for sedation is not clear. There is little evidence in literature regarding its efficacy, however it continues to be widely used for treatment of sleep disorders in children with neurodevelopmental disorder (NDD).
Examples of dosing for older school aged children with cognitive impairment:
Clonidine 25 mcg orally at night for 1 week.
Clonidine 50 mcg at night for 1 week.
Clonidine 75 mcg orally at night to continue.
Can go up from 25 mcg aliquots per week to 125 or 150 mcg.
Stay on lowest effective dose.
Local team to monitor blood pressure and weight and height:
Again this should be reserved for children with disability (normally non-verbal/limited mobility) and not for typical developing children.
Other medication options:
Further medications for use in disability include trazodone (in Angelman syndrome) and low-dose gabapentin in children with significant epilepsy (both with specialist advice from a tertiary sleep centre). Other medications such as clonazepam for parasomnia/night terrors.
For smaller children doses range from 10-70 mcg.
Q5. Are there any other alternatives for children with disability to help with frequent night wakings or early morning wakings?
Answer: In some cases the level of challenging behaviour is significant enough that it warrants treatment from: specialist LD health visiting/nursing team in first instance or to Child and Adolescent Mental Health Services (CAMHS). These will need to be worked on at the same time, as sleep is addressed. It is helpful if members of LD teams have some training in sleep and disability (see box 1).
Outcome: We used alimemazine to stabilise sleep and to allow sleep training and the addition of a safe sleeping space resulted in Caitlyn having a much improved sleep pattern (11–12 hours) and brought the family back from crisis.
Case 2
John is a 15-year-old boy with an underlying diagnosis of Autism Spectrum Disorder with secondary social anxiety.
PC: John has a disturbed sleep pattern described by his mother as ‘moving around the clock’. His anxiety is so severe that he was unable to leave the house to attend appointments regularly and also has been having problems attending school.
HPC: John has had difficulty maintaining a normal sleep routine for 4 years. This was following a traumatic incident in school that he ‘put himself to bed’ in order to avoid schooling. This initial picture of school avoidance evolved to a disturbed pattern of sleep. John is sleeping approximately 10 hours a day but can fall asleep at different times. When he is asleep he is reportedly very difficult to wake. He does not describe excessive sleepiness during waking hours and no unusual arousals or night terrors were reported.
Medications: A trial of melatonin is initially reported to have some improvement but has no long-term effect. Sertraline is commenced for mood and anxiety.
Social: John lives with his mother and elder sister. He has not attended school in 2 years due to sleep difficulties. There has been social work involvement and the threat of legal action due to school refusal. This causes high levels of anxiety for both John and his mother. His mother thinks no one is listening to her concerns.
Q1. What are the possible diagnoses? (Answer: H, I)
Tick all that apply:
Insomnia (adult type)
Behavioural Insomnia
Sleep-related movement disorder
Obstructive sleep apnoea
Partial arousal parasomnia
Restless syndrome
Central disorder of hypersomnolence
Circadian rhythm disorder
No sleep disorder—social anxiety and behavioural school refusal
Answer: The top differential is a circadian rhythm disorder (see box 6). The striking aspect of the history is the description of his sleep onset moving ‘round the clock’. However, a disruption of circadian rhythm should be considered in young people with autism without language disorder (Asperger phenotype).15 This is due to a documented weaker association between sleep–wake cycles and external cues or zeitgebers in autism. We should also consider OSA and RLS. Adult-type insomnia is associated with conditions such as anxiety disorder. His social anxiety and school refusal are significant factors that needed to be addressed.
Circadian rhythm disorder
Your circadian rhythm is a 24-hour internal clock that is running in the background of your brain and cycles between sleepiness and alertness at regular intervals. The term circadian comes from Latin words that literally mean ‘around the day’. Our sleep–wake cycle is only one expression of the circadian rhythm, which dictates all our body physiology. Our circadian rhythms are synchronised by environmental cues called zeitgebers with the most powerful cue being exposure to light and dark (facilitated by pineal gland production of melatonin in total darkness). Circadian rhythm disorders are disruptions in a person’s circadian rhythm. In this case, anxiety and possibly a degree of avoidant behaviour with lack of regular social and environmental cues contributed to the development of delayed sleep–wake phase disorder. Sleep times can be out of alignment leading to difficulty engaging with routine activities expected to occur at certain times such as work and school and with social activities.
Q2. What investigations would be useful? Tick all that apply. (Answer: A, C)
Visual sleep diary
Written sleep diary
Actigraphy
Polysomnography
Multiple sleep latency test
Overnight video recording
Answer: At this stage, polysomnography would not be very helpful (he reportedly sleeps through although his BTs and wake times ‘move round the clock’) though it may be necessary in the future. The initial investigation of choice is actigraphy or a visual sleep diary (if actigraphy is not available). This will allow delineation of a possible circadian rhythm disturbance and will help pinpoint a diagnosis simply and quickly.
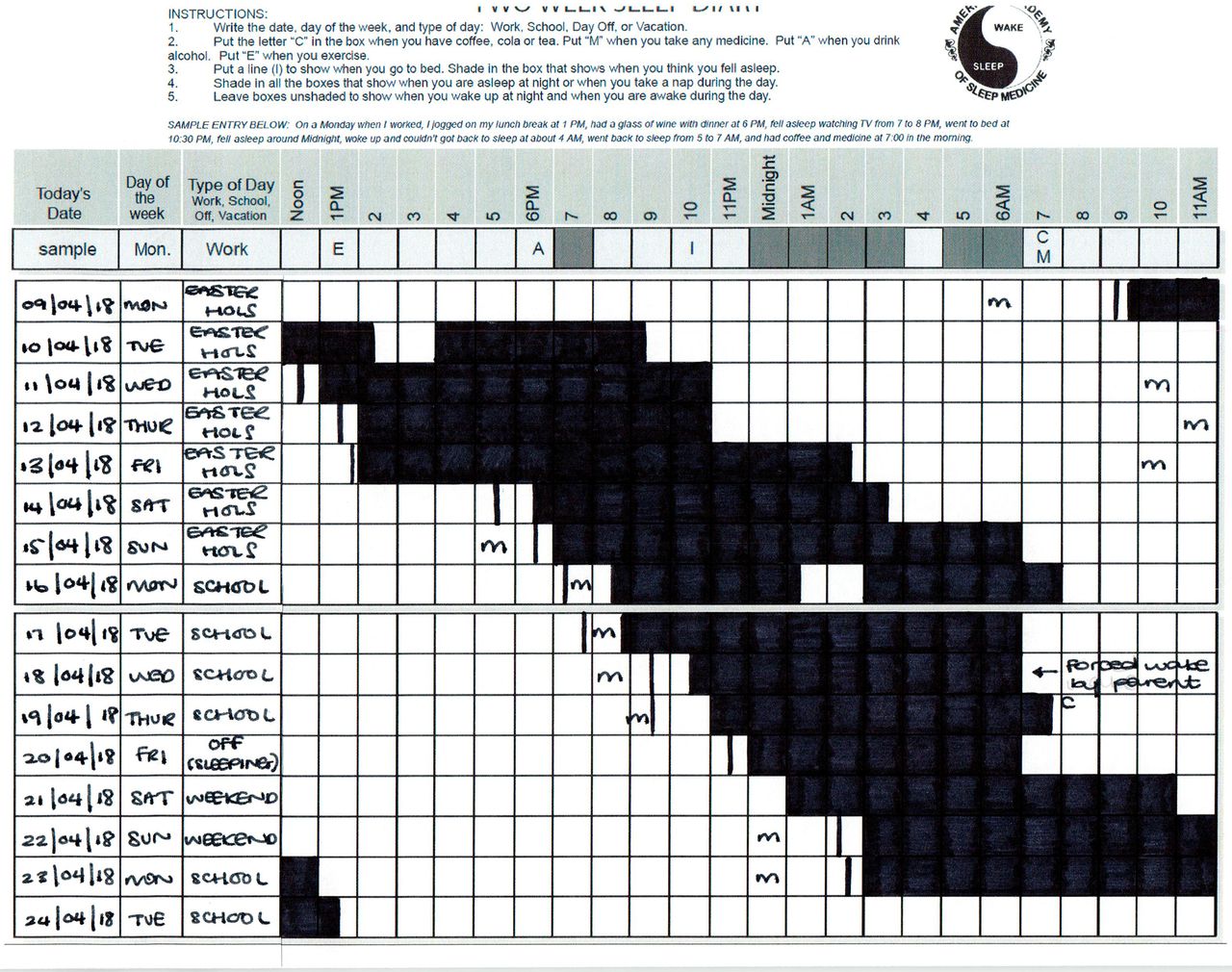
Q3. How would you interpret this sleep diary (figure 2)? What clues can you get from it? (Answer: see text)
Answer:
TST: 8.5 hours.
BT: Irregular BT 13:30–10:10.
SL: <30 min.
TIB: 10.5 hours.
Night waking: Number of night wakings average = 1 per night.
{kind=link}
{kind=link}
Sleep diary for case 2–John.
Q4. What should be considered next? (Answer: A, D)
Behavioural intervention
Alimemazine
Chloral hydrate
Melatonin
Clonidine
Our approach: The debilitating aspect of his sleep problem was non-school attendance with accompanying comorbidity of social anxiety. His mother had tried against considerable odds to get him back into education and the diagnosis of a circadian rhythm disturbance helped move things forward in terms of liaison with local teams. The key intervention was engagement with school with a planned staged return to education, and support for home curriculum in subjects or activities of interest. The treatment for this case had to be planned in advance with the aim to move wake activities at time when the family had the resilience to participate and at a speed that was acceptable to them. Supporting the young person and the main carer/parent was paramount. There was potential for psychological work to explore systemic factors contributing to presentation, as well as motivational interviewing to explore goals and whether change is currently a realistic expectation.
Treatment: The family was offered access to sleep psychology to formulate a sleep schedule. The sleep team worked with other professionals and worked to plan graded return to school with psychoeducation about his sleep difficulty. CAMHS support regarding anxiety was given. Care needed to be taken regarding pressure on the family, which may contribute further to withdrawal and anxiety. The young person and the carer remained central to the process. The last intervention that was considered was the use of melatonin and a light source once sleep schedule was established to stabilise it.
Outcome: Ongoing involvement was key for psychiatric treatment regarding social anxiety and coordination with his local teams via a multidisciplinary team around the child meetings. These interventions superseded any attempt to try to move his sleep ‘back round the clock’ with the secondary care physician emerging as the key member of the team.
Conclusion
Sleep difficulties are widespread in the paediatric population and most paediatricians do not feel confident in managing them. The Working Party on Sleep Physiology and Respiratory Control Disorders in Childhood published the Standards for Services for Children with Disorders of Sleep Physiology report,16 outlined a hub and spoke design for management of sleep disorders but access remains variable. This means the local team, which includes paediatricians, GPs, health visitors and schoolteachers, need to be empowered to identify and manage sleep disorders.
Of just under 200 hospitals in the UK who see children with complex needs (tertiary and secondary care), around only eight labs routinely conduct complex (neurological) sleep investigations (British Paediatric Sleep Association, unpublished data). As access is variable and sleep difficulties are widespread it is important to improve overall education and confidence in identification and management of sleep disorders.
Our key message is always consider a sleep disorder in children and young people with neurodisability. The importance of taking an adequate history cannot be overemphasised. From the history and with an understanding of the underlying condition, the child has your assessment and management can be tailored. The modification of environmental and sleep hygiene issues should be considered first and will be the mainstay of treatment. Educating and supporting parents with anxiety and exhaustion around the issues is of paramount importance. Access to psychological and behavioural interventions is a key part of treatment success and medication should only be used in conjunction with these methods. Non-judicious use of medication is costly to the National Health Service. The coordinating role of the local team is vital. In improving first-line care and management it becomes clear which cases are indeed more complex and require specialist investigation and input from a tertiary sleep disorders unit. Management of sleep can improve the quality of life for both family and the child. We will end with a quote from Caitlin’s Mother:
Without the help and support of the specialist sleep team the outcome would have been completely different. We have been able to keep Caitlyn at home as local authority wanted to move her to respite. This has been extremely important for the family. She is a lot happier. Sleep has improved her overall well-being. Her learning has improved and now I have my family back.
Acknowledgments
We thank the parents of patients used as case studies, sleep physiologists Joshua Piper and Ebrahim Patel who assisted with sleep investigations, Professor Paul Gringras and Dr Charlie Tyack for advice and support. There was no patient or public involvement in the research survey element of this paper as it focused on physician knowledge.
References
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Parental/guardian consent obtained.
Provenance and peer review Commissioned; externally peer reviewed.