Article Text

Abstract
Objective To describe the diagnosis and treatment of patent ductus arteriosus (PDA) in infants born at <32 weeks’ gestational age (GA) in England and Wales between 2010 and 2017.
Study design Retrospective cohort study using routinely recorded data from the National Neonatal Research Database of infants born at <32 weeks admitted to neonatal units in England and Wales from 2010 to 2017.
Results Among 58 108 infants born at <32 weeks’ GA, 28.3% (n=16 440) had a PDA diagnosed clinically or with echocardiographic confirmation. Of these, 34.8% (n=5721; 9.8% of total <32 weeks’ infants included) had PDA treatment including 7.6% (n=1255) with indomethacin, 23.5% (n=3857) with ibuprofen and 5.6% (n=916) with surgical closure. The highest incidence of PDA was among infants born at 24 and 25 weeks’ GA (70.2% and 70.8%, respectively), decreasing to 6.1% among infants born at 31 weeks’ GA. The percentage of infants with a PDA increased over the study period (25.5% in 2010 to 28.5% in 2017). The percentage of infants who received ibuprofen or indomethacin or had PDA surgery decreased from 41.3% in 2010 to 33.7% in 2017, with an increase in use of ibuprofen from 20.2% to 27.3% while use of indomethacin decreased from 20.0% to 8.8%. Surgical closure of PDA decreased from 9.1% to 3.0%. Indomethacin was used for median (IQR) 3 (2–5) days while ibuprofen was given for 3 (2-4) days, at a median of 8 and 10 days after birth, respectively; surgical treatment was used later at 33 (24–45) days after birth.
Conclusions Ibuprofen is the preferred drug and surgical interventions are becoming less frequent for PDA closure among very preterm infants in England and Wales.
Trial registration number NCT03773289.
- Neonatology
- Epidemiology
- Pharmacology
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Optimal management of patent ductus arteriosus (PDA) in very preterm infants remains a clinical controversy in neonatal practice.
Rates of treatment and choice of drugs and surgical closure vary between neonatal units.
What this study adds
In England and Wales, between 2010 and 2017, 28% of very preterm infants had a PDA.
Among those who had a PDA, 35% received PDA-specific treatment. The percentage of infants receiving PDA-specific treatment decreased from 41.3% in 2010 to 33.7% in 2017.
The percentage of infants treated with ibuprofen has increased but those treated with indomethacin or undergoing surgical closure has decreased with an overall decrease in percentage of infants who received indomethacin/ibuprofen or had PDA surgery from 41% to 34%.
Introduction
Optimal management of patent ductus arteriosus (PDA) in preterm infants remains an unresolved controversy.1 Impaired haemodynamics due to persistent PDA is associated with adverse outcomes.2 Large left-to-right shunt with pulmonary over circulation and diastolic steal of systemic blood flow can affect cerebral, gut and renal perfusion and is associated with risk of adverse outcomes such as bronchopulmonary dysplasia (BPD), intraventricular haemorrhages (IVH) and necrotising enterocolitis (NEC).3 PDA closure may be induced by medical and/or surgical interventions. Pharmacological treatment of PDA includes inducing closure with prostaglandin inhibitors, of which indomethacin and ibuprofen are the most widely used agents.1 Additionally, paracetamol has emerged as an alternative, with evidence to suggest it may be as efficacious as indomethacin or ibuprofen in inducing ductal closure.4
Despite evidence that interventions are effective in inducing PDA closure, management strategies are evolving with greater acceptance of conservative management or no treatment because of accumulating evidence that inducing PDA closure does not improve outcomes. Randomised controlled trials (RCTs) show that routine early treatment does not reduce PDA ligation or risk of adverse clinical outcomes and may be associated with higher rates of adverse events.5 A network meta-analysis with 68 RCTs including 4802 infants showed that despite ranking the worst in terms of PDA closure, no treatment was not associated with significantly higher odds of death, NEC, or IVH.6 Similarly, although surgical closure can be achieved by ligation or transcatheter occlusion and is associated with reduced mortality, surviving infants have increased risk of neurodevelopmental impairment.1
These uncertainties lead to wide variations in practice.7 In a retrospective study of Canadian practice, Lokku et al reported that from 2006 to 2012 the rate of both pharmacotherapy and surgical ligation of PDA decreased.8 In a larger international study of PDA treatment rates across 139 neonatal units, Isayama et al, reported overall treatment rates ranging from 36% in Israel to 52% in Japan (ranging from 13% to 77% among the included neonatal units) for very low birth weight infants (<1500 g birth weight) who survived at least 3 days after birth.9 In this study, we aim to describe the use of PDA treatments in infants born at <32 weeks’ gestational age (GA) in England and Wales and the change in prevalence of use of pharmacological agents and surgery from 2010 to 2017.
Methods
The National Neonatal Research Database (NNRD) records data of admissions to the 200 neonatal units in the UK Neonatal Collaborative. Infants born <32 weeks’ GA who were admitted to a neonatal unit in England and Wales from 2010 to 2017, whose data are held in the NNRD, were included. We excluded infants if they were missing data on sex, birth weight, month of birth, or one or more days or episodes of care, were a late admission (>24 hours after birth) or had an extreme birth weight for GA (Z-score ≥+4 SD or ≤ −4SD). We extracted records of a diagnosis of PDA by searching the ‘principal diagnosis at admission’, ‘daily diagnoses’ and ‘diagnoses at discharge’ fields. Records of treatment for PDA were identified from the ‘daily drugs’ field and in the specific field for PDA treatment. We did not have sufficient information to determine how the PDA was diagnosed that is, whether the diagnosis was confirmed by an echocardiogram or made based on clinical signs and symptoms only. We created indicator variables for each day of care to show whether an infant was prescribed indomethacin, ibuprofen, and/or paracetamol, or received PDA surgery. Some infants, particularly in the first 3 years of the study period, had treatment for PDA recorded but did not have a recorded diagnosis. Given the specificity of treatment with indomethacin, ibuprofen and surgery, infants with these treatments recorded were deemed to have PDA even in the absence of a recorded diagnosis. We did not take prescription of paracetamol alone as indicative of PDA given that this is also, frequently, used for other indications.
We performed data management and analysis using STATA V.16.0 (Stata) with descriptive statistics to describe and compare the characteristics and clinical outcomes of infants with and without PDA. We plotted graphically the prevalence of diagnosis of PDA, and prevalence of use of pharmacological and surgical treatment, by GA at birth in completed weeks and by year of admission. For infants with PDA, we described the timing and duration of pharmacological and surgical treatment. Finally, we used multivariable logistic regression to compare the characteristics of infants diagnosed with PDA who did and did not receive treatment (indomethacin and/or ibuprofen and/or surgery), adjusting for sex, GA at birth (completed weeks) and birth weight-for-GA z-score (<-2SD vs ≥−2SD). Given uncertainty about the indication for paracetamol use, infants with PDA whose only treatment was paracetamol were classified as untreated. In a sensitivity analysis, we excluded these infants from the comparison and conducted a comparison between those who received treatment with indomethacin and/or ibuprofen and/or surgery and those who had no treatment excluding those who had treatment with paracetamol only.
Results
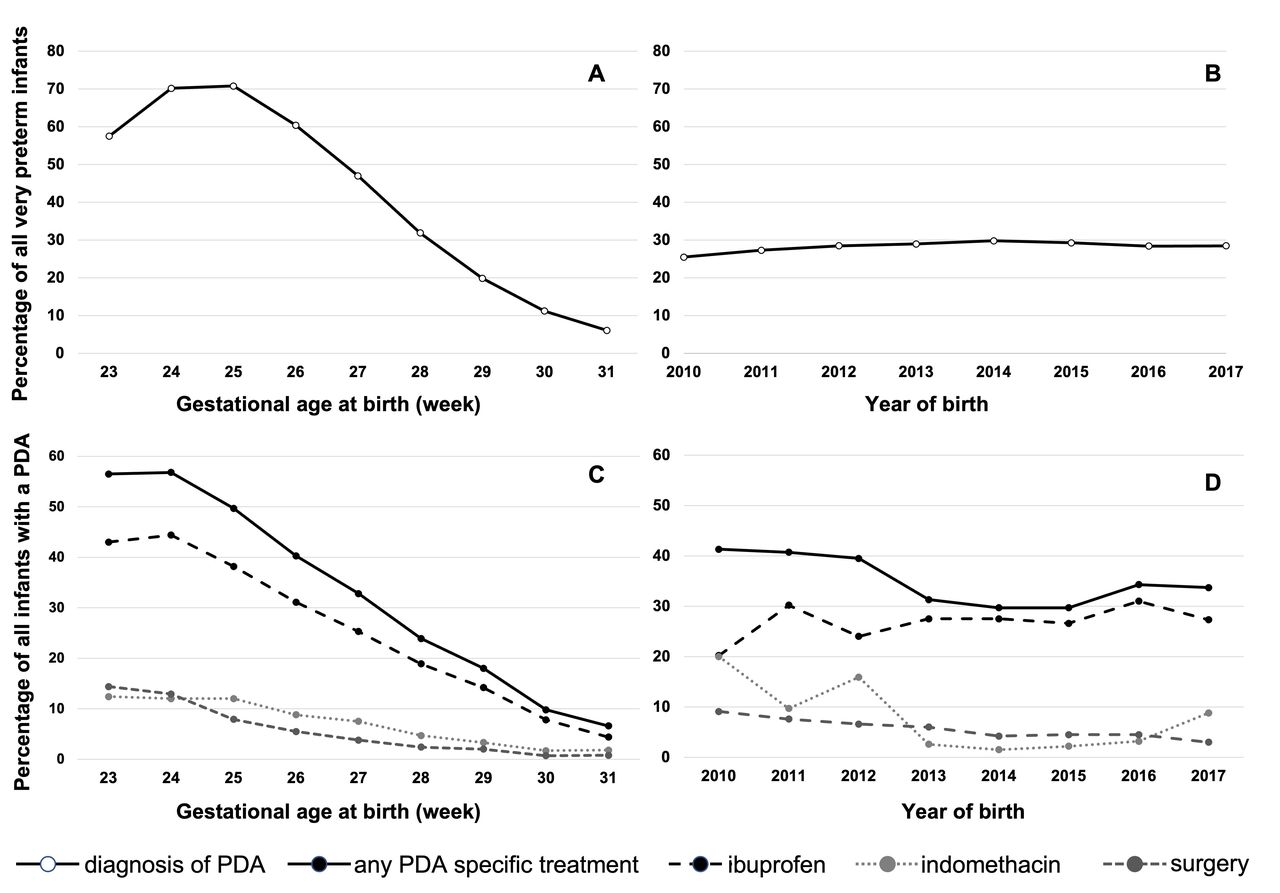
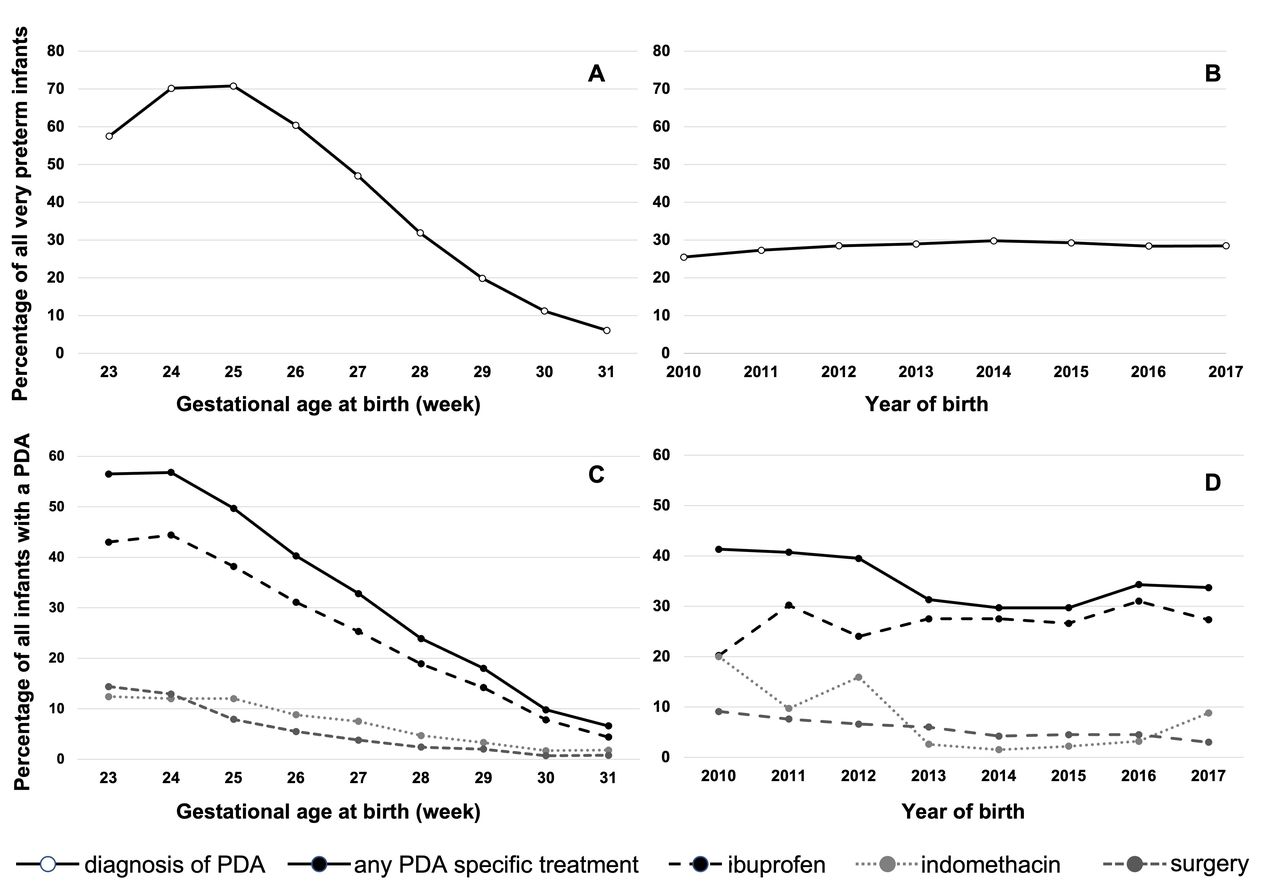
The initial dataset included information on 61 919 infants born at <32 weeks’ GA who were admitted to a neonatal unit in England and Wales from 2010 to 2017. After exclusions, 58 108 were retained for analysis. Of these, 28.3% (n=16 440) were deemed to have PDA, having either a recorded diagnosis and/or a record of a PDA-specific treatment (indomethacin and/or ibuprofen and/or underwent PDA surgery). Figure 1A,B shows the percentage of all very preterm infants who were deemed to have a PDA by GA week at birth and year of birth, respectively. Highest percentages of infants with a diagnosis of PDA were among those born at 24 weeks’ (70.2%) and 25 weeks’ (70.5%) GAs reducing to 6.1% of 31 week infants. There was an increase in the percentage of infants with a PDA from 25.5% in 2010 to 28.5% in 2017.
{kind=link}
(A, B) Prevalence of diagnosis of patent ductus arteriosus (PDA) in infants born at <32 weeks' gestation in England and Wales from 2010 to 2017 by gestational age in completed weeks at birth (A) and by year of birth (B). (C, D) Treatment of PDA in infants born at <32 weeks’ gestation in England and Wales from 2010 to 2017 by gestational age in completed weeks at birth (C) and by year of birth (D). The denominator for PDA prevalence is the total number of infants included in the study. The denominator for percentage of infants who received the drugs/surgery is the total of number of infants who had a PDA. Please note that the scale of the y-axis changes between (A/B) and (C/D).
Table 1 describes and compares the characteristics and clinical outcomes of infants with and without PDA. Infants with PDA were more likely to be female, were born earlier, had a lower birth weight and lower birth weight-for-age z-score and longer length of stay compared with infants without PDA. After adjustment for GA at birth, sex and birth weight z-score, infants with PDA had higher odds of BPD, NEC and late onset sepsis, but a reduced odds of death before discharge. Although the percentage of infants who died before discharge was higher among those who had a PDA (11.6%) than among those who did not have a PDA (8.3%), after adjustment for confounders, the odds of death were reduced in the group that had PDA (adjusted OR, aOR (95% CI), 0.30 (0.27 to 0.32). This may be because of adjusting for GA at birth. Among infants born at 24- and 25 weeks’ GA, 70% had a PDA and 40% died while at the other end, at 31 weeks’ GA, 6% had a PDA and <2% died. After accounting for the high risk of death at the lower GAs and other confounders, a diagnosis of was PDA was associated with a lower adjusted odds of death before discharge.
Characteristics and outcomes of infants born at <32 weeks’ gestational age in England and Wales from 2010 to 2017 with and without a patent ductus arteriosus (PDA)
Tables 2 and 3 show the comparisons between infants who were deemed to have a PDA with those who did not by GA subgroups (<28 weeks’ GA and 28–31 weeks’ GA, respectively). Among extremely preterm infants (<28 weeks’ GA), 34.5% (n=2447/7083) died in the group that did not have a PDA while 15.6% (n=1625/10 418) died among those who had a PDA and the latter group had lower adjusted odds of death (aOR (95% CI), 0.21 (0.19 to 0.23).
Characteristics and outcomes of infants born at <28 weeks’ gestational age in England and Wales from 2010 to 2017 with and without a patent ductus arteriosus (PDA)
Characteristics and outcomes of infants born at 28–31 weeks’ gestational age in England and Wales from 2010 to 2017 with and without a patent ductus arteriosus (PDA)
Of the 16 440 infants with PDA, 34.8% (n=5721; 9.8% of total <32 weeks’ infants included) received a PDA-specific treatment (indomethacin and/or ibuprofen and/or surgery) decreasing from 41.3% in 2010 to 33.7% in 2017. Including those who received paracetamol, 48.2% (n=7930; 12.7% of total <32 weeks’ infants included) received treatment.
Among the infants with a PDA, 26.9% (n=4428) of infants received ibuprofen, 7.6% (n=1255) indomethacin, and 23.5% (3857) paracetamol (table 4). 5.6% (n=916) of infants were recorded to have undergone PDA surgery. The majority of these (70%, n=641) received one or more pharmacological treatments prior to surgery. Figure 1A shows the prevalence of diagnosis and treatment of PDA from 2010 to 2017 by GA at birth in completed weeks. PDA was more frequent in infants of lower GA with 70.2% of 24 weeks’ GA infants and 70.8% of 25 weeks’ infant having a PDA. The incidence reduced to 6.1% among infants born at 31 weeks’ GA.
Timing and duration of treatment for PDA among infants born at <32 weeks’ gestational age in England and Wales from 2010 to 2017
Figure 1C,D represents treatment by GA week at birth and by year of birth, respectively. It shows that the overall percentage of infants who received any treatment (ibuprofen and/or indomethacin and/or surgery) decreased from 41.3% in 2010 to 33.7% in 2017. In the same period, the use of ibuprofen increased from 20.2% to 27.3% while use of indomethacin decreased from 20.0% to 8.8%. Surgical closure of PDA decreased from 9.1% to 3.0%.
Table 4 describes the timing and duration of treatment for PDA. All three pharmacological treatments were used for a median of 3 days. The day after birth and postmenstrual age when the drug was first prescribed was much later for paracetamol compared with ibuprofen and indomethacin.
The characteristics and clinical outcomes of infants with PDA who were treated and those who were not treated with indomethacin and/or ibuprofen, and/or surgery are described and compared in table 5. Infants with PDA who received treatment were less likely to be female, were born earlier, had a lower birth weight and lower birth weight-for-age z-score and longer length of stay compared with infants with PDA who were not treated. After adjustment for GA at birth, sex and birth weight z-score, infants who were treated had higher odds of BPD and late onset sepsis, but a reduced odds of NEC and death before discharge.
Infants born at <32 weeks’ gestational age with a patent ductus arteriosus (PDA) who received treatment vs those who did not in England and Wales from 2010 to 2017
Tables 6 and 7 show the comparisons between infants who were treated and those who were not treated with indomethacin and/or ibuprofen, and/or surgery by GA subgroups (<28 weeks’ GA and 28–31 weeks’ GA, respectively). Among the extremely preterm infants (born at <28 weeks’ GA), the adjusted odds of BPD and late onset sepsis were higher while the adjusted odds of NEC and death before discharge was lower among those who were treated.
Infants born at <28 weeks’ gestational age with a PDA who received treatment vs those who did not in England and Wales from 2010 to 2017
Infants born at 28–31 weeks’ gestational age with a PDA who received treatment vs those who did not in England and Wales from 2010 to 2017
In the above analyses, among the infants in the group that was designated as not having received PDA treatment, there were 2209 infants who had received at least one dose of paracetamol sometime during their care. It is possible that some of this may have been for treating PDA. Therefore, we performed a sensitivity analysis where infants who only received paracetamol were excluded. The results were similar except that more treated infants had NEC (n=433/5721, 7.6%) when compared with those who were not treated (n=334/88510, 3.9%) giving a higher adjusted odds of NEC in the treated group (aOR 1.25, 95% CI 1.07 to 1.47).
Discussion
In England and Wales, between 2010 and 2017, 28% of very preterm infants were diagnosed to have a PDA and, of them, over one-third were treated with ibuprofen, indomethacin, and/or surgical closure.
Infants who had a PDA and survived to discharge had worse clinical outcomes with higher adjusted odds of BPD, NEC, IVH and late onset sepsis as compared with those who did not have a PDA. Delayed closure of the ductus is known to be associated with adverse outcomes including prolongation of need for respiratory support, BPD, pulmonary haemorrhage NEC, IVH, periventricular leukomalacia and cerebral palsy.2 However, it is not established whether these adversities are the direct consequences of haemodynamic instability due to the patent duct and moreover, if inducing ductal closure can prevent or reduce the risk of occurrence or severity of these common complications of prematurity.2
Echocardiography is not routinely performed on all very preterm infants in the UK. We did not have the information to determine how the diagnosis was established. Infants with a PDA that was haemodynamically insignificant and was not treated may not have the diagnosis entered in the database. A diagnosis of PDA is more likely to have been recorded in the database for those infants who had clinical features of PDA and/or had an echocardiography. Such infants may have been more unwell and at a higher risk of the other morbidities and of dying as compared with those who had asymptomatic PDAs that were not evident on clinical assessment and were therefore not recorded as a diagnosis. We found that a higher percentage of infants who had a PDA died before discharge however, after adjusting for confounders the odds of death was lower in the group that had a PDA. This reversal of the direction of the link between PDA and death before discharge was seen after adjustment for GA. Infants born at the lowest GA weeks’ have the highest incidence of PDA and also have the highest mortality risk. In the subgroup analysis including only the extremely preterm infants, we found that the percentage who died was significantly higher in the group that did not have a PDA and the adjusted odds of death remained statistically significantly higher in that group even after adjustment for GA. We did not exclude early deaths and infants who survived were more likely to have undergone a clinical or echocardiographic evaluation resulting in a diagnosis of PDA as compared with those who did not live long enough for such a diagnosis to be made. We have reported similar confounding in other reports10 and such survival bias is a recognised limitation of observational studies particularly in a population such as extremely preterm infants where there is a high risk of early deaths.
Overall, ibuprofen was the most frequently chosen pharmacological agent for PDA closure. In 2011, indomethacin and ibuprofen were used in similar numbers of infants with PDA. Over the study period, use of ibuprofen increased and that of indomethacin decreased such that ibuprofen was more than three times more frequently used as compared with indomethacin (27.3% vs 8.8%) in 2017. We analysed treatment with paracetamol separately. The NNRD does not include information on the indication of drug use and while indomethacin and ibuprofen are almost exclusively used for PDA closure, paracetamol may be prescribed for other indications. Similarly, it is possible that some use of indomethacin, particularly when given on the first day after birth, may have been for prevention of IVH and not following a PDA diagnosis although such treatment may then have reduced the possibility of the infant needing further treatment for PDA11 We found that the median first day of use of ibuprofen and indomethacin were 10 and 8 days after birth, respectively, when they may have been used for targeted closure of PDA, while the median first day of use of paracetamol was day 58. Although such later use of paracetamol may have been for PDA closure after other agents had failed, it is likely that this reflects use as analgesic-antipyretic coinciding with the first set of routine immunisations which occur around this time.
Infants who were treated were more likely to be boys, were more premature, smaller, and had lower birthweight-for-age z-scores. This is similar to other studies9 although Isayama et al found no difference in the percentage of male infants between the treated and untreated groups. When compared with those not treated, we found that those who were treated had higher adjusted odds of adverse clinical outcomes. This may again be a limitation of the observational design of our study that is, confounding by indication where sicker infants are more likely to be treated for their PDA and also more likely to experience the adverse outcomes. Evidence from meta-analyses of RCTs suggests no difference in such outcomes when comparing treatment with medications to conservative management.6 Lokku et al showed, in a Canadian cohort, that increase in conservative management of PDA was associated with reduction in a composite of adverse outcomes.8 Similarly, Okulu et al12 reported that in the cohort of 1193 infants born at 24 to 28 weeks’ gestation, 24% with echocardiographically confirmed moderate-to-large PDA were managed conservatively. Although they did not find any difference in the rates of BPD, infants who were treated had a higher rate of death (OR (95% CI), 1.82 (1.15 to 2.89) when compared with those who were not treated12 similar to our finding that the adjusted odds of death before discharge was lower among the infant with PDA who did not receive treatment, particularly among the extremely preterm infants (aOR (95% CI), 0.59 ((0.53 to 0.66)). The recent PDA-TOLERATE trial5 reported more deaths among those who received early routine treatment as compared with those who were treated conservatively although the difference was not statistically significant. Continuing the controversy, a multi-national study of association of PDA treatment with adverse outcomes showed that both high and low rates of PDA treatment were associated with death or severe neurological injury.9 In this study the overall treatment rate was 45% and authors found that adverse outcomes including death, severe neurological injury, and NEC were less common in the neonatal units that followed a moderate approach to PDA treatment.9
We found that among those with a PDA, 5.6% had surgical ligation at a mean age of 33 days. The majority (70%) of these infants had received previous pharmacological treatment. The recent British Paediatric Surveillance Unit study by Warnock et al showed that between September 2021 and September 2013, 263 infants underwent PDA surgery with inability to wean from respiratory support and haemodynamically significant PDA cited as the most common reasons for surgical intervention.13 Similar to our findings, the median age at surgical intervention was 33 days and 66% had received prior medical therapy. It should be noted that the group included in Warnock et al, are very likely a subset of the cohort included in our current study.
Although meta-analyses show that treating PDA does not improve important clinical outcomes, the continued high rates of clinicians opting for treating PDAs may result from the unresolved issues in this area. Most trials included in these meta-analyses allowed open-label rescue treatment in both groups, resulting in high rates of treatment (ranging from 26% to 85%)3 in those randomised to placebo/no treatment. Such contamination skews the estimated treatment effect towards the null hypothesis14 which means that results are more likely to show no difference between the two groups. This makes the final intention-to-treat analyses difficult to interpret and translate into clinical practice. Some argue that the preference for no treatment is the result of uncertainties about how to treat a PDA rather than evidence favouring no intervention.15
Our results represent use of pharmacological agents and surgical intervention for PDA among very preterm infants receiving newborn care in England and Wales. We acknowledge that the interpretations of the worse clinical outcomes among those who had a PDA compared with those who did not and those who were treated for a PDA and those who were not are treated are limited by the observational design and the biases mentioned above. Another limitation that we faced was that the information about the indication of drug use is not included in the NNRD. Although we have described the use of paracetamol and report an increase in its use during the study period, we were unable to include it in our analyses as paracetamol may have been used for its analgesic-antipyretic properties rather than as an agent to induce PDA closure. Infants who received PDA treatment with paracetamol only are therefore not represented in our analyses.
The optimal management of PDA remains an unanswered question even after numerous randomised trials, and systematic reviews.16 Despite the limitations of observational study design, real-world evidence from large clinical databases with longer term follow-up may be the most pragmatic and efficient research strategy to address this controversy that remains unresolved despite numerous RCTs.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Footnotes
Twitter @AsmaTurkait, @shaliniojha7
Contributors AA-T contributed to study conception and design, performed the data analysis and prepared the first draft and reviewed and approved the manuscript. The article is based on AAT’s PhD dissertation. LS prepared the statistical plan, supervised the data analysis, contributed to the writing of the first draft and critically revised and approved the manuscript. IC conceptualised the study design and critically revised and approved the manuscript. SO conceptualised the study design, obtained ethical approvals, contributed to the design of the statistical plan, and wrote and revised the final version of the manuscript. SO is the author responsible for the overall content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.