Article Text

Abstract
Background Current evidence supports progressive feeding in preterm infants. Due to lower necrotising enterocolitis risk, recent studies suggest starting total enteral feeding from birth in 30–33 weeks preterm infants. The feasibility of this practice is unclear.
Aim Explore feeding practices in 30–33 weeks preterm infants.
Design Prospective, multicentre, observational study recruiting 10 consecutive 30–33 weeks preterm infants from each of the eight UK hospitals.
Results Eighty infants received their first feed at median of 24 hours, achieving total enteral (without intravenous nutrition) and full feeds (≥150 ml/kg/day) at median of 5 and 8 days, respectively. Eleven infants who achieved total enteral feeding within 24 hours after birth achieved full feeds earlier (p=0.02) with shorter hospital stay (p=0.009) but were also of older gestation (p=0.004).
Conclusion Current early feeding approaches in 30–33 weeks preterm infants were found to be conservative. Total enteral feeding from birth is possible in these infants but further studies are needed.
- nutrition
- infant feeding
- neonatology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Recent evidence suggests that earlier and rapid enteral feeding could be achieved in very preterm infants without increasing risk of necrotising enterocolitis or death.
Compared with extremely preterm infants, there are fewer studies investigating enteral feeding practices in 30–33 weeks preterm infants who have lower necrotising enterocolitis risk.
Two Indian studies found total enteral feeding from birth in 30–33 weeks preterm infants to be feasible and beneficial.
What this study hopes to add?
Half the infants were fed on day 1, achieving total enteral (without intravenous nutrition) and full feeds (≥150 mL/kg/day) by days 5 and 8, respectively.
Eleven infants who achieved total enteral feeding by day 1 achieved full feeds earlier (p=0.02) with shorter hospital stay (p=0.009) but were of older gestation.
Total enteral feeding from birth is potentially feasible in 30–33 weeks preterm infants in the UK, but further studies are needed.
Introduction
A decision has to be made about how to feed every baby admitted for neonatal care. Conservative approaches have developed in an attempt to prevent necrotising enterocolitis (NEC), but recent meta-analyses have shown that earlier1 and rapid2 enteral feeding can be achieved in very preterm infants without increasing the risk of NEC or death. However, these studies concentrate on extremely preterm infants. There are very few studies investigating the early feeding of 30–33 weeks preterm infants, who have a lower risk of NEC, and represent nearly a fifth of preterm infants.
Two studies in India3 4 found the provision of total enteral feeding from birth in 30–33 weeks preterm infants to be feasible. Total enteral feeding from birth was defined as providing infants with exclusive enteral feeds without administering intravenous fluids. Infants given enteral feeds alone had improved feed tolerance, shorter hospital stays and reduced intravenous nutrition usage. However, the feasibility of this practice in the UK is uncertain.
Aim
We aimed to explore current feeding practices in 30–33 weeks preterm infants in the UK as well as associated mortality and morbidity (NEC and late-onset sepsis (LOS)).
Methods
Prospective, multicentre observational study in 10 consecutive 30+0 to 33+6 weeks preterm infants, born and cared for in each of the eight participating UK neonatal units was carried out from July to August 2016. Infants were excluded if they had conditions that made enteral feeding unsafe (eg, tracheo-oesophageal fistula). Feeding data were collected until full feeds was achieved (defined as ≥150 mL/kg/day for 3 days). Total enteral feeding was defined as receiving only enteral feeds without any intravenous nutrition. LOS was defined as sepsis presenting >72 hours after birth requiring ≥5 days of intravenous antibiotics. NEC was defined as condition meeting the stage 2 or 3 of the modified Bell’s criteria.
No ethical approval was sought as this was purely an observational study exploring feeding practices in 30–33 weeks preterm infants in eight neonatal units across the UK. There was no new intervention proposed as part of the study. Each participating unit was advised to register the work with their local audit department.
Categorical and continuous data were presented as number of infants (percentage) and median (interquartile range (IQR)), respectively. Growth parameters were presented as mean ± standard deviation (SD) with Z-scores calculated using LMSgrowth 2012 (http://www.healthforallchildren.com/shop-base/shop/software/lmsgrowth/). A priori analyses by gestational age and whether total enteral feeding was achieved within 24 hours after birth were performed. Mann-Whitney U test and χ2 test were used to compare continuous and categorical data, respectively. The Jonckheere-Terpstra test was used to compare trends among medians of multiple groups with an ordered pattern.
Results
Demographics
Eighty infants were recruited from seven lead units (Birmingham, Bristol, King’s College London, Leeds, Newcastle, Nottingham and Sheffield) and one local unit (Worcestershire). The median (IQR) gestational age was 32+3 (31+1–33+0) weeks and mean (SD) for birth weight as well as head circumference were 1728 (382) g and 29.3 (1.9) cm, respectively. There were 41 (51%) boys, 5 (13%) sets of twins and 1 (4%) set of triplets. One infant died and her data up to day of death had been included.
Enteral feeding practices
Infants received their first feed at a median (IQR) of 24 (11–43) hours of age. Forty-two (53%), 2 (3%) and 32 (40%) infants received maternal breast milk, donor breast milk and formula milk, respectively, as their first feed. The type of milk received was not specified in four (5%) infants. Waiting for breast milk was reported as the reason for delay in starting feeds in 43 (54%) infants (table 1).
Reason reported for the delay in starting enteral feeds from birth in 80 30–33 weeks preterm infants in the multicentre prospective observational study.
Feeds were increased at a median (IQR) rate of 24 (17–32) mL/kg/day, achieving full feeds on a median (IQR) of 8 (6–11) days. A median (IQR) of 5 (2–9) days of intravenous nutrition was given. Thirty-one (39%) infants had central venous access.
Outcome
Seventy-nine infants survived to discharge from hospital which was at a median (IQR) of 26 (16–39) days. Two (3%) infants developed NEC. One infant was from a set of twins born at 31+5 weeks gestation weighing just below the 25th centile for birth weight. She was predominantly fed with formula milk up to 45 mL/kg/day on day 3 when she developed stage 3 NEC. Her NEC was diagnosed based on surgical findings on day 3 of age. Unfortunately, she died 2 days later. Her twin brother was born just above the 25th centile for birth weight. He did not develop NEC despite being managed similarly.
The other was an infant born at 30+1 weeks gestation, weighing 50th centile for birth weight. He developed stage 2 NEC at 14 days of age after tolerating full enteral feeds for 4 days. He received formula milk exclusively increasing at an average rate of 23 mL/kg/day to achieve full feeds. His NEC was diagnosed based on radiological findings and was managed conservatively.
The Z-score for weight for gestational age in 79 infants, and head circumference for gestational age in 60 infants changed by −0.7±0.8 and 0.1±1.8 from birth to discharge. There were nine (11%) cases of LOS including four (5%) with positive blood or cerebral spinal fluid (CSF) cultures.
A priori analyses
Gestation
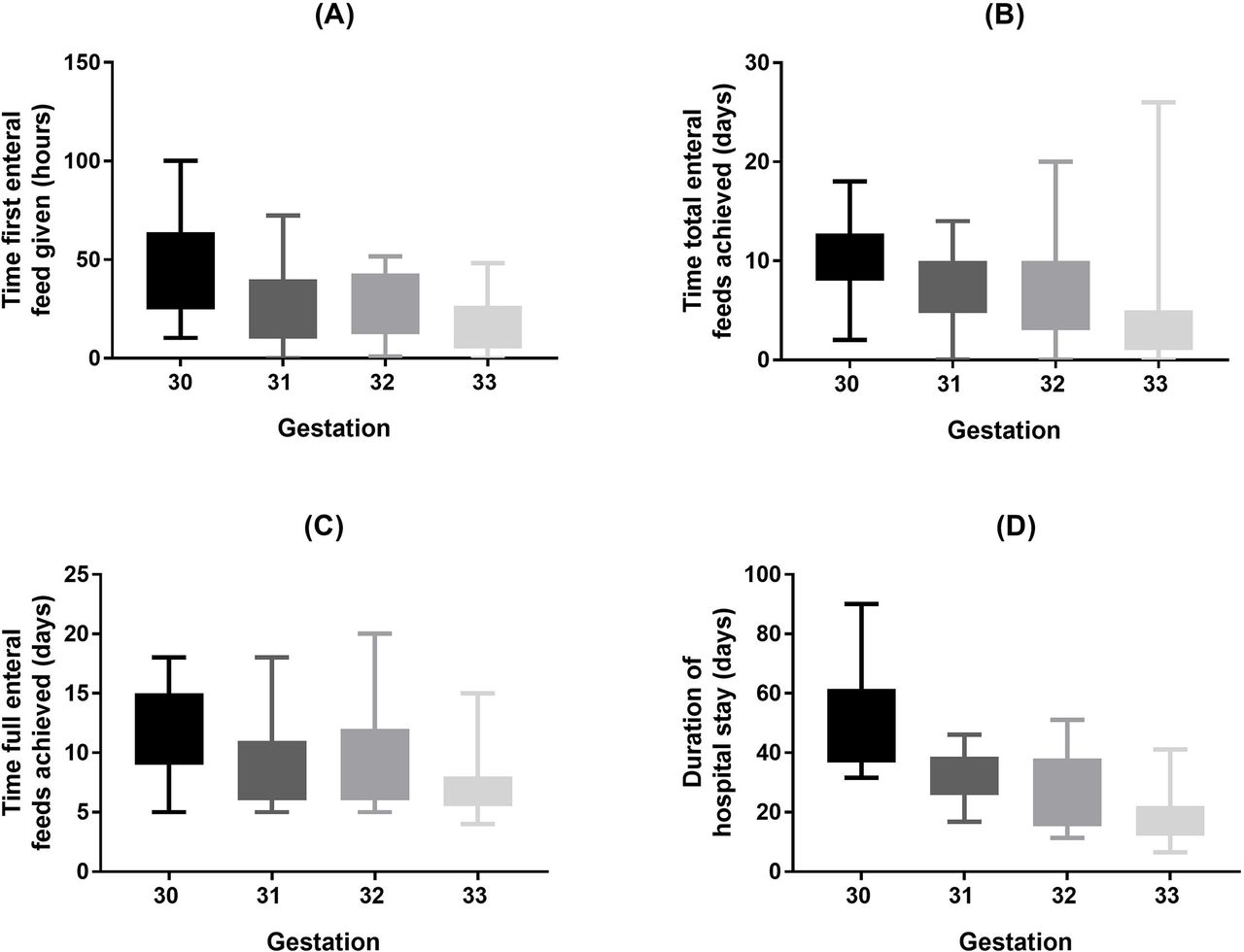
Higher gestational age at birth was associated with infants receiving the first (p<0.001), total (p<0.001) and full feeds earlier (p<0.001), as well as shorter hospital stay (p<0.001) (figure 1).

{kind=link}
Box and whisker plots depicting the time first enteral feed given (A), time total enteral feeds achieved (B), time full enteral feeds achieved (C) and duration of hospital stay (D) in 30-33 weeks preterm infants in the multicentre prospective observational study. The box represents the interquartile range, while the whiskers represent the minimum and maximum values.
Total enteral feeding within 24 hours after birth
Eleven (14%) infants achieved total enteral feeds within 24 hours after birth. They were of higher gestation compared with those who were not totally enteral fed by 24 hours (33 vs 32 weeks, p=0.004). They also achieved full feeds earlier (5 vs 8 days, p=0.02) and had shorter admissions (18 vs 30 days, p=0.009).
Discussion
Two randomised trials3 4 have suggested that it is possible to achieve total enteral feeds from birth in 30–33 weeks preterm infants. However, these reports, with very small numbers, are from India where the healthcare setting is very different and the preterm population may not be representative of that in the UK. However, the risk of NEC is very low in infants above 30 weeks gestation and other emerging evidence supports early progressive feeding.1 2 Despite this, we found that only half of our consecutive sample of 80 infants from eight UK neonatal units received their first feed by day 1 and total enteral feeds without any intravenous nutrition by day 5. Ninety per cent of the cohort received their first feed by 55 hours and achieved total enteral feeds by 13 days of age.
Non-availability of breast milk was reported to cause delay in starting feeds in half of the infants, raising the question of whether alternative milks such as donor breast milk or formula milk should be used in this period or whether it is better to wait for maternal breast milk. Studies to date are inconclusive and heterogeneity among the studies makes the evidence difficult to assess.5
Our study found that infants who were totally enteral fed within 24 hours after birth achieved full feeds earlier with shorter hospital stays without statistical differences in death, NEC or LOS. However, our study was limited by a small sample size and the results were likely to be confounded by gestational age. This was because infants who were totally enterally fed within 24 hours after birth were also of higher gestational age. Mature infants were more likely to be given total enteral feeding, tolerate milk feeds, and be discharged sooner with lower risk of complications.
Hence, an adequately powered pragmatic randomised controlled trial is needed to assess whether providing total enteral feeding from birth in 30–33 weeks preterm infants improves outcomes and reduces hospital stay without increasing the risk of NEC in the UK. The trial would require a clear pathway to obtain parental consent and to allow deviation from study protocol for medical needs. The trial is needed to re-evaluate current enteral feeding practices and enhance understanding of enteral feeding physiology in moderate preterm infants which may differ from early preterm infants. This is crucial as total enteral feeding from birth may also be beneficial in resource rich settings like the UK. It may prevent unnecessary use of intravenous nutrition and venous access which are associated with infection and metabolic complications. It may also improve maternal–infant bonding experience by reducing the time of maternal–infant separation through earlier establishment of enteral feeding and earlier discharge.
Conclusion
Our study found the feeding approach in 30–33 weeks preterm infants in the UK to be conservative. Total enteral feeding from birth is potentially feasible in these infants, but further trials are needed before a change in practice can be recommended.
Acknowledgments
We would like to thank Dr Gillian Preston and Dr Gemma Holder (Birmingham Women’s Hospital), Catherine Turner and Dr Paul Mannix (Southmead Hospital), Dr Ann Hickey (King’s College, London), Dr Alex Liu and Dr Kathryn Johnson (Leeds General Infirmary), Dr Stefan Zalewski and Dr Nicholas Embleton (Royal Victoria Infirmary), Dr Rebecca Musson and Dr Tamanna Williams (Jessop Wing, Sheffield) and Dr Viviana Weckemann (Worcestershire Royal Hospital) for their support and help in providing the data.
Footnotes
Contributors All three authors equally contributed in preparing the manuscript.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Data sharing statement Unpublished data on volume of enteral feeds increased per day are available from the corresponding author by email.