Article Text

Abstract
Introduction Neonatal jaundice is a common cause of concern in immediate newborn period for parents as well as for the caregivers. Babies with visible jaundice are identified by the healthcare provider, and blood samples are sent for confirmation. Clinical expertise varies from person to person and may lead to sending excessive blood sampling. Obtaining blood bilirubin samples is a painful procedure; it predisposes the baby to infections and requires skilled health personnel. Moreover, laboratory tests are costly and time consuming, leading to unnecessary delays in commencing phototherapy and discharge from hospital. Transcutaneous bilirubinometer has been in use for a long time as screening tool in postnatal wards. With passage of time, its accuracy and validity have improved tremendously.
Methodology We aim to implement a quality improvement initiative to reduce the number of blood bilirubin samples using transcutaneous bilirubin (TcBR) nomogram in full-term, low-risk babies who are born at our hospital and are admitted in postnatal ward after birth. Using preanalysis and postanalysis study design, this study will be performed in two phases of 6 months each. Data regarding total number of admissions in postnatal wards, demographics, serum bilirubin(TSBR) samplings and need for phototherapy will be recorded in both phases. TcBR will be done and recorded in postimplementation phase.
Analysis and results Comparisons between the two groups will be made. Primary outcome will be reduction in blood bilirubin samples for TSBR after the implementation of TcBr protocol. The proportion of infants having TSBR performed in both periods will be compared. Crude sampling cost of TSBR will be obtained from laboratory, and cost comparison between two phases will be done to look for difference.
- hyperbilirubinemia
- neonate
- transcutaneous bilirubin meter
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Neonatal jaundice is a common cause of concern both for caregivers and parents.
If left unrecognised, it can lead to serious complications like bilirubin encephalopathy.
Transcutaneous bilirubin meter has proven to be a good tool for screening of neonatal jaundice.
What this study hopes to add?
We are presenting a quality improvement protocol to reduce the number of blood bilirubin samples for neonatal jaundice.
We have introduced a TcBR nomogram for the first time in Pakistani population.
If successful, this can be used at a larger scale for improvement in quality and reduction in cost of care for babies with neonatal jaundice.
Introduction
Neonatal jaundice is a common cause of concern in the immediate newborn period for parents as well as for caregivers. It occurs in many newborns, usually after the first 24 hours of life and spontaneously resolves over the next few days. If deep and prolonged jaundice remains unrecognised, it can lead to bilirubin encephalopathy and permanent neurological damage.1
Traditionally babies with neonatal hyperbilirubinaemia are screened clinically using Kramer’s scale or by using other modalities.2 Blood bilirubin samples for total serum bilirubin (TSBR) is usually done to confirm and start treatment once jaundice is identified.3 Serum TSBR sampling is a resource-intensive procedure. It requires skilled health personal and can also lead to nosocomial infections.4 Moreover, laboratory testing is costly and time consuming, leading to unnecessary delays in commencing phototherapy and discharge from the hospital.5
Transcutaneous bilirubin (TcBR) measurement devices use multiwavelength spectral reflectance from the skin surface and can be used to estimate total serum or plasma bilirubin and thus avoid blood sampling. TcBR is a ‘Point of Care’ test (bed-side test) that can be performed by physicians, nurses or any other health caregiver within hospital or in community.6 It is used as a non-invasive, rapid screening tool to identify babies with neonatal hyperbilirubinaemia.7 Various studies have shown its efficacy, safety and utility.8 9 One randomised controlled trial done in the Netherlands showed significant reduction in blood bilirubin samples in TcBR group compared with non-TcBR group.9 TcBR is an inexpensive test10 and can be performed over forehead or mediastinum, but studies suggest that measurements over mediastinum are better than forehead.11 Despite its utility, only 27% of the hospital wards are using TcBR as a screening tool.9
Although TcBR is a good screening tool, TSBR is still the gold standard for diagnosing and commencing phototherapy.12 Most studies on the use of TcBR are done to establish its accuracy, comparing TSBR with TcBR levels. Implementation of TcBR in hospital or community-screening programme is associated with a reduction in the incidence of severe neonatal jaundice, readmission for phototherapy and lower duration and rate of phototherapy.13 Study done on TcBR from our institute 25 years back showed a poor sensitivity and specificity of 88% and 53%, respectively.14 Important to note was the small sample size, and both term and preterm infants were enrolled. Similar study from Pakistan during the same era showed good sensitivity.15 Technology has advanced significantly since then with the emergence of newer and more sophisticated devices with good precision. Recent data from Pakistan have shown good correlation of TcBR with TSBR.16
Although several TcBR nomograms have been evaluated, significant differences exist across populations based on ethnicity, race and bilirubin kinetics.17 A systematic review based on four studies that constructed TcBR nomograms from predominately Caucasian, Thai or Hispanic populations reported TcBR nomogram values varied among the ethnic groups. Up to the best of our knowledge, no study has been performed using TcBR nomogram in Pakistan. Therefore, it is imperative to know the nomogram for our babies. The aim of our quality improvement initiative is to reduce the number of blood bilirubin samples by introducing a TcBR nomogram (attached) to plot the readings of TcBR and only do serum TSBR sampling when the readings cross the TcBR line (blue line). We hypothesise that if our TcBR nomogram is safe and effective, this will reduce the number of blood bilirubin samples significantly and will be incorporated into the hospital phototherapy protocol.
Objectives
We intend to implement a quality improvement project to reduce the number of blood bilirubin samples by introducing a TcBR nomogram in full term well babies admitted in the postnatal ward of our hospital.
Study design
Preanalysis and postanalysis design with preimplementation phase being retrospective and postimplementation phase as prospective cohort.
Settings
Postnatal ward of Aga Khan University Hospital, Karachi.
Duration
Thirteen months.
Inclusion criteria: eligibility criteria
All babies admitted to the Aga Khan University Hospital postnatal ward from 1 September 2016 to 30 September 2017 with gestational age 37 weeks or more with birth weight more than 2500 g having clinical jaundice after 24 hours of life but within 7 days of life.
Exclusion criteria
Babies having clinical jaundice within 24 hours of life or after 7 days of life.
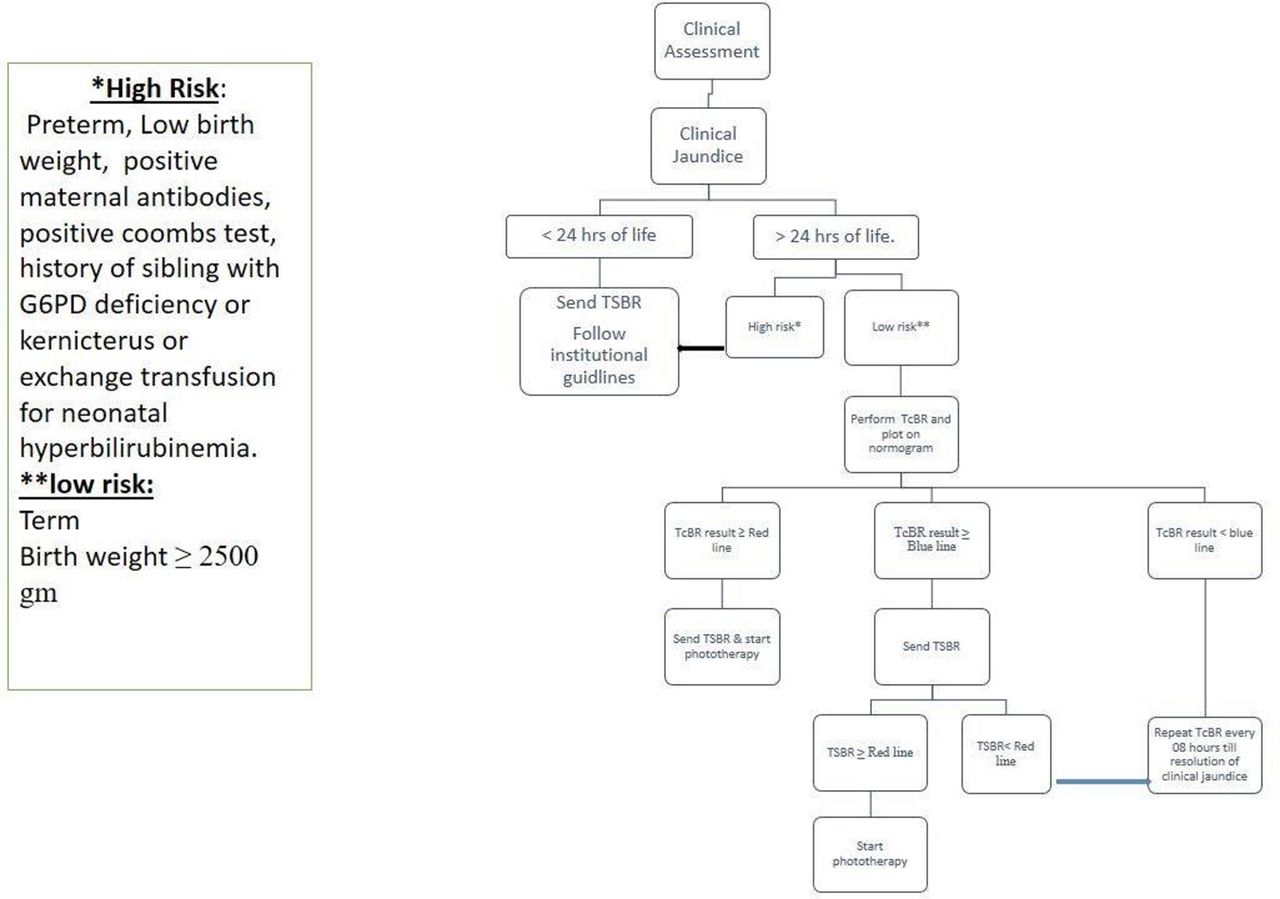
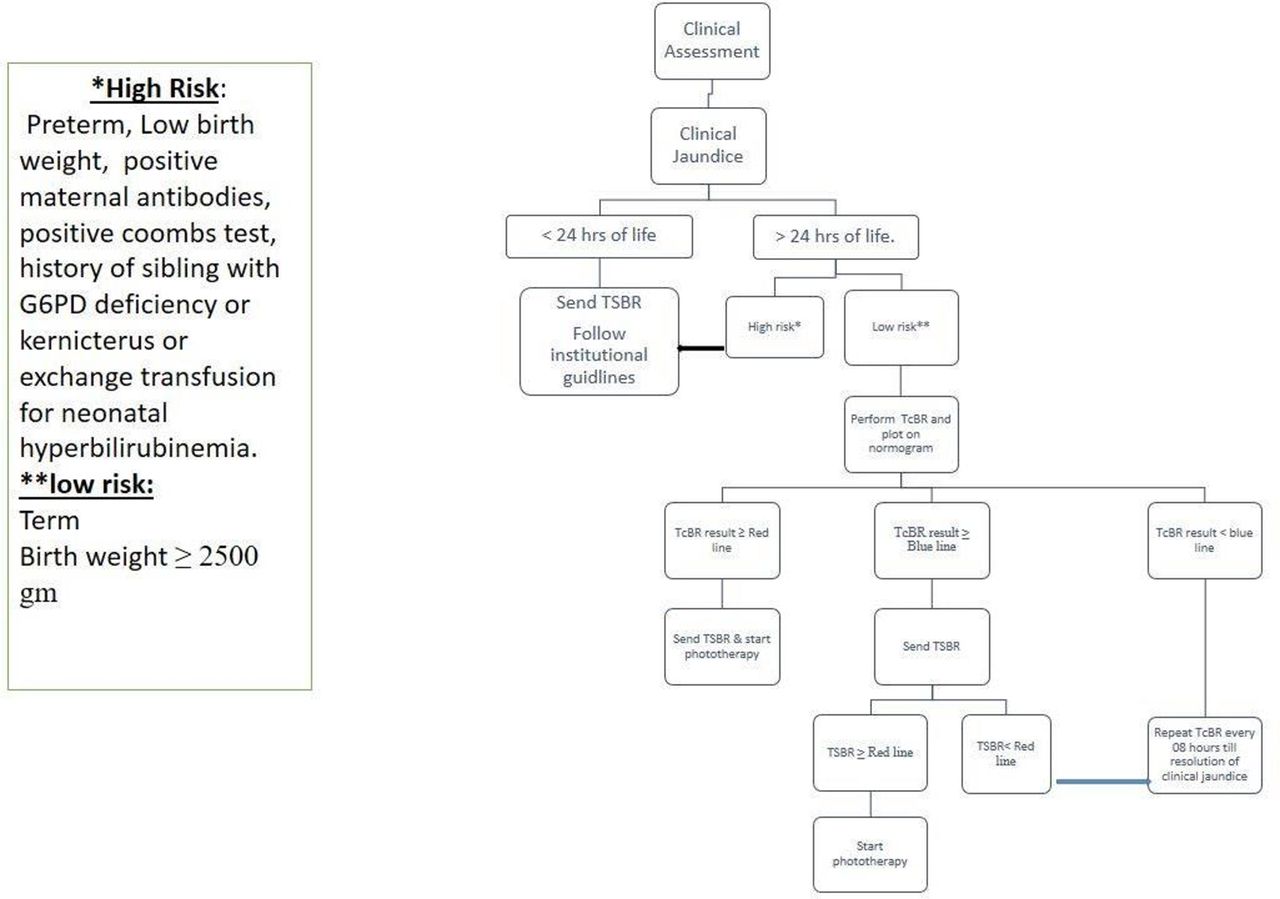
Babies at high risk for neonatal hyperbilirubinaemia, that is, preterm, low birth weight ,babies whose mothers have positive antibody screening, babies with positive Coombs test, babies requiring serum TSBR sampling within 24 hours of life, babies already on phototherapy, history of sibling with G6PD deficiency, history of sibling with kernicterus and history of sibling requiring exchange transfusion for neonatal hyperbilirubinaemia.
Operational definitions
Clinical jaundice
Yellow discolouration of skin reaching up to abdomen assessed by trained health worker, that is, physician or nursing staff.
Methodology and data collection
The study will be performed in three phases.
Phase 1: Preimplementation phase
Duration: 6 months (1 September 2016–28 February 2017).
Data regarding all neonates admitted in postnatal ward will be extracted retrospectively using medical records. Following data will be collected for all eligible cases.
Demographic data including gestational age, chronological age, gender and birth weight and so on, will be extracted from the hospital database. TSBR data will be retrieved from the laboratory’s online database, and all babies who received phototherapy will be identified by reviewing medical records and cross-checked against nursery discharge data (figure 1).
Preimplementation phase flow diagram. TSBR, total serum bilirubin.
Implementation phase
1 March 2017–31 March 2017.
Two Dräger JM-105 TcBR metres are being used, one for each well baby nursery. Both devices are being regularly calibrated and serviced by our hospitals biomedical department.
TcBR nomogram
TcBR nomogram is made using American Academy of Pediatrics (AAP) guidelines for phototherapy threshold. A new line is drawn 2 mg/dL (34.2 µmol/L) below the phototherapy line for low-risk babies and is named as TcBR line because literature review reveals a variation of ±1 mg/dL (17.1 µmol/L) in results of TcBR and TSBR.18 For simplification, the high and intermediate risk lines are removed from the chart since those babies are not the study population and their management is being done according to the hospitals jaundice protocol. The lines are colour coded. Phototherapy line is of red colour, whereas TcBR line is blue coloured. This modification in the AAP nomogram is called as TcBR nomogram. Attached is the sample of our TcBR nomogram (figure 2).
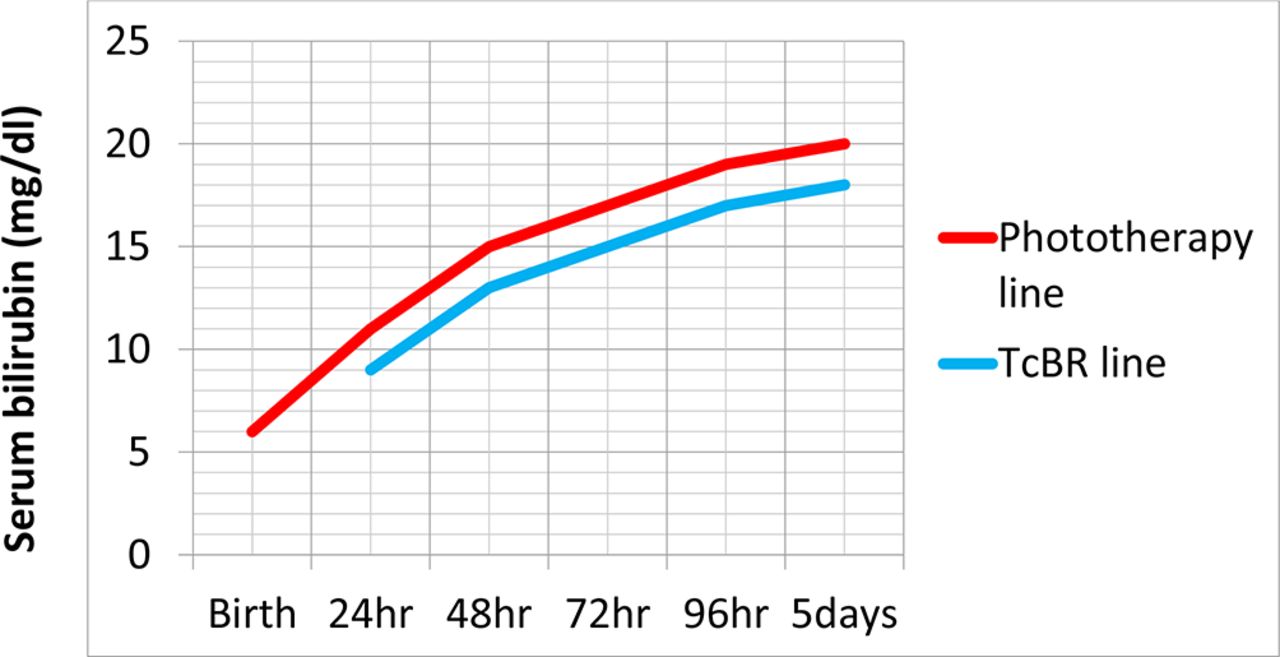
Transcutaneous bilirubin nomogram for term well babies.
Prior to the implementation of the project, hands-on training and competency certification of all neonatal healthcare providers has been undertaken by senior neonatologist/nurse instructor in which all components of study protocol were explained. Protocol flow chart and TcBR nomogram were handed over to all postnatal nurses and physicians and also pasted at all postnatal ward areas for reference.
The study is approved by the hospitals ethical review committee (Ref # 4742-PED-ERC-17).
Phase 2: postimplementation phase
Duration: 6 months (1 April 2017–30 September 2017)
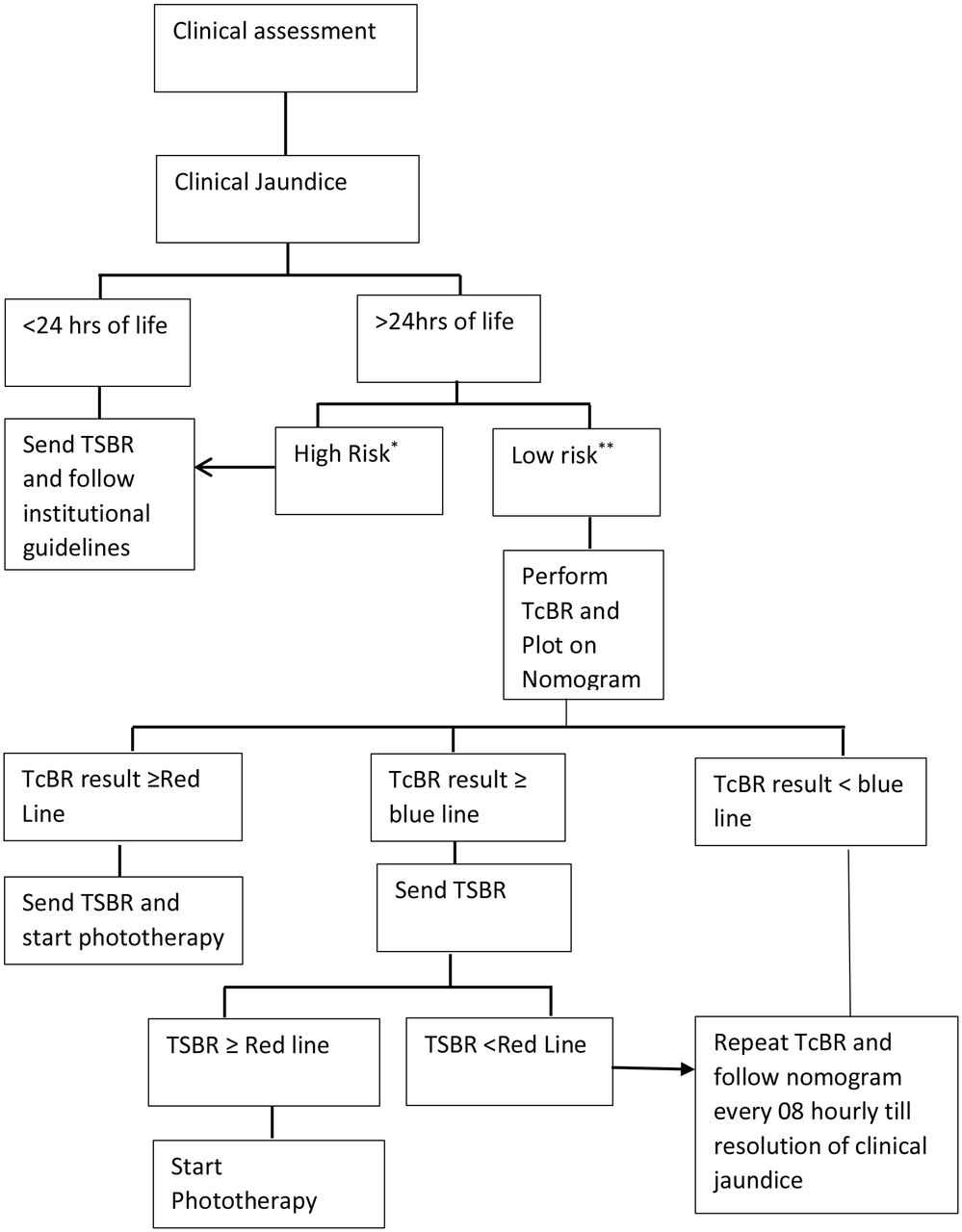
All babies meeting eligibility criteria having clinical jaundice assessed by nursing staff/paediatric resident/neonatology fellow will be approached. Basic demographic and anthropometric data will be recorded. TcBR will be performed using Dräger JM-105. Three consecutive readings will be taken on the sternum, and mean result will be recorded on the proforma. If TcBR level falls on or over red line (phototherapy line), serum TSBR will be sent and phototherapy will be started. If TcBR level falls on or over blue line (TcBR Line), then serum TSBR will be sent, and phototherapy will be started only if TSBR falls on or over red line (phototherapy line). All babies with TcBR or TSBR level below blue line (TcBR line) will be followed with TcBR testing after every 8 hours until resolution of clinical jaundice (figure 3).
{kind=link}
{kind=link}
{kind=link}
Postimplementation phase protocol flow diagram.
Sample size
As we have an average of 4000–5000 admissions in postnatal wards per year, out of which approximately 500–1000 are high-risk babies, we anticipate a sample size of around 1500 eligible babies in each phase.
Outcome
Primary outcome
Reduction in the number of blood bilirubin samples for TSBR.
Secondary outcomes
Assessment of accuracy of bilimeter in Pakistani population.
Reduction in the cost of blood bilirubin sampling between the two phases.
Analysis plan and results
Analysis will be done on SPSS V.19. Means with SD will be used for normally distributed data. Comparisons between the two groups will be made using equality of variances test and two independent t tests for comparing means. The proportion of infants having a TSBR performed in both periods will be compared with the χ2 test.
Assessment of accuracy of bilirubin metre will be assessed by performing comparative analysis between TcBR and TSBR only on those babies in whom both are done.
Sampling cost of TSBR will be obtained from laboratory and cost comparison between two phases will be done to look for difference.
We will use SQUIRE V.2.0. Guidelines for reporting our findings.19
Discussion
NICE guidelines 2016 for the management of neonatal hyperbilirubinaemia recommends the use of TcBR for the screening of babies who are >24 hours old and >35 weeks.20 We aim to improve the quality of care given to our neonates by reducing the number of blood bilirubin samples using TcBR nomogram on babies who are low risk and are >24 hours old. We believe that this will decrease the requirement of blood bilirubin samples for TSBR and also reduce cost, infections, pain and delay in discharge from hospital. If the results are suggestive and favourable, this protocol will be incorporated into our hospitals phototherapy protocol.
References
Footnotes
Contributors All authors have contributed equally.
Competing interests None declared.
Ethics approval Ethical review committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement None.