Article Text

Abstract
Background Allergies are a growing health concern with a significant impact on quality of life and healthcare costs. It is critical to develop an appropriate care plan to deal with children’s allergies. This study aimed to assess and compare the knowledge and perception of families and school personnel caring for children with history of anaphylaxis who were prescribed the epinephrine autoinjector (EpiPen). The study also examined the underlying reasons for any observed knowledge gaps.
Methods A cross-sectional study of 128 families and 50 corresponding school personnel caring for children at risk of anaphylaxis who had been prescribed the EpiPen was conducted. The primary outcome was to identify any knowledge deficiency within family and school personnel and the reasons behind knowledge gaps.
Results Of the 128 screened schools, 30 (23%) were not informed by parents about their pupils’ risk of anaphylaxis. Importantly, 113 (88%) of families and 42 (84%) of schools were unable to recognise the symptoms of anaphylaxis. Also, 67 (52%) of families and 22 (44%) of schools were not aware that a child should ideally have two EpiPen in case of a severe allergic reaction. The EpiPen had been used by 18 (14%) families and 5 (6%) schools.
Discussion Communication among families and school personnel regarding anaphylaxis was suboptimal. Both parents and school personnel lacked key information in allergy management. Managing a child at risk of anaphylaxis requires effective communication among healthcare professionals, families and schools. There is an urgent need to improve knowledge of anaphylaxis and its management among families and school caregivers.
- allergy
- school health
- general paediatrics
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Anaphylaxis can be fatal if not addressed in a timely and effective manner.
Studies have identified the limited availability of epinephrine autoinjectors in schools.
There are limited data about the role of instructions and communication between parents and school in the knowledge of anaphylaxis.
What this study hopes to add?
There are key deficiencies in knowledge regarding the recognition and management of anaphylaxis among caregivers of children.
Receiving instructions was more important than who gave the instructions in the knowledge outcome.
Effective communication between school personnel and parents is required to develop an appropriate care plan.
Introduction
Allergies are a growing health concern, with studies suggesting a cumulative prevalence of 3%–6% in children, translating to a significant impact on quality of life and healthcare costs.1 There is an increasing number of cases of peanut allergy and anaphylaxis visiting paediatric emergency departments. When allergies result in anaphylaxis, timely and efficient use of the epinephrine autoinjector (EpiPen) can be life-saving. Most anaphylaxis events in children occur either in the presence of family members or at school. A recent US school study reported that 55% of EpiPen use was for children with no identified previous risk who had their first episode of a serious allergic reaction at school.2
Knowledge about anaphylaxis and its management has been studied with a primary focus on either parents or schools. In a study of 237 schools, only 53% of school personnel reported to have been informed by primary caregivers that their children had a history of anaphylaxis.3 Other issues identified were the limited availability of the EpiPen at school; out of 171 California schools, only 13% reported having an EpiPen stock at their campuses.4 Knowledge gaps identified among families of allergic children have included the recognition of anaphylaxis and anaphylaxis management aspects and how the EpiPen is used.5 6 Out of 101 families, only 32% correctly demonstrated the use of the EpiPen device.7
Formal training of school personnel and caregivers, regarding the prevention, diagnosis and management of allergies is of paramount importance.8 9 Effective communication among school personnel and parents is required to develop an appropriate care plan to deal with allergies during school time.10
No previous study has examined knowledge of anaphylaxis and EpiPen use among parents of children who had a history of anaphylaxis and personnel at schools where these children attend in Qatar, a country in rapid development with a diverse population. The primary objective of our study was to determine current knowledge and perceptions regarding anaphylaxis and its management in Qatar. We hypothesised that families and school personnel lack the key knowledge regarding allergies and anaphylaxis. For children with a history of anaphylaxis who had been prescribed the EpiPen, the study compared knowledge between parents and schools. The secondary objective was to identify the underlying reasons for any observed knowledge gap. Understanding key knowledge gaps and their underlying reasons is essential for optimising the training of key persons who may deal with a child’s anaphylaxis, thus ensuring that a fatal outcome is avoided.
Methods
Study design
This study was a two-phase cross-sectional study. Both the institutional review board and the Hamad Medical Corporation Hospital Committee approved the study. Verbal consent was taken after explaining the objectives of the study, and predetermined questions were administered over the telephone.
Setting
The study was conducted in Doha, the largest city and capital of Qatar. Families and schools were included. Schools included public and private nurseries, kindergartens and primary and secondary schools. In phase 1, the parents of children with known anaphylaxis and prescribed the EpiPen identified from clinical records (at Hamad General Hospital, the only tertiary healthcare centre in Qatar) were contacted. Parents were asked to supply the name and contact details of their child’s school. In phase 2, we contacted the schools to identify personnel who were likely to deal with a child’s health problems (nurse, teacher or school principal). We started collecting data from February 2016 to June 2016. Contact was attempted three times, and if no response was obtained, we deemed the participant to be a non-responder.
Participants
Parents and school personnel caring for children aged 1–14 years old, with a previous history of anaphylaxis, who had been prescribed the EpiPen device between August 2015 and December 2015 were eligible for the study.
Selection criteria
We selected all families who had children with history of anaphylaxis and whose children had been prescribed the EpiPen. School names and contact information were received from families. Our study included both private and public schools.
Sample size
From the medical records of the hospital, we selected all patients who had history of anaphylaxis and been prescribed EpiPen between August 2015 to December 2015. A sample size of 140 was obtained. Three families were not willing to participate, four had the wrong contact numbers and five had telephone numbers that were out of service. For school sample size, refer to figure 1.

School sample size assembly.
Study tools
Participants were contacted by telephone, the most common and effective communication modality in Qatar. Telephone-administered questions were delivered in either Arabic or English, depending on the parent/school personnel’s language preference. The interview questions were based on previous studies and clinical expertise of the investigator group.
Twenty-four questions were asked from families and 21 from schools (table 1). Parents had three additional questions to ascertain details of the epinephrine prescription (prescriber, clinic and date). According to responses to the interview questions, further enquiry was conducted to confirm the accuracy and consistency of the responses.
Interview question areas and response choices
Variables
Four variable domains were included in the interview:
Demographic data
Allergy-related questions
Anaphylaxis
Epinephrine-knowledge-related questions.
Outcomes
The outcomes of interest were the following:
The knowledge related to anaphylaxis definition and management and knowledge related to EpiPen characteristics and use;
The gaps in the knowledge related to anaphylaxis identification and management;
The reasons behind identified gaps, including whether the instructions received and the role of the instructors in the knowledge outcomes;
Communication between families and school personnel.
Definitions
The definition of anaphylaxis used was according to the World Allergy Organization11: a severe allergic reaction that involves more than one system, can happen instantly, and EpiPen usage can save life when used promptly. For assessment of when to use the EpiPen, we used severe cardiorespiratory symptoms (respiratory difficulty or hypotension) as the indication for use. Detailed information about EpiPen prescription, availability, symptoms for which it was used, instructions given, storage area, temperature, expiration date and steps used in its administration was included.
Data sources/measurement
The study assessed and compared knowledge-related interview questions among family caregivers and school personnel as primary objectives. Attempting to understand knowledge gaps as a secondary objective, we analysed the knowledge of participants based on the individual who provided instructions to them, and where parents demonstrated better knowledge compared with school personnel, we further examined the effectiveness of the individual providing instruction regarding the epinephrine autoinjector use.
Statistical analysis
Descriptive statistics were used to summarise demographic and all other characteristics of the participants. We assessed knowledge-related responses in family and school as quantitative data using frequencies along with percentages (univariate analysis). For comparisons between families’ and schools’ knowledge and the role of instructors in both family and school knowledge outcomes, we used the χ2 test (multivariate analysis).
A two-sided p value <0.05 was considered to be statistically significant. Because the study was survey based, there were few missed data to affect the conclusion of the study. The missed data were not accounted in the analysis. All statistical analyses were conducted using statistical package SPSS, V.19.0 (IBM).
Results
Families
A total of 128 of the 140 parents identified agreed to participate over the 3-month study period (91% response rate). The majority of families 125 (98%) were aware of the reason why the EpiPen was prescribed for their child. The indications for EpiPen prescriptions were: 76 (61%) were for a food allergy, 18 (14%) for bee-sting allergy, 18 (14%) for unknown allergy, 9 (7%) for multiple allergies and 4 (2%) for medication allergy. The the most common type of food allergy was nut allergy, 50 (66%) of all food allergy, and mainly peanut allergy, 30 (60%) of all nut allergy. The prescribers for the EpiPen were: paediatricians 74 (58%), allergists 49 (38%) or both 5 (4%).
Schools
We evaluated 128 schools having children with history of anaphylaxis who were prescribed the EpiPen. From these, 50 schools participated in the study for a variety of reasons (figure 1). Importantly, 30 out of the original 128 screened schools (23%) denied having been informed by parents about their pupil’s history of anaphylaxis EpiPen prescription.
The majority of the children included were males, 30 (60%). Importantly we found that 20 (40%) did not have the EpiPen available at schools. Surprisingly, 8 (16%) claimed that they were forbidden by school administration to give injections at school.
Comparison of knowledge between families and school personnel
Table 2 shows the knowledge-related responses from families and schools. The EpiPen had been used by 18 (14%) of the families, while schools reported using it in only 5 (6%). Importantly, 113 (88%) families and 42 (84%) schools were unable to recognise the symptoms of anaphylaxis. Both families (67 (52%)) and school personnel (22 (44%)) were not aware that a child should ideally have two EpiPen in case a severe allergic reaction is ensued requiring more than one dose.
Knowledge-related responses
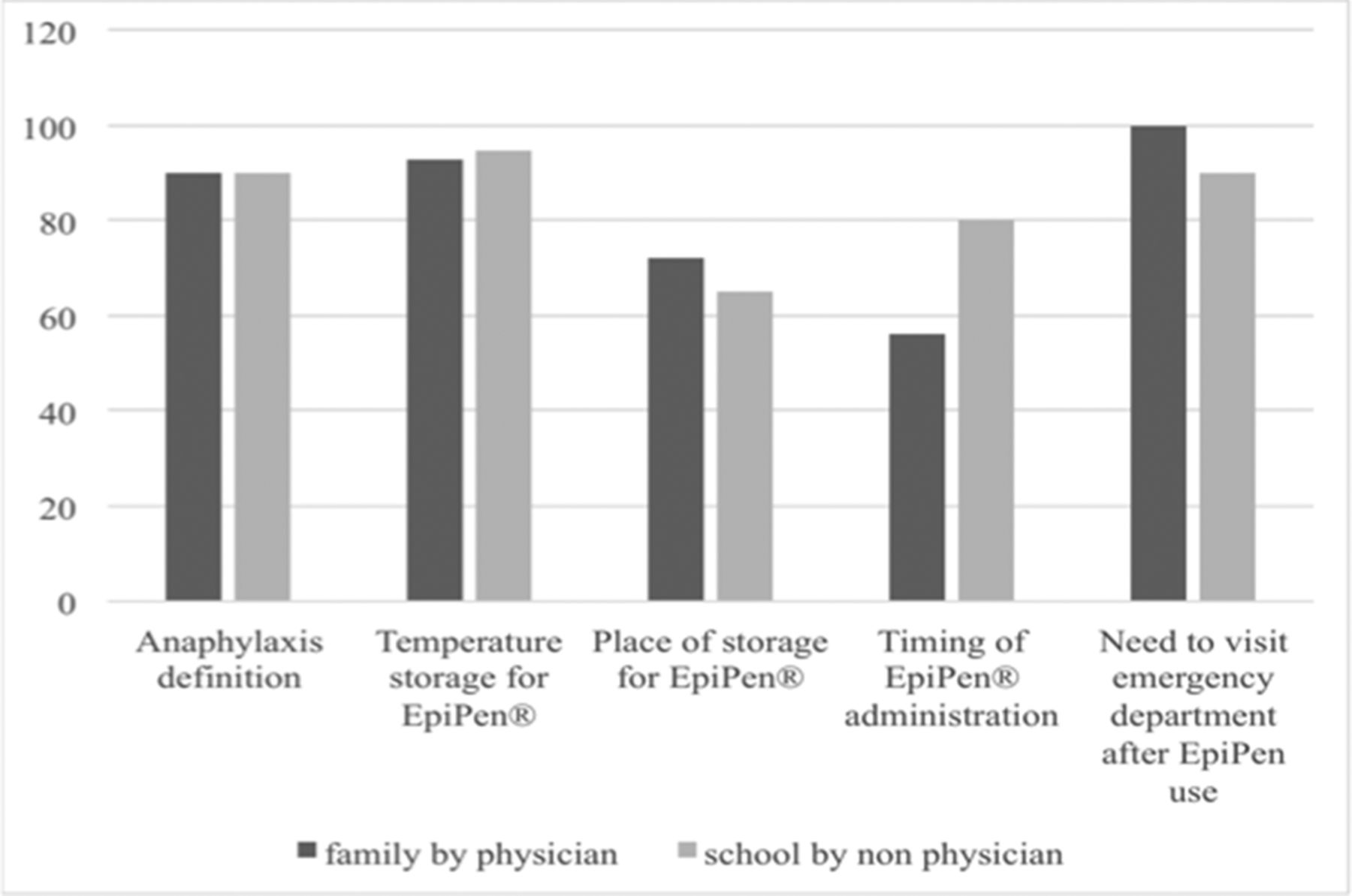
Families’ knowledge significantly exceeded school personnel about the definition of anaphylaxis, correct temperature storage for the EpiPen and the need to visit the emergency department after EpiPen administration. Although not statistically significant, families’ knowledge was also greater regarding the ideal number of EpiPen a severely allergic child should own, the site of storage and how soon after suspected a trigger should a caregiver administer the EpiPen.
The instructions given to families were mainly by physicians, while those given to school personnel were mainly by non-physicians (table 2). Figure 2 compares the instructors’ effectiveness in areas where the families’ knowledge was greater than school personnel.

{kind=link}
{kind=link}
Comparing instructors’ effectiveness at areas of families’ knowledge strength over schools.
We compared the knowledge of participants based on the individual providing instructions (table 3). We found that, for families, instruction given by physicians was associated with significantly greater knowledge in only three areas: the place of storage of EpiPen (physician 74 (72%) vs non-physician 9 (60%)), the correct sequence giving EpiPen (physicians 67 (65%) vs non-physicians 12 (57%)) and the need not to remove clothing before administering the EpiPen (physicians 72 (70%) vs non-physicians 9 (60%)). For schools, one significant area of knowledge was the circumstances requiring action if a child was exposed to an allergen related to the child’s anaphylaxis (physician 5 (30%) vs non-physician 16 (80%)).
Comparing the knowledge of participants based on the individual providing instructions
Discussion
There are several notable findings from our study. Of importance is the observation that 30 out of the original 128 screened schools (23%) denied having been informed by parents about their pupil’s history of anaphylaxis and that the pupil had been prescribed the EpiPen. Nearly half of the schools did not have any EpiPen stock available at their campuses, although they had high-risk children. Surprisingly, eight (16%) claimed that they were banned by school administration to give injections at school.
Both families and school personnel were not aware that a child should ideally have two EpiPen in case of a severe reaction. School personnel and families were not aware of the symptoms mandating that the EpiPen be used and of how soon they should administer the EpiPen if they suspected an offending anaphylaxis trigger. Multiple other deficiencies in knowledge of managing anaphylaxis were observed for both families and schools.
Our study was the first to examine the knowledge of families and school personnel in Qatar with key findings that will inform the care of children at risk of anaphylaxis. Few studies have examined knowledge of anaphylaxis and its management in both families and schools. Furthermore, we aimed to identify factors associated with knowledge gaps, including the role of healthcare professionals delivering instructions regarding the use of the EpiPen. Our study relied on self-reports, which may limit our observations. We also did not examine actual episodes of anaphylaxis and how these were managed.
The communication between parents and schools regarding children with allergies is alarming. A cross-sectional study of 237 schools in Turkey3 revealed that only 125 (53%) of school teachers were aware of their children allergy. The findings from Qatar show that school awareness was better, although still low and of great concern. Greater communication between families and schools is essential to address this vital gap.
Both parents and school personnel reported reasonable knowledge of anaphylaxis definition, that is, anaphylaxis is a life-threatening condition, can occur instantly and use of EpiPen can be life-saving, if used promptly12 compared with other areas, but the level of knowledge was still poor. There were deficiencies in the identification of symptoms, the time a caregiver should inject the EpiPen if anaphylaxis was suspected and the number of EpiPen a child with history of anaphylaxis should ideally have.13 14 15
In our study, demonstration of knowledge regarding the correct sequence of administrating the EpiPen was just reasonable (79 (62%) of families had sufficient knowledge) compared with a cross-sectional study of 101 family members from New York where 32 (32%) knew how to demonstrate correctly the steps for autoinjector administration. In a study by Chad et al, the majority of parents (56%) were afraid of using autoinjectors for fear of either hurting the child or performing the steps incorrectly.7 16 We observed that more paediatricians were prescribing the EpiPen than allergists. Evidence suggests that the collaboration between the allergist and the family is essential to improve the skills of caregivers.17
Although the EpiPen is well known to be the immediate therapy, both families and school personnel appeared to be underusing it.18 19 While EpiPen availability can be improved through better communication between families and schools, there is a need to educate school administrators regarding the importance of timely and effective EpiPen use. In our study, we did not test whether the EpiPen was underused because of overprescription of the EpiPen, although according to the literature, epinephrine autoinjectors are both underprescribed and underused.20 21 Epinephrine autoinjectors cannot save lives when they are underused, used too late or not carried at all times or when an inadequate dose is absorbed.22
The families’ knowledge in multiple domains was significantly greater than school personnel. This is likely to be because they received more instructions than school personnel. Instructions by physicians were better in three areas only. Therefore, receiving repeated instructions may be more crucial than the healthcare professional delivering the instructions.
An exploratory, cross-sectional, descriptive study by Morris et al,4 which included 171 credentialed California school nurses, observed that only 13% had epinephrine stock programme and that there was a lack of policies and guidelines, inadequate training and deficiencies in the education of school personnel. Therefore, our work and previous studies highlight a multitude of deficiencies in knowledge of anaphylaxis and strategies for its management by families and school personnel. These pervasive deficiencies need to be addressed with specific tailoring for the sociocultural environment. Addressing key deficiencies in countries similar to Qatar, where there is rapid development and multiple nationalities, is challenging but can improve through specific policies and greater communication.
Conclusion
Managing a child at risk of anaphylaxis requires effective communication among healthcare professionals, families and schools. Families’ communication with school personnel was suboptimal; some families did not inform schools about their children’s allergies. Both parents and school personnel lacked key information regarding a child’s allergy management. Receiving repeated instructions appears to be more important than who gave the instructions in the knowledge outcomes. School personnel should be empowered to provide life-saving treatments such as EpiPen injections. There is an urgent need to improve knowledge of anaphylaxis and its management among families and school caregivers to avoid serious consequences for children at risk of anaphylaxis.
Acknowledgments
The authors thank Dr Carol Mancusso and the faculty team at the division of Clinical Epidemiology and Evaluative Sciences Research, Weil Cornell, New York, USA, for their guidance and feedback. We also thank the parents and the school personnel for their contribution and support.
References
Footnotes
Contributors SME (principal investigator) conceptualised the study, collected data, analysed it, drafted and wrote the manuscript. ST contributed substantively to designing, editing and drafting of the manuscript. MC revised the protocol and contributed to editing and drafting of the manuscript. HJ, FZ, FA and RHE helped with data collection and coding of data.
Funding ST is supported by the biomedical research program at Weill Cornell Medicine, Qatar, funded by Qatar Foundation.
Competing interests None declared.
Patient consent Parental/guardian consent obtained.
Ethics approval The study was approved by the institutional review board of Hamad Medical Corporation, Doha, Qatar.
Provenance and peer review Not commissioned; externally peer reviewed.