Article Text

Abstract
Currently, 5 million Palestinian refugees live in Palestine, Jordan, Syria and Lebanon and around 40% of these are children. Mortality rates for Palestinian children are comparable to neighbouring Arab countries but the speed of reduction has faltered in recent years. Morbidity is greatly affected by the occupation which has increased violence towards children, mental health problems and poor nutrition, particularly in Gaza which is experiencing a health crisis. Access to healthcare for children in Palestine is constrained as a result of the requirement for visas to travel into Jerusalem where specialist hospitals are sited, by difficulties with ambulance transfers, by shortages of equipment in hospitals and by lack of trained staff. Palestinian health workers are developing new initiatives in healthcare and show a high level of resilience, despite the very considerable stress affecting most citizens.
- paediatric practice
- comm child health
- children’s rights
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
In this article, we highlight the health problems of the Palestinian children, and in particular the difficulties they face in accessing healthcare.
This article focuses on the population in the occupied Palestinian territories of Gaza, the West Bank and East Jerusalem.
Palestinians represent the world’s largest refugee population and one of its longest standing. Military conflict and political turmoil stemming from the Arab-Israeli dispute have forced millions of Palestinians to leave their homes and seek refuge elsewhere, many more than once. The great grandchildren of the original refugees are now parents to refugee children, testimony of the duration of the dispute. Sadly, prospects of a just and lasting resolution of the conflict are not yet in sight. The socioeconomic hardship in which the Palestinian people have been living, whether it is in the Occupied Palestinian Territory itself or in the neighbouring countries of Jordan, Syria or Lebanon, is therefore likely to continue to be a serious challenge for the new generation in the foreseeable future.1
Who are Palestine refugees?
Palestine refugees are defined as ‘persons whose normal place of residence was Palestine during the period 1 June 1946 to 15 May 1948, and who lost both home and means of livelihood as a result of the 1948 conflict’.
The United Nations Relief and Works Agency for Palestinian refugees (UNRWA) provides health, social and educational services to those living in its area of operations who meet this definition, who are registered with the Agency and who need assistance. When the Agency began operations in 1950, it was responding to the needs of about 750 000 Palestine refugees. Today, some 5 million Palestine refugees are eligible for UNRWA services.2
Nearly one-third of the registered Palestine refugees, more than 1.5 million individuals, live in 58 recognised Palestinian refugee camps in Jordan, Lebanon, the Syrian Arab Republic, the Gaza Strip and the West Bank, including East Jerusalem.
The remaining two thirds of registered Palestine refugees live in and around the cities and towns of the host countries, and in the West Bank and the Gaza Strip, often in the environs of official camps.
In many ways, Palestinian health holds in microcosm the problems which face the world in the 21st century: migration, poverty, discrimination against minorities, poor access to healthcare, violence against children and the violation of their rights. Although Palestine has in effect been in existence since 1948 (historically for much longer), and the population has now been living under occupation for 50 years (since the 1967 war), the efforts of the UN and the world community have failed to enable justice and freedom for Palestinian people within their own state. It is not possible in this short article to provide a full history of the conflict, which has been described fully elsewhere—we recommend readers to the paper in the Lancet Palestinian Health series by Giacaman et al,3 which summarises current status. The Lancet series demonstrates that the occupation by the Israeli state is the major determinant of the health problems for Palestinian children, together with internal governance failures and lack of resources.4
Organisation of healthcare for Palestinian children
The main provider of healthcare is the Palestinian Ministry of Health that provides primary care services for children up to 5 and secondary care in hospitals in the West Bank and Gaza (the Ministry of Health operates 24 of 78 hospitals in Palestine). However, there are also several other providers of healthcare:
UNRWA that provides primary healthcare for Palestinian refugees.
Non-governmental organisations that are major providers in tertiary care services especially in Jerusalem and offer secondary care services and to a lesser extent some primary healthcare services.
Palestinian Red Crescent that provides ambulance services and some clinics.
The private sector that covers private doctors and is a new sector in providing health services in Palestine.
There is a lack of effective co-ordination between these different sectors, and also a severe deficiency of services for child protection, mental health and child disability. There is also a shortage of medical staff in sectors such as family practice (particularly with an orientation to children), neurology, oncology, paediatric surgery and psychiatry. Most doctors wishing to specialise will need to leave the country to access training in the Gulf States, Europe and Russia and many do not return.
According to Giacaman et al,3 there is a general problem of low quality of care in the health sector owing to ‘restricted mobility inhibiting effective health-system function, management, and accountability; the presence of underqualified healthcare providers; and weak institutional capacity for monitoring and assessment’.
What are the health problems of Palestinian children?
The health profile for Palestinian children represents a population affected by poverty, migration, conflict and environmental degradation.5
Forty per cent of the population is under 18 years, and the population growth rate is extremely high at over 3%.6
Mortality rates
Under-five mortality (UFM) is accepted as a central indicator of child health and is used in comparison between neighbouring countries. Historical data for Palestine are difficult to obtain as it was only in 2012 that Palestine was given observer status at the UN. In 2014,7 the UFM in Occupied Palestinian Territories (OPT) was 22 per 1000, and a reduction from 38 per 1000 in 1990. This placed the OPT beside countries such as Algeria (25) and Egypt (25) and markedly worse off than Israel (4) and Lebanon (8).8 Unicef noted that OPT had the fourth fastest rate of reduction of UFM in the Arab world after Egypt, Oman and Libya.
Data from the Ministry of Health on UFM show that prebirth-related complications (premature or low birth weight births) accounted for 44% of child deaths in 2007, while congenital abnormalities accounted for 13%. Respiratory infections and congenital abnormalities are key causes of death. The rate of child mortality caused by respiratory infections was 5%. For children ages 1–4, accidents contribute 27.7% of total deaths, with traffic accidents amounting to 11.7% (figure 1).
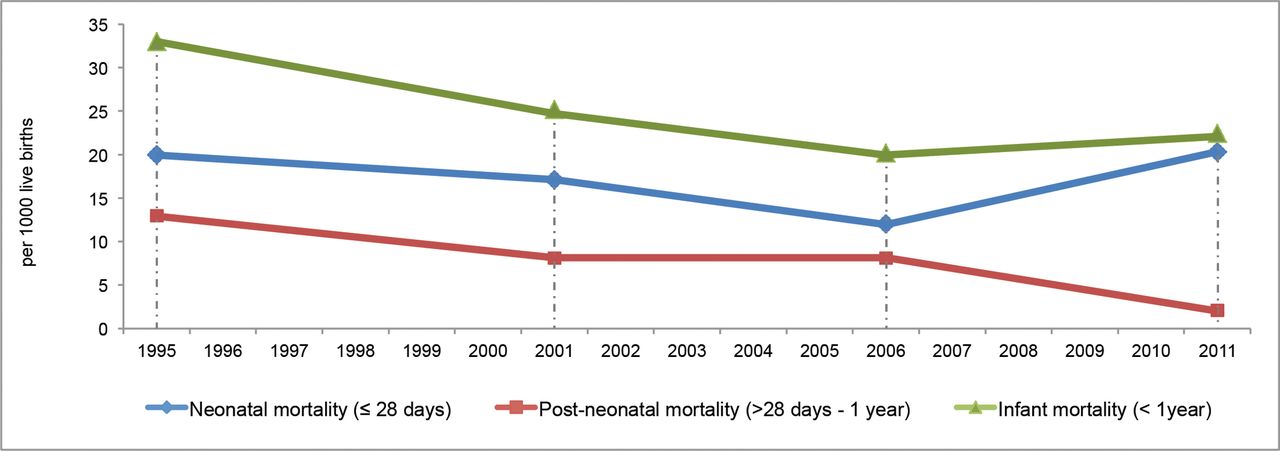
Neonatal and infant mortality9 in Palestine.
Main causes of morbidity
In general, health problems in Palestine are not markedly different from other countries in the region. However, the social determinants of health of children in Palestine are affected by the ongoing burden of living under occupation and siege as well as a state of chronic stress due to acts of violence against a whole nation including children. Unemployment as reported by the World Bank in 2016 remains at 27%: 42% in Gaza and 18% in the West Bank, resulting in a poverty rate of at least 25% and deep poverty rate of 18%.10
These determinants have influenced morbidities including nutritional disorders, mental health, accidents, violence against children and disabilities.
Nutrition
Malnutrition figures prominently and stunting has been increasing particularly in Gaza where it has risen to 13%. According to Rahim et al,11 stunting has been rising since 1996 from 6.7% to 7.9% in the West Bank and from 8.2% to 13.2% in Gaza. The prevalence of underweight and wasting has changed little. In Gaza, the food situation is precarious with 56% of the population classified as food insecure compared with 25% in the West Bank.
Iron deficiency has been reported as being very common in young children in Gaza (see below in Special situation in Gaza).
Mental health
A study in 200312 found that 93% of children had experienced being or feeling threatened, a loss or a lack of security, and fear. Parents also reported many psychological symptoms in their children such as nightmares, enuresis, and high levels of aggressive behaviours, hyperactivity, low attention and concentration. A survey13 of Palestinian adolescents in school investigated collective and individual exposures to violence and its negative effect on adolescents’ mental health. The level of exposure to trauma and violence was very high. The experience of the teenagers was horrific: 80% had seen shootings, 28% had seen a stranger killed, 11% had seen a friend or neighbour killed and 54% of boys had experienced body searches. Not surprisingly, 10.4% of the participants had a depressive-like state, 14.1% emotional difficulties and 10.3% somatic disorders.
Accidents
The accident mortality in children under 14 years in 2009 was 12.1 per 100 000. Shaheen showed that the leading cause of injury mortality in Palestinian children under 14 years is road traffic accidents (4.2) followed by firearms missiles (3.9), drowning (1.5) and falls (1.4). The rate for missile injuries was nearly twice in Gaza over the rate in the West Bank.14
Violence against children
Over 1800 children have been killed as a result of occupation policies and practices since the year 2000.
Between 2006 and 2012, Defence for Children International (DCI)-Palestine documented 26 cases of children being recruited by armed Palestinian groups.
Since 2000, at least 8000 Palestinian children have been arrested and prosecuted by the Israeli military.15 The children detained have been subjected to systematic ill treatment and torture.
Specific techniques used regularly by Israeli interrogators on Palestinian children include a combination of: excessive use of blindfolds and handcuffs, beatings (slapping and kicking), sleep deprivation, solitary confinement. denial of food and water for up to 12 hours, denial of access to toilets, denial of access to a shower or change of clothes for days or weeks, exposure to extreme cold or heat, position abuse, yelling and exposure to loud noises, insults and cursing. 16
Violence at home and in school are also common in the OPT. Over 50% of mothers reported that one of their children between 5 and 17 years had been exposed to violence either at home (93%) or at school (45%).7
A survey by the UN Girls Education Initiative17 showed that physical and verbal violence by teachers (and sometimes by pupils themselves) is experienced by over half the students in West Bank schools.
However, it is injuries from violence by Israeli security forces which are most concerning. Unicef reported in 201518 that during the last quarter, 25 Palestinian children were killed and 1310 injured across the country, the majority in the West Bank or East Jerusalem.
The following is taken from an article19 in the New York Review of Books by David Shulman, Professor Emeritus at the Hebrew University of Jerusalem, 22 June 2017:
‘Children from the Twaneh area [West Bank] are at constant risk of being attacked by settlers on their way to school in the village; the daughter of a friend of mine, Ali from Tuba, nearly lost an eye in such an attack. The army has been forced to provide a military escort to take them to and from school, but even that is not always enough; there have been occasions when the soldiers stood idly by while settlers beat the Palestinian children with clubs and metal chains.’
Violation of children’s rights
According to Defence for Children International,20 between 500 and 700 Palestinian children are detained and prosecuted every year by Israeli security forces, usually for stone throwing. During 2016, the monthly average of children between 12 and 17 held in detention was 375, the highest figure in the last decade.
Case study
Shayma, 13, whose home was destroyed during the 2008–2009 military offensive on Gaza21:
Before the offensive, I had my own room. I had pictures of Barbie posted in every corner of my room. Now I sleep with my three sisters and three brothers in the same area. Before the offensive, I used to go to school, come back, have a shower, eat, study and then sleep. Now I go to school and come back without taking a shower because we always have a water shortage. I don’t study, because I’m not comfortable. I don’t feel at home at all. I stopped doing all the things I like, such as drawing and playing. I don’t even like watching TV now, which was my favourite hobby of all. My academic achievement is much worse than before the offensive. I was getting very good marks but now I’m not that good at all, and I’m afraid that now I won’t be able to be a doctor.
Disability
Up-to-date data are not available on the prevalence of childhood disability in Palestine although it is estimated by the Palestine Central Bureau of Statistics 2011 survey22 that 1.5% of children aged 0–17 years were disabled, with a higher incidence among males (1.8%) than females (1.3%). It is known that the conflict has contributed greatly to conditions such as loss of limbs, serious head injuries and post-traumatic stress disorder.
There is also a high prevalence of congenital disorders related to consanguinity which is common in the Palestinian population, and these conditions are associated with learning disability.
What are the determinants of the health problems?
According to Horton,4 the causes of the Palestinian predicament are complex—occupation, internal governance failures, absence of resources, actions and inactions of the international community, aid dependency and a rapid epidemiological transition.
As a country under occupation, the main social determinants of health for Palestinian children are the socioeconomic circumstances in which they live, the limitations in access to healthcare, the impact of the occupation on daily living and availability of food, electricity and adequate housing, and everyday occurrence of violence which impacts on children as much as on adults.
According to Medical Aid to the Palestinians (MAP),23
Israel’s policies inhibit the construction and maintenance of medical infrastructure and the essential services needed to promote health, such as water, sanitation and electricity. Restrictions on free movement between different areas of the oPt (the West Bank, including East Jerusalem, and Gaza) limit the access of health workers to training and professional development. Restrictions on access to medical equipment and materials further prevent the development of services in some areas of the OPT.
What are the barriers in access to healthcare for Palestinian children?
Permits
The occupied Palestinian territories are divided into three areas: the West Bank, East Jerusalem and Gaza. If a patient requires to be transferred from one area to another—usually into East Jerusalem, where the main tertiary specialist Palestinian hospitals are sited—a special permit must be obtained from the Israeli authorities. Frequently, permits are refused on ‘security grounds’. Over 100 000 patients sought permits in 2014–2015; between 2012 and 2016, the percentage receiving a permit to cross from Gaza to East Jerusalem has fallen from 92% to 64%.
Research by Medical Aid to the Palestinians24 has shown that the reasons for refusing a permit to a Gaza patient may be age (particularly 18–45 year olds), gender (men are more likely to be refused), patients with family considered to be a security risk and patients requiring non-life-saving treatment. Patients only find out if their application was successful, the evening before they are due to travel.
Augusta Victoria hospital in East Jerusalem offers the only treatment for hemato-oncology, radiation and nephrology services for children.
Due to restriction in permits and for males most of the children receive their care accompanied by a grandmother or an aunt adding to the psychological burden of children and violating further their rights in accessing care supported by their parents.
Since 2007, Augusta Victoria Hospital in Jerusalem has run a free bus service from the South of the West Bank for the patients and children who come for dialysis—they are able to stay on the bus and not have to walk across checkpoints.
According to the WHO,25 40% of requests to exit Gaza for medical appointments were denied or delayed by the Israeli authorities in February 2017. The approval rate for such travel requests has declined year on year since 2012, when 8% of such requests were denied or delayed.
According to Physicians for Human Rights–Israel,26
‘since January 2016 there has been a disconcerting rise in number of medical permit denials that Gazan patients receive. In particular, PHRI data showed a dramatic increase in these denials among cancer patients'.
Checkpoints
Ambulance to ambulance transfer
The Israeli government does not normally allow Palestinian patients, even emergency cases or those receiving critical care, to enter East Jerusalem from the West Bank freely even in a Palestinian registered Red Crescent ambulance.
Hence, if a patient is being transferred from a West Bank Hospital to a hospital in Jerusalem (the site of specialised facilities), the patient must be transferred from the ambulance to another either Palestinian or Israeli ambulance back to back at the check point figure 2. A study by MAP27 has shown that emergency transfers incur an average delay of 27 min, which clearly could make the difference between life and death in emergency cases.

Illustration of Bethlehem checkpoint.
Health infrastructure
In area C (60% of the West Bank where Israel maintains full military and civil control), Palestinians are normally prevented from building permanent hospitals or health centres so none exist for the 300 000 population.
In Gaza, the constant cycle of bombardment and attempted rebuilding has lead to the destruction of 17 hospitals and 56 primary care centres (figure 3).26 Some have been rebuilt but there is currently no dedicated rehabilitation hospital as the existing one was completely destroyed.

{kind=link}
{kind=link}
{kind=link}
Illustration of destruction in Gaza
Medical materials
Gaza faces severe equipment and stock shortage and in May 2017, 34% of essential medicines and 32% of medical disposables were at ‘zero stock’ in Gaza, meaning that less than a month’s supply was available. Among the 170 items affected were medications used to treat cancer and immunological diseases, and medical disposables needed for use in operating rooms, emergency departments and intensive care.27
Medical and nursing training
Medical and nursing training outside Palestine is limited by the difficulties which health personnel have in obtaining permits to travel, even to overseas conferences or on fellowships. This also applies to travelling to East Jerusalem where six specialised Palestinian hospitals are located.
Between 2015 and 2016, the number of permits approved for Palestinian health personnel to travel through Israeli checkpoints dropped by 28%, from 6914 to 4985. A MAP study28 has also shown that travel to other countries may be restricted by the visa requirements of their governments, including UK, Jordan and Egypt.
The special situation in Gaza
Currently, the population of Gaza (some 1.8 million people) are facing a critical situation in relation to income, food availability, electricity, water and not least, healthcare.25–28
Case study
Al Mezan Center for Human Rights reported that Aya Khalil Abu Metalq, aged 5 years, died on 17 April 2017 due to lack of treatment for a metabolic disorder. Israeli authorities twice failed to respond to requests submitted by Aya’s family to travel to appointments at Al Makassed Hospital in East Jerusalem.28
According to the Ministry of Health (MoH), 55% of medications used to treat blood diseases and cancers were at critical levels.
MAP’s team in Gaza has also highlighted particular scarcity of special formula milk for babies with phenylketonuria disorder—an inherited disorder which affects metabolism of certain amino acids—at Gaza’s Central Drug Store.
Iron deficiency has been reported in 33.5% of kindergarten children living in marginalised areas of Gaza.29
The UN has reported that chronic fuel shortages mean that hospitals are only able to provide the most critical services such as intensive care. Elective surgeries are being put on hold, and sterilisation and cleaning services have been reduced, increasing the risk of complications and infections for patients.
The UN has also stated that the number of patients being referred outside of Gaza is increasing.
New initiatives in Palestinian healthcare
Palestinian health workers are not victims waiting for others to solve their problems. They are self determining professionals who urgently seek to devise new alliances to protect the future of their communities and to inform their politicians with the best available evidence and data to guide health system reform. Horton R, Lancet March 7 20094
The 2014 attacks on Gaza caused many injuries too complex to be treated within the local health system. With a local partner, MAP established a permanent limb reconstruction unit staffed by local surgeons and nurses at Al Shifa Hospital, securing the future of post-traumatic and reconstructive surgery in Gaza.
In Gaza, a neonatal network was established to address neonatal care in order to organise efforts of different donors and missions to support effective neonatal care.
A training programme is being developed by the Palestinian Paediatric society with the assistance of the Royal College of Paediatrics and Child Health (RCPCH) in UK to enhance capacity among doctors, therapists, nurses and community workers in the multidisciplinary assessment and treatment of children with disabilities and special needs. This builds on a previous RCPCH programme30 with Al Quds Medical School to develop first a Diploma in Child Health and later a Master of Child Health for doctors and nurses in primary care, using small group teaching facilitated by local tutors. The aim of this programme was to improve the quality of paediatric primary care which was widely considered to be imperfect.
There is a huge potential for effective and high-quality healthcare to be developed in Palestine, whereas the constraints of the occupation and the urgent need for a permanent peace place a severe limitation on achieving this goal. There is a responsibility for health workers and others around the world to show solidarity with the Palestinian people and advocate strongly for the removal of the occupation and the institution of an independent Palestinian state.
Footnotes
Contributors TW conceptualised and designed the study, collated references, drafted the initial manuscript, and reviewed and revised the manuscript. DN commented on the design, collated references and examples, and reviewed and revised the manuscript.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed.
Data sharing statement Any unpublished data are freely available to all readers.