Article Text

Abstract
Objective To understand the prevalence of pneumonia risk factors and perceived barriers to risk factor reduction among Vietnamese infants.
Methods We conducted a cross-sectional survey of mothers in the postnatal wards of Da Nang Hospital for Women and Children in central Vietnam from 10 February 2017 to 24 February 2017.
Results Of 286 mothers surveyed, 259 (91%) initiated breast feeding and 207 (72%) intended to continue exclusive breast feeding for 6 months. No mother smoked cigarettes, but 42% of fathers did. Mothers’ decision not to smoke was motivated by concerns for their own health and that of their baby. Households rarely used wood or coal for cooking (6%). Mothers indicated near universal (99%) uptake of the National Expanded Program of Immunization vaccinations. Few (64; 22%) mothers knew about the pneumococcal conjugate vaccine; 56/64 (88%) indicated that they would purchase it for their infants. Family members rarely influenced mothers’ decisions about breast feeding or vaccination, except in two instances where fathers were concerned about vaccine-related adverse effects.
Conclusion Modifiable pneumonia risk factors were uncommon among newborn babies in central Vietnam, apart from paternal cigarette smoke exposure. Successful local implementation of the WHO Essential Newborn Care package as well as high levels of maternal education and decision autonomy was observed.
- Immunisation
- Infant Feeding
- Respiratory
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Pneumonia is a common cause of morbidity and mortality in young children in Vietnam and worldwide.
The WHO recognises lack of breast feeding, cigarette smoke or indoor air pollution exposure and vaccination as major modifiable risk factors for child pneumonia.
Previous studies showed low rates of exclusive breast feeding, with high cigarette smoke and indoor air pollution exposure in Vietnam.
What this study hopes to add?
We demonstrated a low prevalence of modifiable pneumonia risk factors, except for paternal cigarette smoke exposure, among newborn infants in central Vietnam.
High breastfeeding initiation rates reflect recent successful implementation of the WHO Essential Newborn Care package at Da Nang Hospital for Women and Children.
Mothers had high levels of education and displayed strong decision autonomy regarding what is best for their baby.
Background
Pneumonia is a common cause of death in young children worldwide.1 2 An estimated 900 000 children less than 5 years of age died because of pneumonia in 2015, with more than 90% of these deaths occurring in low-income and middle-income countries.3 In 2015, 14% of under-5 deaths in the Western Pacific region were attributed to pneumonia,4 with the majority (>75%) of pneumonia-related deaths occurring in six countries: Cambodia, China, Laos, Papua New Guinea, the Philippines and Vietnam.5 Despite recent progress, the pneumonia disease burden in Vietnam remains nearly 10 times higher than in developed country settings like Australia and Europe.6 Efforts to reduce pneumonia-related morbidity and mortality in young children usually focus on vaccine-preventable causes and improved case management. In Vietnam, conjugated Haemophilus influenzae type B (Hib), measles, pertussis and BCG vaccination is provided free of charge by the National Expanded Program of Immunization (EPI). In general EPI uptake is excellent, although national Hib roll-out has only recently been achieved.4 7 The use of pneumococcal conjugate vaccine is advised in national guidance documents, but it is not provided free of charge in Vietnam and coverage is low.8
Apart from vaccination, primary prevention is rarely emphasised in settings that are dominated by income-generating healthcare models, and often low on the priority list of developing countries with poor regulatory frameworks. The WHO recognises lack of breast feeding and cigarette smoke or indoor air pollution exposure as major modifiable risk factors for child pneumonia.9 10 In Vietnam, previous studies reported that less than 30% of mothers exclusively breast fed during the neonatal period11 and less than 10% sustained exclusive breast feeding for up to 6 months of age.12–14 Although the health benefits of exclusive breast feeding, including significant reductions in infant pneumonia and death, are undisputed,15 many barriers compromise exclusive breast feeding during the first 6 months of life. Identified barriers include difficulties in establishing breast feeding, sociocultural factors and family expectations, as well as feasibility issues, inappropriate marketing of infant formula and poor health education.12 14 16 Studies from Vietnam listed ‘working away from home’, ‘Caesarean section (C-section)’ and ‘maternal grandmother or husband preferences’ as factors that reduce exclusive breast feeding.17–20
Exposure to parental smoking increases the risk of severe pneumonia in children21 22 and is an independent risk factor of poor outcome.23 In addition, indoor air pollution associated with the use of biomass fuel in homes is strongly associated with pneumonia-related mortality in children.24 25 Given the high burden of child pneumonia in Vietnam, there is a need to better understand the prevalence of pneumonia risk factors and perceived barriers to risk factor reduction, especially in central Vietnam where sociocultural practices are poorly documented.
Methods
We conducted a prospective cross-sectional survey of mothers in the postnatal wards, within the first few days after delivery. The study was approved by the ethics review board at Da Nang Hospital for Women and Children (approved 26 August 2016) and performed over a 2-week period (10 February 2017 to 24 February 2017). All participating mothers provided written informed consent.
Study setting
The Da Nang Hospital for Women and Children is a regional hospital in central Vietnam with 1400 inpatient beds. It is the largest provider of obstetric services in Da Nang City with around 14 000 deliveries each year. It also serves as the regional referral hospital for women and children. Pregnant women may come directly from home or be transferred from surrounding district and provincial hospitals to deliver their baby. The Da Nang Hospital for Women and Children recently implemented (fully implemented since November 2014) the WHO Essential Newborn Care (ENC) package,26 which encourages early breastfeeding initiation.
Data collection and analysis
All mothers who were present in the postnatal wards when the researchers made their daily visits were recruited, if they provided informed consent to participate. Data were collected by the first author (NTKP) and a research assistant, neither of whom were involved in the clinical care of the mothers interviewed. Interviews were done in private without participation of staff members to limit possible social desirability bias. There were no exclusion criteria, and mothers were recruited irrespective of their date or mode of delivery (including vaginal deliveries and C-sections). However, recruitment only occurred in the general maternity wards, which effectively excluded mothers that required high-level care themselves or had infants that required neonatal intensive care. We recorded basic demographics (age, education level, address, type of delivery and reason for refusal) from mothers who declined participation or were otherwise unavailable for recruitment (not present in their rooms when the study team visited). Data were collected on a detailed questionnaire administered in Vietnamese by the investigator or trained assistant (see online supplementary questionnaire) .
Supplementary file 1
The questionnaire content was developed to focus on important modifiable risk factors for childhood pneumonia identified by the WHO. The questionnaire was translated into Vietnamese and back translated into English by a second independent translator to optimise the accuracy of the translation. A small group of Vietnamese mothers assisted questionnaire development to ensure that questions were correctly interpreted in the local cultural context. Further refinements were made after pilot testing was done on the maternity ward at Da Nang Hospital for Women and Children. Pilot testing occurred over a period of 3 days and involved more than 30 mothers. All questions were critically assessed and revised where necessary to improve efficiency, standardise data collection procedures and limit possible misinterpretation. Data quality checks were performed at the end of each day before entry into an Epidata database.27 Descriptive analyses were performed using SPSS (V.24). Comparative analyses of factors that affected exclusive breast feeding will be presented separately.
Results
In total, 573 mothers were admitted to the postnatal wards during the 2-week study period, of whom 302 were approached and 286 (53%) completed the postnatal questionnaire (figure 1). Only 16 (3%) mothers declined study participation, mostly because they were too tired to be interviewed. The age categories, occupation, mode of delivery and rural or urban origin were similar between study participants and those who were not enrolled (online supplementary file 2). All study participants were from the majority Kinh ethnic group.
Supplementary file 2

Study recruitment flow diagram.
Table 1 reflects the demographics of mothers who completed the questionnaire. Most (185; 65%) mothers were in the 25–34 age category; only one mother was less than 18 years and 16 (6%) were older than 40 years of age. Mothers were generally well educated, 64% attended college or university after high school completion and 55% were employed. Only one mother was HIV infected. Around half of mothers (55%) were primigravidas. Table 2 describes the characteristics of the newborn infants and the healthcare that they received. The mean age of babies were 2.8 days (range: 1–5) with more boys than girls (55% vs 46%). More than half (162; 57%) were born by C-section, 55%) and 95% fell in the normal weight range; 5% were preterm.
Demographics of mothers who completed the postpartum questionnaire
Characteristics of babies born to mothers who completed the postpartum questionnaire
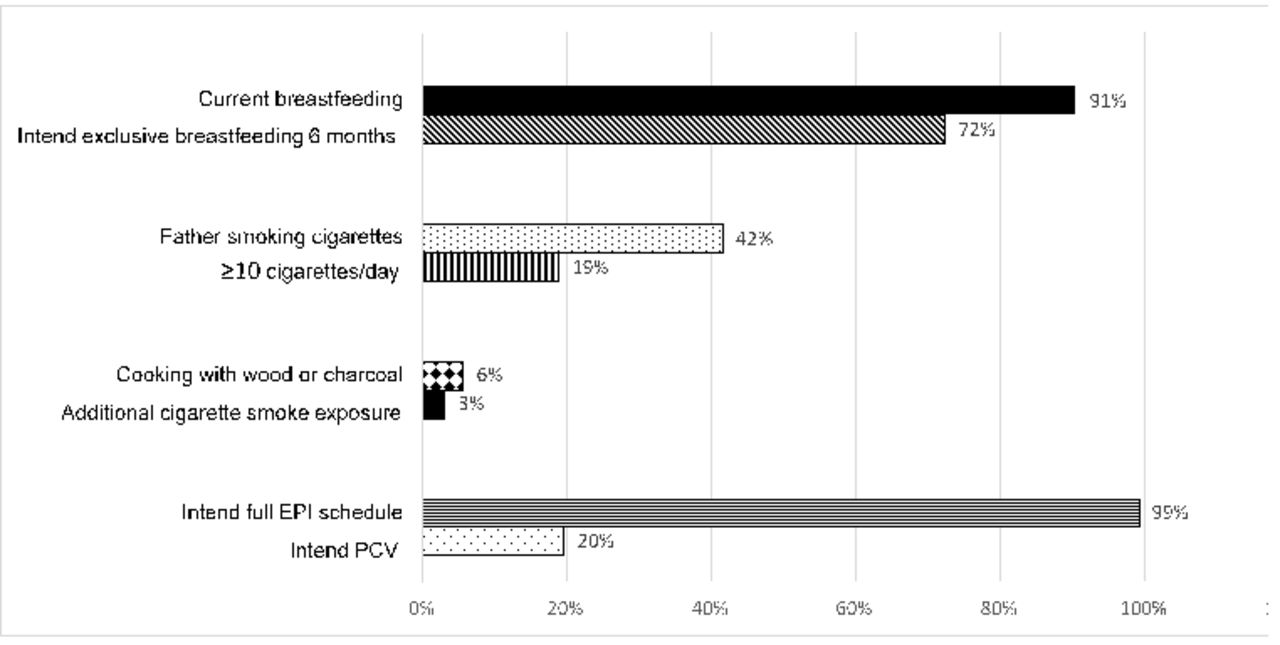
Figure 2 provides an overview of common pneumonia risk factors reported during the interview. At the time of interview, 259 (91%) mothers had initiated breast feeding and 207 (72%) indicated that they intend to breast feed exclusively for 6 months. Not a single mother smoked cigarettes. Most mothers indicated consideration for their own health and that of their newborn baby as the main reasons for not smoking (table 3). By contrast, (120/286, 42%) of fathers smoked with a third (33/120, 28%) smoking more than 10 cigarettes per day; 23 (19%) smoked inside the house. We did not record data on other family members who may smoke in the house. Few families used wood (14, 5%) or charcoal (2, 1%) for cooking, and only 4 (1%) reported use of biomass fuel inside the house.
{kind=link}
{kind=link}
Key pneumonia risk factors assessed during maternal postnatal interview. EPI: Expanded Program on Immunization; PCV: pneumococcal vaccine. Percentages were calculated based on the frequencies of each risk factors with 286 as nominator.
Reasons mothers identified for not smoking cigarettes
Table 4 summarises the mothers’ knowledge of key pneumonia risk factors, with most mothers providing correct answers to basic questions on breast feeding and smoke exposure. As for vaccination, 284 (99%) mothers indicated that they intended adherence to the full EPI schedule. Of the non-EPI vaccines, 165 (58%) mothers were aware of the measles, mumps and rubella (MMR) vaccine; 56% intended to provide this to their child. Only 64/286 (22%) mothers were aware of the pneumococcal conjugate vaccine and 56/286 (20%) intended to provide this to their infant. Table 5 provides an overview of factors that influenced mothers’ vaccination decisions. Mothers were mainly motivated by the fact that vaccines will protect their own babies, although there was awareness that ‘everyone should vaccinate their children" to protect the community. Only two mothers expressed fear of vaccine-related adverse effects and indicated that they will not vaccinate their children; their decisions were mostly influenced by concerns that their husbands expressed.
Mothers’ responses to questions on risk factors for child pneumonia
Factors that influenced mothers’ vaccination choices for their babies
Discussion
To our knowledge, this is the first study to explore the prevalence of pneumonia risk factors among newborn babies in central Vietnam. The rate of successful breastfeeding initiation and intent to continue exclusive breast feeding for 6 months among mothers was very high compared with national average estimates of 17% exclusive breast feeding for the first 6 months of life (in 2007–2014).4 The high rate of breastfeeding initiation is likely a reflection of recent adoption of the WHO Essential Newborn Care package at the Da Nang Hospital for Women and Children. The care package encourages healthcare professionals to assist mothers with breast feeding within the first hour after giving birth, together with regular skin-to-skin contact initiated at the time of delivery.26 The hospital also provides mothers with knowledge on exclusive breast feeding through antenatal and postnatal consultation services.
The percentage of babies exposed to cigarette smoke at home was comparable with worldwide estimates (40% in 2011)28 and slightly lower than national estimates for Vietnam (48% in 2012).10 The fact that only fathers were reported to smoke cigarettes concurs with high male smoking rates in Vietnam. In 2015, an estimated 36% of males in Vietnam smoked cigarettes compared with a global average of 25%.29 It has been estimated that nearly a third (29%) of child pneumonia cases and 44 000 paediatric hospitalisation events in Vietnam can be attributed to passive cigarette smoke exposure.30 In utero exposure to cigarette smoke, or indoor air pollution, has also been associated with an increased risk of child pneumonia.25 31 32 However, studies showed that having a non-smoking mother significantly reduces the risk of hospitalisation from childhood pneumonia.33 None of the mothers interviewed indicated that they smoke cigarettes, which is consistent with local clinical experience. The fact that mothers were motivated by concern for their babies health indicates that they could potentially also influence fathers to stop smoking. Although indoor air pollution is a major concern globally, very few families in our survey cooked with wood or charcoal and less than 2% burned biomass fuel inside the house. This figure is much lower than national solid fuel cooking rates of 47%, reported for Vietnam in 2013,4 which may be partly explained by the absence of minority ethnic groups from the study population.
In the study setting, BCG vaccination was not provided in hospital, but in the community during the first month of life.34 In countries with high rates of tuberculosis, WHO recommends that BCG vaccination should be provided at birth (before hospital discharge).34 35 Vietnam has a high tuberculosis incidence (137/100 000 population) indicative of ongoing community transmission, as well as high rates of drug resistant tuberculosis.36 Infant BCG vaccination provides important protection against disseminated forms of disease, including drug-resistant tuberculosis, during the first 2–3 years of life.37 There is room to consider whether BCG should best be administered before hospital discharge, but current arrangements are working well with good BCG uptake (95%, 2016)7 and low tuberculosis disease rates among young children.
Additional pneumonia risk factors such as prematurity, low birth weight and HIV infection were uncommon in the study cohort; only one infant was born to an HIV-infected mother. The percentage of babies born by C-section was much higher than previous reports from Southern Vietnam (40%)20 and other countries in the region (Cambodia 3%, Laos 4% and the Philippines 9%).4 Da Nang Hospital for Women and Children is a regional referral hospital with a more complex patient mix; however, C-section rates in Vietnam are generally higher than in neighbouring countries, which may reflect differences in local clinical guidance and cultural expectations. It should be acknowledged that unnecessary C-section is a risk factor for neonatal respiratory distress and possible pneumonia.
Only two mothers indicated serious concerns regarding vaccine-related adverse effects. Most mothers were very keen to ensure that their children received the full EPI vaccination schedule. While many mothers planned to provide their children with MMR vaccination, in addition to measles vaccination provided by the EPI, few mothers had knowledge of newer pneumococcal conjugate vaccines. Of those who are new about pneumococcal conjugate vaccines, the majority planned to purchase this out of their own pocket. Vietnam has not yet indicated whether MMR or pneumococcal conjugate vaccines will be included in the state-sponsored EPI schedule. Previously documented barriers to vaccination uptake include mothers from socioeconomic disadvantaged backgrounds, ethnic minorities, rural areas or those with limited education.38 Of particular interest is the large degree of decision autonomy exercised by mothers, most of whom were primigravidas. Only a small minority indicated that family members or health professionals had a strong influence on their decisions to breast feed or vaccinate their children. Most mothers consulted with their husbands, mothers and healthcare professionals but indicated that they made the final decision themselves. The fact that mothers demonstrated a high degree of decision autonomy is encouraging and probably reflect their high education status and improved health literacy.
Our study was limited by the fact that we failed to interview a large number of mothers who delivered during study period. However, we purposefully guarded against selection bias and demonstrated comparable demographics among mothers who were interviewed and those not included in the study. Interviews were done within the first few days after delivery, and the hospital environment may have influenced mothers to provide the answers that they thought healthcare providers wanted. We tried to limit affirmation bias by framing all questions as objectively as possible and utilising study personnel who were not involved in the patient care. Our study did not include anyone from a minority ethnic group and therefore none of the study findings can be extrapolated to these populations, who may have increased exposure to indoor air pollution, lower health literacy and different barriers to vaccine uptake. It should also be emphasised that we only captured mothers’ stated intent, without measuring their actual behaviour. However, we believe that the responses provided were truthful and provide useful insight into pneumonia risk factor exposure.
In conclusion, we documented a low prevalence of modifiable pneumonia risk factors, except for paternal cigarette smoke exposure, among newborn infants in central Vietnam, associated with high levels of maternal education and decision autonomy. High rates of breastfeeding initiation reflect recent successful implementation of the WHO Essential Newborn Care package at Da Nang Hospital for Women and Children.
Acknowledgments
We would like to thank all the women who kindly agreed to participate, the staff at postnatal wards in Da Nang Hospital for Women and Children for supporting during the study period. Especially, we would like to thank mid-wife Le Thi Nhu Quynh and Tran Thi Xuan Oanh who helped with data collection.
References
Footnotes
Contributors All authors contributed to the design of the protocol and questionnaire. NTKP collected the data. NTKP and BJM conceptualised the manuscript and wrote the first draft. All authors gave constructive inputs and approved the final manuscript.
Funding No project funding received. Da Nang government provided an international PhD scholarship to the first author (NTKP).
Competing interests None declared.
Patient consent Obtained.
Ethics approval Da Nang Hospital for Women and Children Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.