Article Text

Abstract
Background Low blood glucose levels (BGLs) in infants are known to adversely affect neurodevelopmental outcomes. However, this risk is not well explored in infants with hypoxic ischaemic encephalopathy (HIE) that receive therapeutic hypothermia (TH). Additionally, little information is available on the optimal BGLs to target in infants with HIE.
Aim To explore the association between hypoglycaemia and neurodevelopmental outcomes at different BGL thresholds (2.6 and 3.0 mmol/L) in neonates with HIE treated with TH.
Methods Retrospective cohort study. Clinical information and 2-year neurodevelopmental data using Bayley Scales of Infant Development, third edition (BSID-III) and disabilities were recorded for infants born in Western Australia with HIE and treated with TH between February 2008 and February 2012. Multivariable logistic regression models explored the association between hypoglycaemia and neurodevelopmental outcomes.
Results 122 infants underwent a total of 1616 BGL estimations before and during 72 hours of TH. Hypoglycaemia (BGL<2.6 mmol/L) occurred in 38/122 (31%) infants and 11/122 (9%) had recurrent hypoglycaemia (three or more episodes). Infants with recurrent hypoglycaemia (<2.6 mmol/L) had significantly lower mean BSID-III cognitive, language and socioemotional subscale scores. On multivariable analysis, recurrent hypoglycaemia (<2.6 mmol/L) was associated with increased odds of death or disability (adjusted OR 8.15; 95% CI 1.31 to 50.58; p=0.024). Recurrent hypoglycaemia (<3.0 mmol/L) during the first 12 hours of life was also associated with severe disability among survivors (adjusted OR 11.13; 95% CI 2.06 to 59.89; p=0.005).
Conclusions Early recurrent hypoglycaemia was associated with increased risk of death or severe disability in neonates undergoing TH for HIE. Prospective studies are needed to identify the ideal target BGL in this population.
- neurodevelopment
- neonatology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Infants with hypoxic ischaemic encephalopathy (HIE) are at high risk of neurodevelopmental disability.
Hypoglycaemia in HIE may increase the risk of unfavourable neurodevelopmental outcomes.
This risk is not well explored in infants who receive therapeutic hypothermia.
What this study hopes to add?
Hypoglycaemia is common in patients with HIE.
Avoiding recurrent hypoglycaemia in infants with HIE is important to reduce secondary brain injury.
We hypothesise that targeting blood glucose levels >3.0 mmol/L may reduce the risk of unfavourable outcomes in these infants.
Introduction
Hypoxic ischaemic encephalopathy (HIE) in newborn infants is associated with high rates of mortality and neurodevelopmental morbidity.1–3 Therapeutic hypothermia (TH) is known to improve short-term and long-term outcomes and has become the standard of care for moderate to severe HIE.4–6 Glucose control is an important management goal in intensive care units with studies showing that hypoglycaemia is associated with poor neurodevelopmental outcomes.7–9 However, there is controversy over the definition of hypoglycaemia in neonates with HIE.10–12 There are only four studies that have explored the effect of hypoglycaemia on the outcomes of neonates with HIE or suspected asphyxia,13–16 of which two studies included neonates with HIE that received TH.14 16
Hence we aimed to further explore the relationship between hypoglycaemia and neurodevelopmental outcomes in neonates with HIE that received TH. Another aim was to examine whether targeting higher blood glucose levels (BGLs) may reduce the risk of adverse neurodevelopmental outcomes.
Methodology
This was a population-based retrospective case-control study of all neonates with HIE and managed with TH in Western Australia (WA) between February 2008 and February 2012. During this period all infants with HIE that required TH in WA were managed in the neonatal intensive care units (NICU) of Princess Margaret Hospital for Children (PMH) or King Edward Memorial Hospital for Women (KEMH). Both units function as a single clinical care unit and follow the same management protocols. Neonates with HIE were started on a maintenance intravenous infusion of 10% dextrose at 50 mL/kg/day without enteral feeds. A BGL below 2.6 mmol/L was managed with an intravenous bolus of 2 mL/kg of 10% dextrose and the maintenance infusion increased by 10–20 mL/kg/day with a repeat BGL within 60 min. If the total fluid rate reaches 80–90 mL/kg/day then the concentration was incrementally increased by 5%. Hyperglycaemia was managed by reducing glucose infusion rates; insulin was not administered to any infant in this study. The majority of neonates were outborn and transferred to PMH or KEMH by the Newborn Emergency Transport Service of WA, which is based within the PMH neonatal unit and advise the same protocol as above when calls for transfer are received.
The cohort was identified using the neonatal database at both NICUs. All infants who were ≥35 weeks postmenstrual age with HIE and treated with whole body TH were included in this study. TH was commenced in infants ≥35 weeks postmenstrual age that were less than 6 hours old, had moderate or severe encephalopathy based on the Sarnat Grading Scale17 and had evidence of asphyxia as defined by the presence of at least two of the following criteria: (1) Apgar score <6 at 10 min or continued need for resuscitation with positive pressure ventilation or chest compressions at 10 min, (2) any acute perinatal event that may result in HIE (ie, placental abruption, cord accident, prolonged fetal bradycardia, etc), (3) cord blood (or if cord blood is not available, arterial blood sample within 60 min of birth) with a pH <7.0 mmol/L or base deficit of 12 or more. Some infants with mild HIE received TH because of initial uncertainty of the severity of the encephalopathy prior to or during transfer. Some of these infants were subsequently reclassified to Sarnat grade 1 encephalopathy by the clinical team but completed 72 hours of cooling. These infants were included in the final analysis.
Infants were excluded if they had an inborn error of metabolism or congenital structural brain defect. Our unit protocol was to measure BGLs at least four hourly in the first 24 hours and then six hourly until the end of TH. More frequent measurements were undertaken in infants with poor glucose control.
The demographic, BGLs and 24-month neurodevelopmental outcome data were recorded. All BGLs from birth until the end of the 72 hours cooling period were recorded. Hypoglycaemia was defined as BGL <2.6 mmol/L,10 and hyperglycaemia was defined as BGL >8.3 mmol/L.16 If more than one episode of hypoglycaemia or hyperglycaemia was detected within the same hour it was considered as one episode with the lower level recorded. BGLs were analysed using a point of care blood gas analyser at each NICU (ABL800 Flex; Radiometer, Copenhagen, Denmark). Glucose levels at the referring hospitals and during transfer were measured using a variety of methods, including reagent strips or iSTAT (Abbott Point of Care, Princeton, New Jersey, USA) and these were included in this analysis.
Neurodevelopmental measures recorded at 24 months include Bayley Scale of Infant and Toddler Development III (BSID-III) subscales (cognitive, language, motor and socioemotional), blindness, sensorineural deafness and cerebral palsy using the Gross Motor Function Classification System (GMFCS). Severe disability was defined as one or more of the following:
A cognitive or language subscale score <70 (standardised score of 100±15, mean±SD) on BSID-III. Infants who were unable to complete an assessment due to their disabilities were given a score of 40 (4 SDs from the mean) for all subscales.18 19
Blindness: defined as 6/60 vision in the better eye.
Sensorineural deafness: defined as the need to use bilateral hearing aids.
Cerebral palsy: GMFCS ≥3.
Statistical analysis was done using IBM SPSS statistical software for Macintosh;V.21.0 (IBM, 2012; IBM, Armonk, New York, USA). Summary statistics are presented as median and IQR for skewed data and mean and SD for normally distributed continuous data. Frequency distributions and percentages were used to describe categorical data.
Infants were divided into two groups: no hypoglycaemia (all BGLs were ≥2.6 mmol/L) and hypoglycaemic group (at least one BGL <2.6 mmol/L). The hypoglycaemic group was further divided into those with one episode, two episodes and three or more episodes of hypoglycaemia (recurrent). For univariate analysis, continuous normally distributed outcomes were compared using two-sided Student’s t-test and Mann-Whitney U was performed for non-normally distributed continuous outcomes. Categorical outcomes were compared using Fisher’s exact test. Logistic regression models were used to analyse the relationship between neurodevelopmental outcomes and hypoglycaemia as defined at two different levels (2.6 and 3.0 mmol/L) and time periods (hypoglycaemic episodes in the first 12 hours of life and first 72 hours of life). Effect size estimates were derived after adjusting for HIE stage, time of commencement of TH and any episode of hyperglycaemia. Statistical significance was defined as a p value of less than 0.05.
Hospital ethics and governance committee approval was obtained for this study. Parent consent was deemed not necessary given the retrospective nature of the study.
Results
A total of 122 infants were included in this analysis of which 18 (14.7%) died in the first 2 years of life (all had HIE Sarnat stage 3). Eight died during the first 72 hours of life, eight between 72 hours and 28 days and the remaining two at 17 and 22 months of age. Of the 104 survivors, follow-up data were available for 87 (84%) infants. Severe disability was seen in 15/87 (17%) infants. Nine had cerebral palsy, four were deaf, one was blind and 11 had a BSID-III cognitive or language score <70). None of the infants reclassified to Sarnat grade 1 died or had severe disability.
Glucose homoeostasis
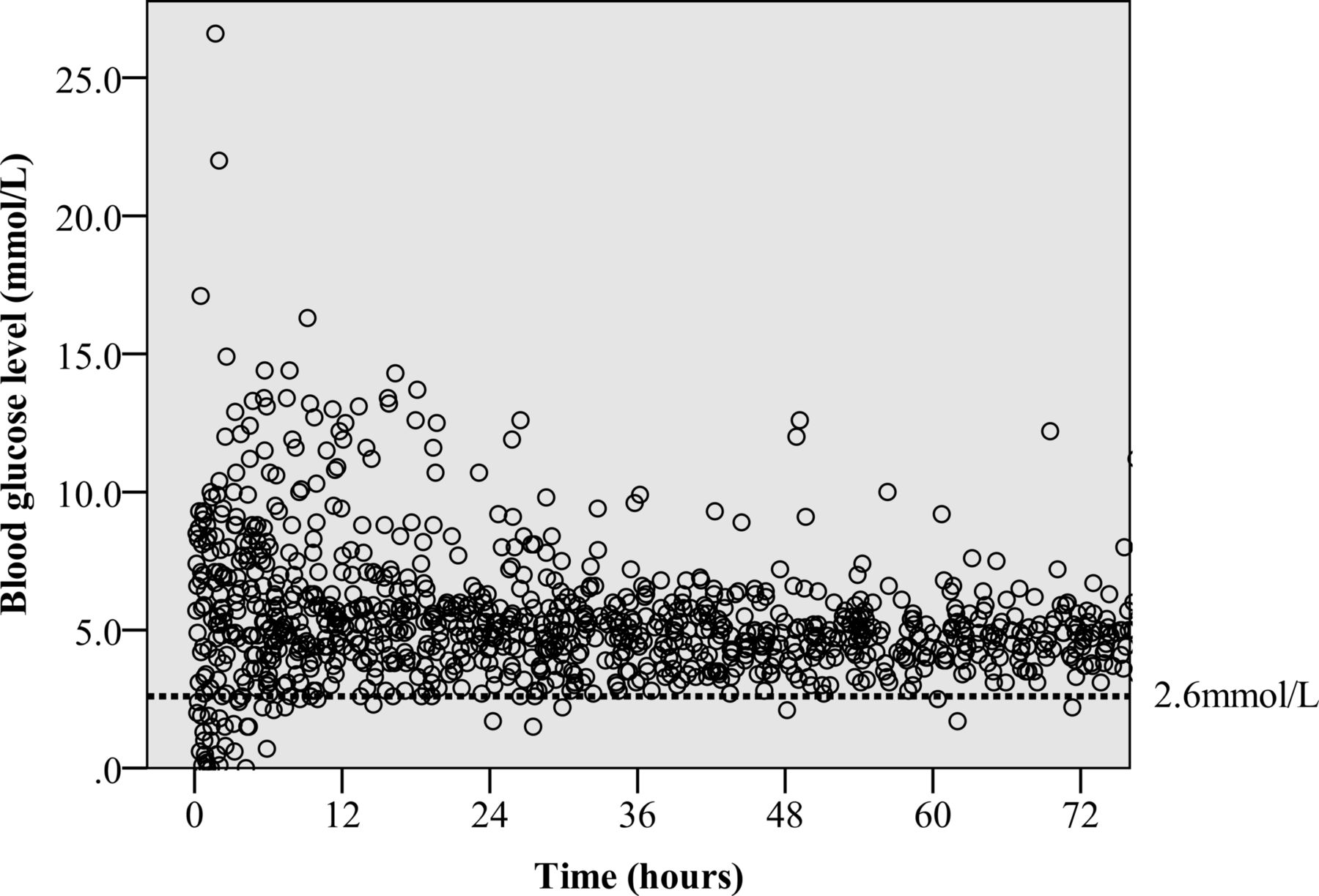
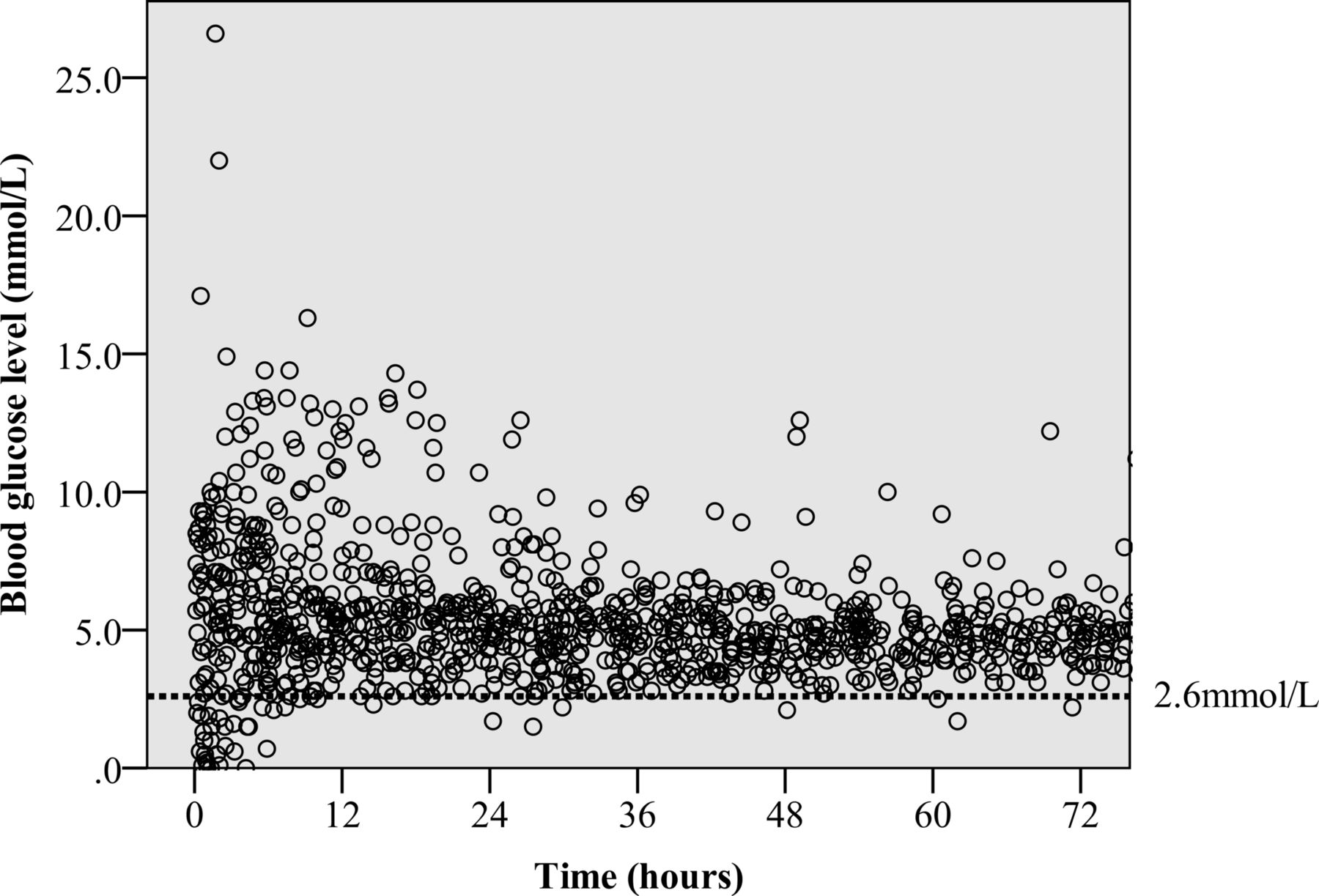
A total of 1616 BGL measurements were recorded from 122 infants from birth to the end of TH or death when this occurred within 72 hours of birth. Half of the samples were measured in the first 24 hours of life. Of the 122 infants, 38 (31%) had at least one episode of hypoglycaemia (BGL <2.6 mmol/L); 22 (18%) had two episodes and 11 (9%) had three or more episodes of hypoglycaemia. Glucose homoeostasis of the infants appeared to improve over the period of TH as seen on the scatterplot (figure 1). The majority (86.5%) of hypoglycaemic episodes occurred during the first 24 hours, 9.5% in the second 24 hours and 4% in the last 24 hours of TH.
{kind=link}
Variation of blood glucose levels over time.
Table 1 compares the basic demographic data of the no hypoglycaemia group and hypoglycaemic group. The only significant difference was that the hypoglycaemic group had a higher cord blood lactate level.
Comparison of no hypoglycaemia versus hypoglycaemic infants
Relationship between hypoglycaemia and neurodevelopmental outcomes
The BSID-III and adverse neurodevelopmental outcomes at 24 months of life are shown in table 2, which compares infants with no episodes of hypoglycaemia (baseline) to infants who have varying frequency of hypoglycaemia. The cognitive, language and motor mean BSID-III subscale scores were significantly lower in the group with three or more episodes of hypoglycaemia than the no hypoglycaemia group. Deafness, any severe disability and composite of death and/or severe disability were significantly more common in the group with three or more episodes of hypoglycaemia compared with the no hypoglycaemia group. Mortality rate was similar between all the hypoglycaemic groups and the no hypoglycaemia group.
Neurodevelopmental outcomes at 24 months
On univariate analysis, hyperglycaemia was significantly associated with severe disability and the composite of death and/or severe disability; however, this association was lost on multivariable analysis.
After adjusting for HIE stage, hyperglycaemia and time of starting TH, infants with three or more episodes of hypoglycaemia (BGL <2.6 mmol/L) had significantly higher odds of severe disability alone (table 3) or the composite of death and/or severe disability than infants with nil episodes (table 4). Hypoglycaemia within the first 12 hours of life worsens the odds for severe disability and the composite of death and/or severe disability.
Association between hypoglycaemia and disability at different blood glucose level thresholds (multivariable analysis)
Association between hypoglycaemia and death and/or disability at different blood glucose level thresholds (multivariable analysis)
When using a BGL threshold of 3.0 mmol/L, hypoglycaemia in the first 72 hours of life was not associated with severe disability alone (table 3) or the composite of death and/or severe disability (table 4). However, infants with three or more episodes of hypoglycaemia in the first 12 hours of life had significantly higher odds of severe disability alone and the composite of death and/or severe disability than infants with nil episodes. This association was still significant in this subset after adjusting for hyperglycaemia and time of starting TH.
Discussion
This study highlights the fact that glucose homoeostasis is poor in the first 72 hours of life for infants suffering from HIE, which predisposes them to episodes of hypoglycaemia. The results also suggest that recurrent episodes of hypoglycaemia (BGL <2.6 mmol/L) are associated with worse neurodevelopmental outcomes.
There is no universal agreement on the definition of neonatal hypoglycaemia in otherwise healthy neonates, although maintaining levels above 2.5 mmol/L, especially after the first 24 hours of life, is recommended.10 A large proportion of our study group (31%) had at least one episode of hypoglycaemia (BGL <2.6 mmol/L) with almost 10% having three or more episodes of hypoglycaemia. The prevalence of any episode of hypoglycaemia in our cohort was similar to studies that involved TH in newborns, with rates ranging from 12% to 28%.16 20 Similar to other studies, the glucose homoeostasis improved over the first 72 hours of life with the majority of BGLs falling between 3 and 8.3 mmol/L after the first 48 hours of life.15 16
We found that recurrent hypoglycaemia, particularly in the first 12 hours of life, was associated with adverse neurodevelopmental outcomes after adjusting for HIE stage, time of commencement of TH and any episode of hyperglycaemia. Three studies have reported on the association of early hypoglycaemia with long-term neurodevelopmental outcomes in infants with HIE,14–16 Nadeem et al 15 found that early hypoglycaemia was associated with worse neurodevelopmental outcome at 24 months of age in infants with HIE, however, when adjusted for HIE stage this was no longer significant; the difference between this and our study may be due to the larger number of infants in our study, 52 vs 122. Two studies, Basu et al and Tam et al, had infants who received TH, making up 50% and 12% of their cohort, respectively.14 16 Tam et al 14 found that hypoglycaemia was a risk factor for future corticospinal tract injury and there was a 15-point lower cognitive and language score on the BSID-III scale. Basu et al 16 found that infants from the CoolCap trial that had hypoglycaemia were at significantly higher risk of an unfavourable neurodevelopmental outcome. These associations remained significant after adjusting for birth weight, Apgar score, pH, Sarnat stage and hypothermia group.
An interesting finding of our study was that even when we used a cut-off of 3.0 mmol/L for the definition of hypoglycaemia, the association between recurrent hypoglycaemia in the first 12 hours of life and death and/or severe disability among survivors persisted. These findings may be due to the small numbers. There are no comparative studies conducted that support this finding. Hence, we can only hypothesise that targeting a threshold of 3.0 mmol/L in the first 12 hours of life instead of the traditional 2.6 mmol/L may result in additional benefits for these vulnerable infants. This requires further investigation.
The limitations of this study are its retrospective cohort design, small sample size and the heterogeneous population group (inborn vs outborn) and absence of data on Apgar scores at 10 min in many of the infants. Despite having a heterogeneous population the clinical characteristics of inborn and out-born groups were similar with regards to demographic data, stage of HIE, biochemical and clinical markers of severity and rates of hypoglycaemia. Although there was a 20% rate of loss to follow-up at 2 years, the study and lost to follow-up group were similar with regards to demographic data, stage of HIE, biochemical and clinical markers of severity and rates of hypoglycaemia. Another limitation was that the cut-off values that we chose to define hypoglycaemia for analysis were arbitrary.
Our study confirms that hypoglycaemia frequently complicates the care of infants born with HIE and that recurrent hypoglycaemia (BGL <2.6 mmol/L) in this setting is associated with significantly higher risk of death or severe disability. Larger prospective studies are required to establish the optimal BGLs in infants undergoing TH for HIE. Early anticipation and prompt management to prevent early, recurrent hypoglycaemia is essential to improve neurodevelopmental outcomes in infants with HIE receiving TH.
References
Footnotes
Contributors JKGT designed the study and data collection instruments, collected the data, carried out the initial analyses, drafted the initial manuscript, reviewed and approved the final manuscript as submitted. CM assisted in design of the study, reviewed and revised the manuscript and approved the final manuscript as submitted. JM assisted in design of the study, reviewed and revised the manuscript and approved the final manuscript as submitted. SR conceptualised the study and assisted in design of the study, reviewed and revised the manuscript and approved the final manuscript as submitted. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Competing interests None declared.
Ethics approval Princess Margaret Hospital Human Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.