Article Text

Abstract
Objectives Most children admitted to the emergency department (ED) require peripheral venous access (PVA), which is often difficult to perform or is unsuccessful. Ultrasound guidance helps with the placement of peripheral short cannulas (SC), but it has a limited cannula duration and a high risk of developing complications. The aim of this study was to compare success rates, dwell times and complications of peripheral venous long cannulas (LCs) inserted under ultrasound guidance with those of SCs in children.
Methods We prospectively studied all children older than 10 years of age admitted to our paediatric ED requiring PVA for an expected therapy of more than 5 days. In children with difficult intravenous access (DIVA), after two unsuccessful attempts of ‘blind’ placement of SCs, LCs (20 G, 8 cm) were inserted in the deep veins of arms using ultrasound guidance and the direct Seldinger technique.
Results LC placement (n=20) was successful in 100% of the cases. LC dwell time was 9.2±6.0 days, and most catheters were electively removed because they were no longer indicated. SC (n=20) placement showed a shorter dwell time duration, 3.2±2.1 days (p<0.0001), with complications occurring in 70% of the cases compared with 25% of cases in patients with LC (p=0.002). No local or major infectious complications were reported with LC placement.
Conclusions Ultrasound-guided placement of LC was associated with a low risk of catheter failure and complications compared with the ‘blind’ placement of SC. LC placement may be considered a valid option in patients with DIVA requiring PVA in paediatric ED or in children who are candidates for infusion therapy expected to last longer than 5 days.
- general paediatrics
- paediatric practice
- procedures
- resuscitation
- vascular disease
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What is already known on this topic?
Ultrasound-guided placement of polyurethane long (8 – 10 cm) cannulas (LCs) by the Seldinger technique has been recently introduced in clinical practice.
In adults with difficult venous access, ultrasound-guided placement of LC is preferable to ultrasound-guided placement of short cannulas (SCs) in terms of complications and duration.
LCs have been used as alternatives to peripherally inserted central catheters for prolonged intravenous antibiotic therapy in children with cystic fibrosis.
What this study hopes to add?
LC was superior to SC in children who required >5 days intravenous therapy.
Children with difficult venous access in the ED may benefit from LC insertion.
Introduction
Most children admitted to our emergency department (ED) require peripheral intravenous access. The most frequent indications for intravenous treatment are need for rehydration during gastroenteritis and forced fasting, infusion of intravenous drugs and administration of a contrast medium to perform radiological exams.1
Peripheral short cannulas (SCs, length <6 cm) are traditionally the first choice device for achieving peripheral venous access (PVA). However, for compliance of the patient and anatomical reasons, SC placement may be troublesome in children; the success rate of the first attempt is estimated to be lower than 35%.2 This makes the procedure a traumatic event for both the child and the parents.3 Furthermore, difficult intravenous access (DIVA) delays treatment and increases healthcare costs in terms of material and the work duration of clinicians.4 Occasionally, the difficulty of PVA leads to less cost-effective and more invasive options, such as intraosseous infusion or placement of midline catheters or central venous access devices,5 further increasing costs and the risk of complications.
Recently, ultrasound guidance has been increasingly used to achieve PVA as well as central venous access in emergency settings and in paediatric patients, decreasing the unsuccessful attempts of both types of peripheral intravenous cannulation.2 6
Although ultrasound-guided placement of SC (2–5 cm) is successful in 100% of cases, it has a limited dwelling time and a high risk of dislocation, probably because ultrasound guidance selects for deep veins, and the tract of the cannula placed inside the vein is substantially shorter.7 8
At the same time, SCs placed without ultrasound (blind technique) guidance have a high incidence of complications, such as occlusion, dislocation, infiltration and local infection. It is estimated that a third of pre-existing SCs were dysfunctional in children presenting for anaesthesia and surgery, requiring the placement of new SCs often resulting in stress and trauma for the child.9
The risk of infiltration secondary to dislocation increases with SC dwell time: it is estimated to be 1.5% after 24 hours of catheter and 17.3% after 96 hours. Moreover, inappropriate asepsis during insertion or during maintenance may lead to local infection causing serious and permanent disabling outcomes.10 11
The guidelines of the US Centres for Disease Control and Prevention suggest that in paediatric patients, the catheter can remain in place for the entire duration of the intravenous therapy unless complications arise.12 13
Various studies in adults have shown that ultrasound-guided insertion of peripheral longer cannulas (LCs) (6–12 cm) may have a better performance compared with that of traditional SCs.14 15 These devices have also been called ‘mini-midlines’ since they are longer than traditional SCs (<6 cm), but shorter than midline catheters (15–30 cm).
In the adult ED of our hospital, a retrospective study showed that, in acute adult patients with DIVA, ultrasound-guided placement of 8–10 cm polyurethane LCs offered a fast, safe and long-lasting PVA.16
In this setting, LCs were found to couple the advantage of a fast and successful insertion (due to the ultrasound guidance and the Seldinger technique) with a prolonged dwelling time (due to the polyurethane material and a length >6 cm). At the same time, LCs are less expensive and can be more rapidly placed than traditional midline catheters, which are typically inserted by a modified Seldinger technique. LCs are also less expensive and less invasive than central venous catheters or intraosseous devices.
The aim of this preliminary prospective study was to compare the clinical performance of LCs with that of SCs in children admitted to the ED who need PVA.
Methods
The study was conducted at the paediatric ED of Fondazione Policlinico Universitario A. Gemelli-Università Cattolica S. Cuore in Rome during a limited period of 4 months (December 2016 to March 2017).
We prospectively evaluated paediatric patients older than 10 years of age who consecutively presented to the ED during the study period and were in need of a peripheral line because they were candidates for intravenous therapy expected to last more than 5 days.
Children with DIVA (scarcity or absence of visible or palpable veins of the arms), after two unsuccessful attempts of SC placement, were considered eligible for LC (study group); the placement occurred in the deep veins of the arms using ultrasound guidance and the direct Seldinger technique. All procedures were performed by specifically trained operators (nurses, attending physicians or resident physicians). We used polyurethane or polyethylene 20 G catheters that were 8 cm long (external diameter 3 Fr).
Children that had a successful SC insertion at the first or second attempt were considered as the control group.
After admission and primary exams in the paediatric ED, all children in both groups were sent to the ward.
The present study reports the first 20 patients in each group.
Technique of LC placement
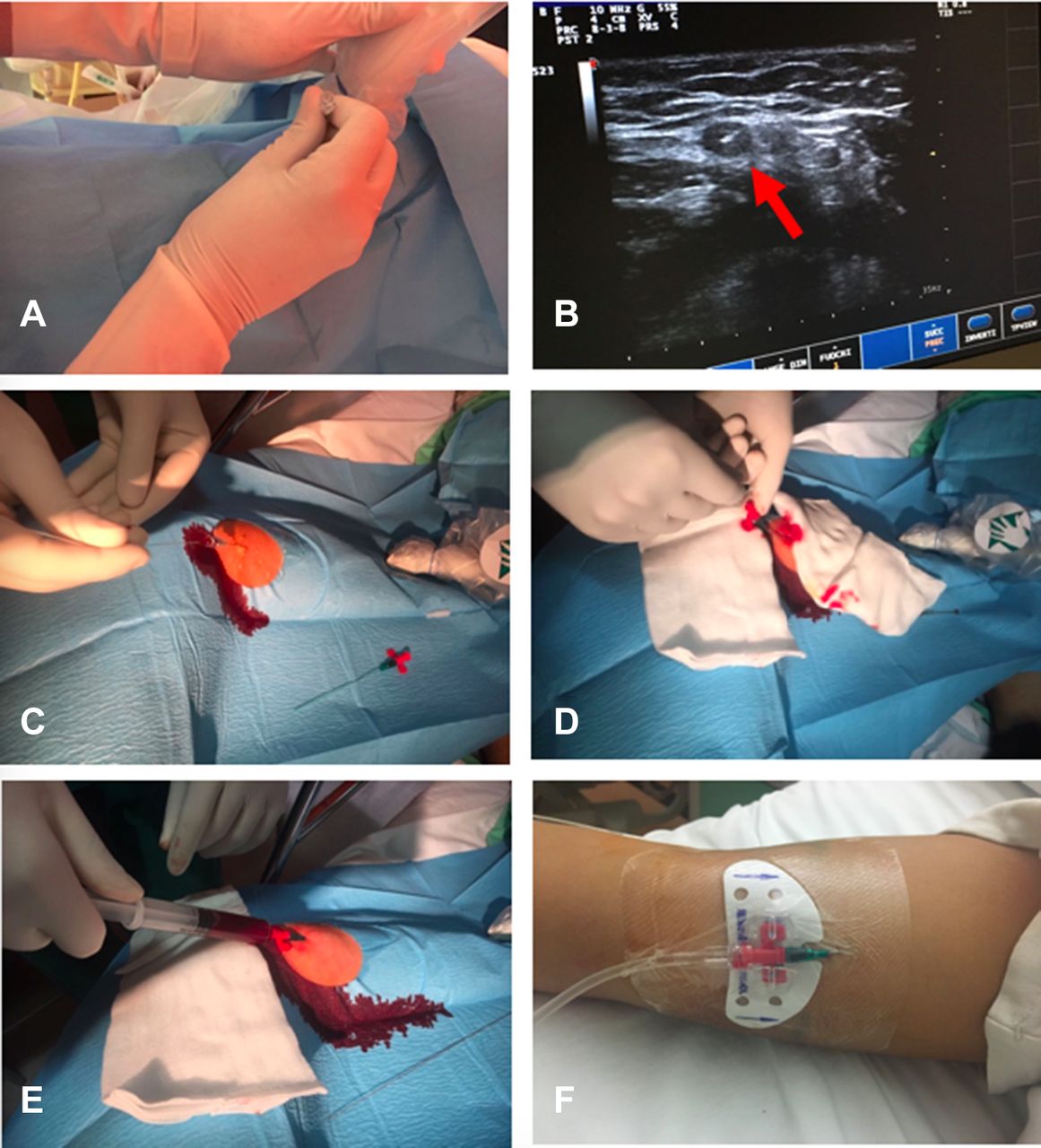
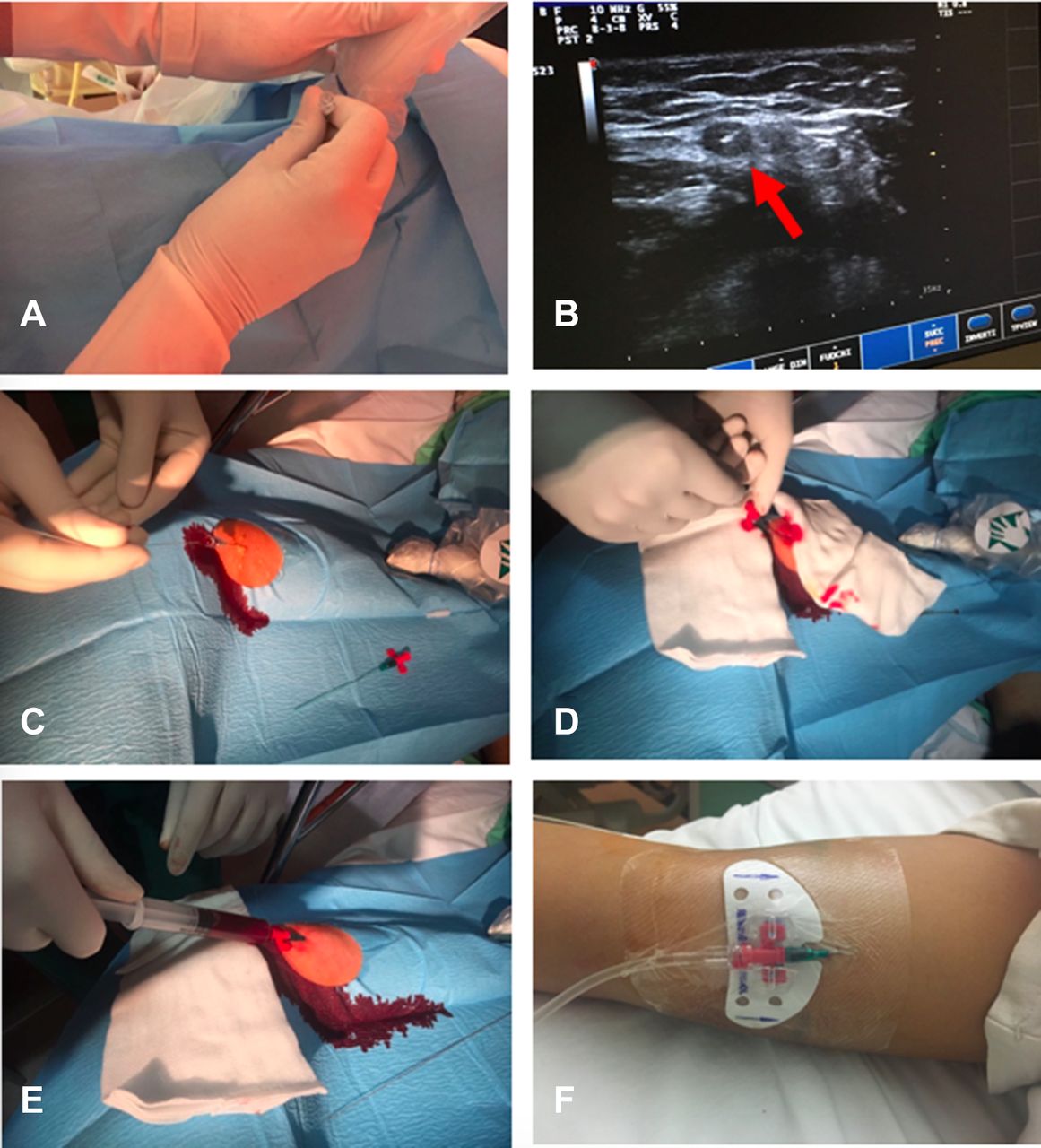
A portable ultrasound device was used (linear probe, 10–14 MHz). Before LC placement, both arms were examined by ultrasound to locate the most appropriate vein, usually in the upper mid-arm (typically basilic or brachial veins). The vein was chosen based on anatomical criteria (venous diameter and depth). The puncture site was scrubbed with 2% chlorhexidine in alcohol and was protected by a sterile fenestrated drape. The probe was covered with sterile wrap, and sterile gel was used. The operator wore sterile gloves. When required, ultrasound-guided local anaesthesia (2 mL of 1% ropivacaine) was injected before venipuncture. Venipuncture was consistently performed with real time ultrasound guidance—visualising the vein in the short-axis and directing the needle with an out-of-plane technique. After the venipuncture, according to the direct Seldinger technique, a small 0.018’ non-J guide wire was introduced into the needle. After removing the needle, the cannula was advanced into the vein, the guide wire was removed and the cannula was connected to an extension closed with a needle-free connector. The whole system was then flushed with saline solution. The cannula was finally secured with a sutureless device; the exit site was sealed with cyanoacrylate glue and covered with a transparent semipermeable dressing that provided a waterproof, sterile barrier to external contaminants (figure 1). The time to cannulation was computed from the moment of skin preparation to the final catheter securement.
{kind=link}
The cannulation procedure. (A) Puncture of the vein with the needle under direct ultrasound guidance (out-of-plane approach); (B) Ultrasound visualisation of the vein in short axis, with the needle inside the vein (arrow); (C) Introduction of the guide wire through the needle; (D) Introduction of the catheter over the guide wire; (E) Confirmation of the successful cannulation by aspiration of blood; (F) Stabilisation of the catheter with a sutureless device and a transparent semipermeable dressing.
Technique of SC placement
We used 20 G or 22 G short Teflon cannulas. For SC cannulation, according to our hospital policies, the skin was prepared with 0.5% chlorhexidine, and the operators used non-sterile gloves. The device was not secured but was covered with gauze dressing or transparent dressing.
When children were admitted to the ward, a checklist of recommendations for proper catheter management was handed to the ward nurses. Both LC and SC were used continuously, infusing exclusively solutions appropriate for PVA according to our hospital policies (ie, no parenteral nutrition, no vesicant drugs and no solutions potentially irritating to the endothelium). The exit site was examined by the nurses three times a day. The dressing was changed every week. Reasons for removal included end of use, infection, accidental dislocation, signs of infiltration, phlebitis or occlusion. At the time of LC removal, an ultrasound scan was performed to rule out venous thrombosis.
Collected data included patient characteristics (age, gender, diagnosis at admission, infusion therapies, etc) and venous access information (insertion-related complications, success of insertion, number of attempts before insertion, insertion site, type of vessel, duration of the access and late complications).
All data were analysed by standard descriptive statistics. The results in the two groups were evaluated using the unpaired Student’s t-test. A two-tailed level of significance of p<0.05 was considered significant for all comparisons.
The parents provided written informed consent.
Results
Data collected from patients with LC placement (study group) were compared with data from the patients with SC placement (control group). Characteristics of the two groups are shown in table 1. In this pilot study, we analysed the following two groups of patients: 20 children with LC and 20 children with SC.
Patient characteristics for both groups
The majority of children in the SC group had non-surgical emergencies (osteoarthritis, pneumonia, sepsis, etc), while the majority of children in the LC group had surgical conditions (trauma, fractures, appendicitis, etc).
All catheters were used for the administration of intravenous drugs (in 35 patients), rehydration of fluids (12 patients), replacement of fluids during fasting (34 patients) and rapid injection of contrast medium during radiological exams (9 patients).
The number of attempts before successful placement, as reported in table 2, were significantly higher in the SC group compared with the 100% success rate at first attempt in the LC group. In contrast, the mean duration of each SC was drastically lower, with many cannulas repositioned during treatment. However, there was no difference in duration of the total intravenous therapy between the two groups.
Peripheral vein cannulation and complications data, by group
Seventy per cent of patients in the SC group reported episodes of dislocation/infiltration, occlusion and thrombosis compared with 25% of children in the LC group. In 15 patients (75%), LCs were electively removed at the end of therapy. In one patient, LCs were replaced by a central venous access device after 7 days (need of chemotherapy). In two young agitated patients, accidental dislocation occurred. In two cases, the catheter was removed because of venous thrombosis (after 25 days and 8 days, respectively); both patients were receiving infusion of vancomycin. No clinical embolic events were recorded in these two patients with thrombosis of the catheters. No local or major infective complications were reported in patients with LC; however, 35% of children with SC developed local infections.
With respect to the vein considered eligible for LC positioning, eight LCs (40%) were placed in the basilic vein, three (15%) in the brachial vein and nine (45%) in the cephalic vein. Using preformed kits for LC insertion, the total procedural time was 7.4±1.4 min.
Discussion
Our study suggests that the use of ultrasound-guided LCs in a paediatric ED may have many advantages over the use of traditional SCs inserted with or without ultrasound guidance.
While ultrasound guidance has been recommended in paediatric patients for the placement of DIVA, SCs placed under ultrasound guidance have a shorter duration than those inserted using the traditional blind technique.17 This is probably due to the higher risk of dislocation; when a short cannula is inserted by ultrasound guidance in a deep vein, the tract of the cannula placed inside the vein is obviously shorter. In contrast, the LCs we used were 8 cm long and even if placed in veins located at a depth of 1 cm, the long tract of the cannula remained inside the vein. In our study, the mean time for LC insertion was 15±2.34 min, which is comparable with the results of Elia et al,15 who reported a time required for positioning the LC of 16.8 min in adult patients. Even if LC insertion required a technique slightly more complex than that of SC, when using a preformed kit that contains the LC and all the accessories required for the procedure, such as in our study, the insertion time was 7.4±1.38 min. This time is not much longer than the time needed for SC placement in our ED routine.
In addition, the rate of late complications was significantly lower in the LC group than that in the SC group. The heterogeneous group of complications that may lead to ‘catheter failure’ includes non-infective complications (dislocation, lumen occlusion, infiltration, chemical thrombophlebitis, mechanical thrombosis, etc) and infective complications (bacterial phlebitis, catheter-related bloodstream infection, etc). The frequency of children in the SC group with catheter failure due to non-infective complications was very high (70%), which is similar to data reported in the literature. There are not enough recent studies in children to make a comparison; however, a recent analysis estimated that a third of pre-existing PVA devices were dysfunctional in children presenting for anaesthesia and surgery.8 Dislocation was rare with LC because of the particular length of the device (8 cm) and because of its securement (glue, sutureless device and transparent dressing). Occlusion and thrombosis might have been at least partially prevented by the material of our LCs, since our SCs were made of Teflon, which is known to be more thrombogenic than polyurethane.18 Two cases of symptomatic vessel thrombosis (10%) were found after an LC dwell time of 16.5 days. This was not worse than rates reported in other studies in adults where the incidence varied from 20.9% to 2.8%.15 19 Interestingly, these two cases of thrombosis occurred in LCs used for vancomycin, an irritating drug, preferably infused by the central route. In both cases, venous thrombosis was probably due to a chemical phlebitis induced by vancomycin.
We found no bloodstream infections, only local infections, exclusively in the SC group (35% of patients). This is not surprising considering that LCs were inserted with an appropriate aseptic technique that was not adopted in SC placement. Of course, a low risk of infection is also strongly related to an appropriate policy of maintenance. Nursing care is very important to ensure the safety of the placement and the management of peripheral intravenous catheters in children.10
This lower risk of catheter failure was associated with extended duration of the line. LCs were maintained for 9.2±6 days, and the catheters were left in place without any time limit as long as needed or until complications occurred. This was done to reduce costs and patient discomfort related to multiple punctures.12 To the best of our knowledge, only two other studies in adults analysed LC without establishing a maximum dwell time, reporting an average lifetime of 6.2±5.1 days and 14.5±10.6 days.15 19 Sarah et al reported 20 cases of paediatric patients affected by cystic fibrosis using Vygon Leaderflex 22G×8 cm catheters for intravenous antibiotic therapy. The mean duration of the catheters was similar to our experience (mean 9.5 days±5.0 SD), but the reported rates of local complications were high without serious adverse outcomes.20
The success of insertion at first attempt, the long dwelling time and the low risk of catheter failure or infection may contribute to increasing the overall cost-effectiveness of LC.
Our study has several limitations: (1) The study was prospective and controlled but non-randomised due to the necessity to adhere to the criteria of good clinical practice; (2) the population we studied was small and limited to children >10 years old; and (3) following our hospital policies, the protocols of insertion and maintenance of LC were quite different from the protocols of SC, and this result probably had an impact on the infection and dislocation risk.
Further larger studies are needed to better analyse the risks and benefits of LC in the emergency room to evaluate both the cost-effectiveness and the paediatric population most likely to benefit from this strategy.
Conclusions
In this preliminary clinical study in children admitted to an ED, ultrasound-guided placement of peripheral LC appeared to be preferable to SC placement in terms of fast and successful insertion, low risk of catheter failure and long duration of the line. These results improve children and parent satisfaction with fewer skin punctures and fewer complications and reduce nursing workload.
The paediatric population that might benefit from this device is acutely ill children with DIVA requiring fast and reliable peripheral access and children who are candidates for infusion therapy, compatible with the peripheral route, for more than 5 days.
References
Footnotes
Contributors AP, AC, KWS, MP and GV have made substantial contributions to the conception and design of the study protocol and have given final approval of the version to be published. AP was responsible for the statistical analysis, sample size calculation, randomisation process and final approval of the version to be published. AP and KWS carried out the recording of all the studied items of the randomised patients and have given final approval of the version to be published. AP, MP and GV wrote the manuscript with inputs from all authors.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Parental/guardian consent obtained.
Ethics approval Ethics Committee of Catholic University of Sacred Heart, Rome, Italy.
Provenance and peer review Not commissioned; externally peer reviewed.