Article Text

Abstract
Objective Multiple outcomes can be measured in infants that receive neonatal care. It is unknown whether outcomes of importance to parents and patients differ from those of health professionals. Our objective was to systematically map neonatal care outcomes discussed in qualitative research by patients, parents and healthcare professionals and test whether the frequency with which outcomes are discussed differs between groups.
Design Systematic review of qualitative literature. The following databases were searched: Medline, CINAHL, EMBASE, PsycINFO and ASSIA from 1997 to 2017. Publications describing qualitative data relating to neonatal care outcomes, reported by former patients, parents or healthcare professionals, were included. Narrative text was analysed and outcomes grouped thematically by organ system. Permutation testing was applied to assess an association between the outcomes identified and stakeholder group.
Results Sixty-two papers containing the views of over 4100 stakeholders were identified; 146 discrete outcomes were discussed; 58 outcomes related to organ systems and 88 to other more global domains. Permutation testing provides evidence that parents, former patients and health professionals reported outcomes with different frequencies (p=0.037).
Conclusions Parents, patients and health professionals focus on different outcomes when discussing their experience of neonatal care. A wide range of neonatal care outcomes are reported in qualitative research; many are global outcomes relating to the overall status of the infant. The views of former patients and parents should be taken into consideration when designing research; the development of a core outcomes set for neonatal research will facilitate this.
- neonatology
- outcomes research
- patient perspective
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Multiple outcomes can be measured in infants that receive neonatal care.
It is not known which outcomes are considered important by former neonatal patients, parents and healthcare professionals, or whether these differ between groups.
What this study hopes to add?
The predominant outcomes identified by parents, former patients and health professionals related to holistic concepts (such as ‘normality’).
Significant differences were identified in outcomes discussed by parents, patients and health professionals.
Differences in neonatal outcomes prioritised by parents, patients and health professionals should be recognised when planning research.
Introduction
In high-resource settings approximately 1 in 10 babies will require care in a neonatal unit.1 Conditions such as preterm birth affect patients’ long-term outcomes: consequences include cardiovascular disease in adulthood,2 neurosensory impairment,3 respiratory disease4 and lower rates of employment and marriage.5 Infants born more prematurely tend to have worse outcomes.6 As neonatal survival for babies of all gestational ages improves long-term outcomes become more important.
An outcome is the measured effect that illness or treatment has on an individual.7 Parents and patients are rarely involved in outcome selection in paediatric research.8 Poor outcome selection causes research waste9: research produced is not relevant to patients’ lives. Neonatal care, and the underpinning research, should focus on outcomes important to those it affects most: former neonatal patients, parents and healthcare professionals.9 10 Identifying these outcomes is crucial to ensure research is relevant and efficient.9 11 Qualitative research provides a rich description of complex phenomena such as neonatal care.12 One commonly used approach to identify outcomes of importance to stakeholders is primary qualitative research. Considerable qualitative research exploring how parents and health professionals perceive neonatal care has been conducted previously13 14; therefore, by systematically reviewing published qualitative research it is possible to map the outcomes discussed by different groups. This review does not include all research on how stakeholders perceive neonatal care: it is focused on how former patients, parents and health professionals perceive the outcomes of this care.
In this study we aimed to map the range of outcomes identified in qualitative literature by different stakeholder groups: parents, ex-neonatal patients and healthcare professionals. We also wanted to test the hypotheses that stakeholder groups prioritise outcomes differently, and that outcomes identified differ by infant gestational age category.
This work is a component of a wider programme to compile a core outcomes set for neonatology.15 A core outcomes set is an agreed collection of important outcomes identified through robust consensus methods by all key stakeholder groups.7 The results of this study will be combined with the results of a systematic review of outcomes reported in clinical trials.16 These will be used as the starting point for the consensus process to determine a core outcomes set.15
Methods
We registered this systematic review prospectively on PROSPERO (prospective register of systematic reviews): CRD42016037874.17 We conducted the review according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.18 We searched the following databases: Medical Literature Analysis and Retrieval System Online (MEDLINE), Cumulative Index to Nursing and Allied Health Literature (CINAHL), Excerpta Medica Database (EMBASE), Psychological Information Database (PsycINFO) and Applied Social Sciences Index and Abstracts (ASSIA). Qualitative or mixed methods studies were included if they contained outcomes identified by stakeholders in the context of babies admitted to a neonatal unit. Full inclusion and exclusion criteria are listed in online supplementary eTable 1. We considered all studies published from 1 January 1997 to 1 January 2017 in a peer review journal in all languages (where necessary a translation was obtained). The databases were last searched on 14 February 2017. The search strategy used for MEDLINE is described in online supplementary eFigure 1. The terms derived from this search strategy were translated to other databases.
Supplemental material
All identified papers were screened by title and abstract and then by full text. After double-screening a sample of papers and agreeing criteria all screening was completed by one researcher (JW). For quality assurance, a second researcher screened a random 10% sample of abstracts and titles (CG). Agreement between reviewers was assessed by Cohen’s kappa coefficient.19
After screening all papers were coded independently by two researchers (JW and CG or GB) using Eppi-Reviewer V.4 software.20 Any disagreement was resolved by a third researcher (CG or GB). Data on study design, stakeholder demographics, infant birth characteristics and verbatim text relating to neonatal care outcomes were extracted and stored. Quality assessment of individual studies was not undertaken as it is a controversial area of uncertain value in relation to qualitative research.21
All outcomes were grouped according to a previously defined framework of organ systems22 using the following domains: cardiovascular, respiratory, gastrointestinal, neurological, genitourinary, infection, skin and development. All three reviewers jointly refined this framework using methods incorporating thematic analysis.23–25 Where narrative data did not fit clearly into the domains, dialogue between all reviewers was used to develop new domains. Outcome domains were thematically analysed to develop higher order categories. A new hierarchy was developed to group outcomes because established hierarchies either did not relate well to neonatal care26–28 or missed key concepts.7 This outcome hierarchy is described in box 1.
An example of an outcome hierarchy
Text extracts to identify or infer a result of clinical care, the ‘outcome’ such as ‘Bonding with parents’.
Similar ‘outcomes’ were grouped into thematically linked ‘domains’ such as ‘Relationships with others’.
‘Outcome domains’ relating to similar concepts were grouped into ‘categories’ such as ‘Social’.
We did not address the ways in which an outcome was measured. For example, the ‘outcome’ ‘Parental bonding’ could be measured using parent-reported scores or an external assessment.
We analysed whether outcomes identified differed by stakeholder groups and by infant gestational age category (using WHO definitions of prematurity).29 We used permutation testing30 to test for an association between the frequency that outcomes in different domains were identified and the stakeholder group involved. We performed 5000 replications to generate the distribution of the test statistic under the null hypothesis of no association, and compared our results with this distribution. We performed a similar analysis to test for an association between infant gestational age and frequency of outcome reporting. If a significant association was found we explored this further in a post hoc analysis to identify where the observed results differed most from the frequencies expected under the hypothesis of no association established by the permutation analysis.
Results
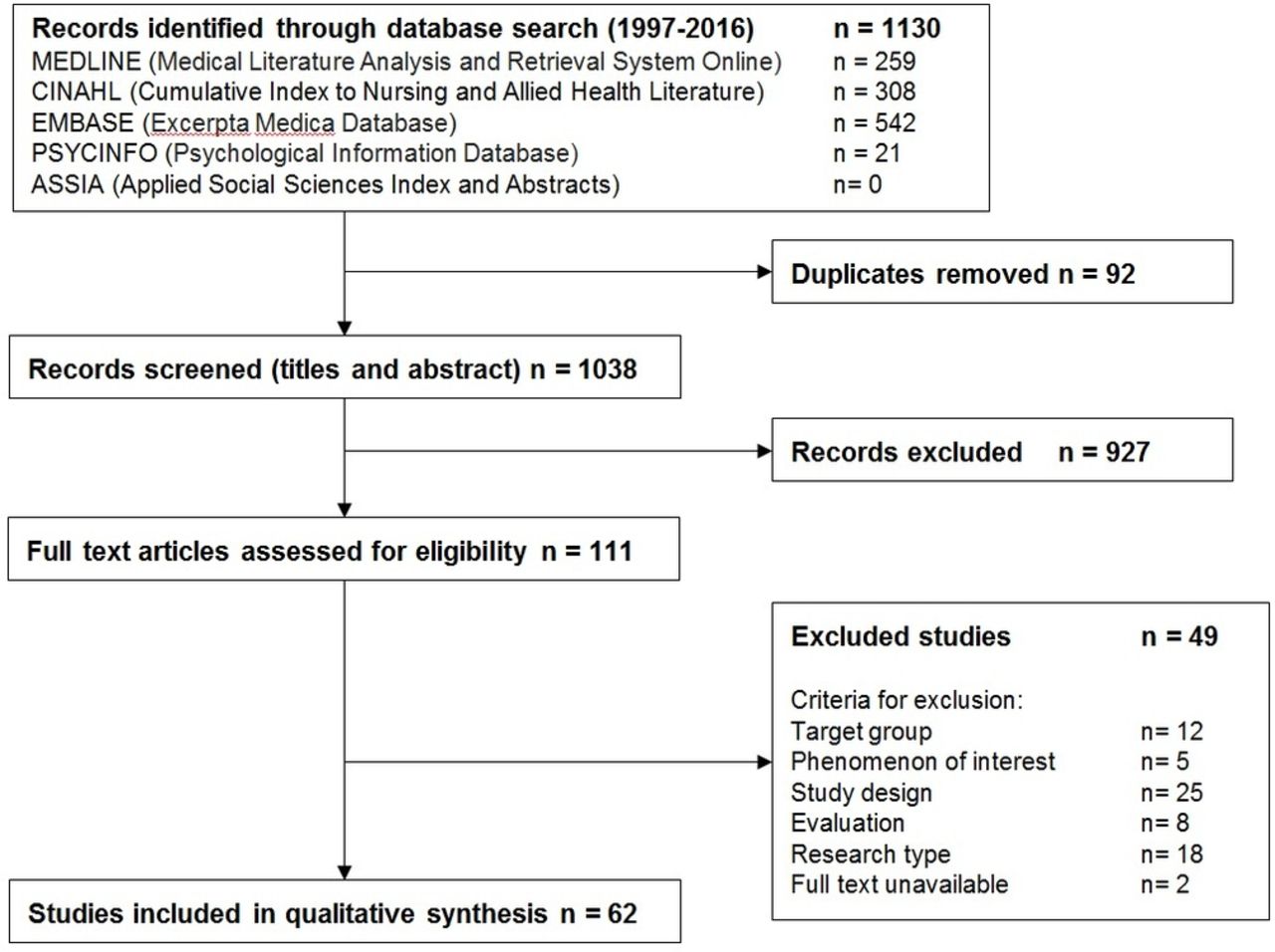
Database searches produced 1130 results which were screened and assessed for eligibility (figure 1). After applying inclusion and exclusion criteria 62 studies containing the views of 4100 stakeholders were analysed. Agreement between reviewers was high (Cohen’s kappa coefficient=0.81).19
{kind=link}
PRISMA flowchart of study selection.
The 62 included studies reported data from 15 countries; 9 related to full-term infants, 31 to preterm infants (born <37 weeks’ gestational age) and 20 to extremely preterm infants (born <28 weeks’ gestational age). A range of methodologies was used including direct observation (13 studies) and individual (25 studies) or group interviews (13 studies). Questionnaires were used in 21 studies, two of which were Delphi processes. Included studies are described in online supplementary eTable 2.
Included studies involved over 4100 participants. Parents were the most frequently involved stakeholder group (1969 parents in 40 studies; 65%); former neonatal patients were less commonly included (368 patients in 5 studies; 8%). Nurses and midwives were the professional group involved most often (1096 involved in 24 studies; 39%). Three hundred and sixteen doctors were involved in 18 studies (29%). We also identified 351 additional participants consisting of other family members, teachers, social workers and allied health professionals. In many studies, particularly those employing observation of clinical practice, the total number of research participants was not recorded.
One hundred and forty-six distinct outcomes were extracted from the included studies. Fifty-eight outcomes related to organ systems within the original framework; we were unable to categorise 88 outcomes within the original framework. The final framework is shown in table 1. An example of the thematic analysis leading to the expanded framework is shown in box 2.
Final outcome framework
Example of framework synthesis related to the outcome of ‘Normality’. Thematic analysis of verbatim extracts identified a recurring theme
‘The mother also worried that…Lisa would not have a normal life.’ 41
‘Being reassured that he was on line for how old he was…Just reassurance he was doing well.’ 42
‘Finally, a mother called it a developmental land-mark when an older sister dared show her irritation towards her little brother, ‘no longer treating him as if he were made of glass.’ 43
From this and similar text the outcome of ‘Normality’ was derived by thematic analysis. It did not fit within the existing outcome hierarchy but was reported extensively, so a new domain was added to the framework again called ‘Normality’. This outcome domain relating to the overall status of the infant was similar to outcome domains like ‘survival’, ‘vitality’ and ‘growth’, so these domains were grouped together as an outcome domain category called: ‘Holistic outcomes’.
The full inventory of outcomes is listed in online supplementary eTable 3. A table of all outcomes in each study (with verbatim text extracts) is shown in online supplementary eTable 4.
Outcomes were identified relating to all of the organ systems included in the original framework and assigned to an organ system outcome domain category (table 2). The organ system outcome domains most frequently discussed at the study level were ‘development’ (32 studies; 52%) and ‘gastrointestinal’ (24 studies, 39%). The individual organ system outcomes most frequently discussed were ‘language disorders’ (8 studies, 13%), ‘visual impairment’ (7 studies, 11%) and ‘breast feeding’ (7 studies, 11%).
Organ system outcomes
The majority of outcomes identified did not relate to individual organ systems. Some related to the overall status of the infant and were assigned to a holistic outcome domain category (table 3). Other domains related to the effects experiencing neonatal care has on parents; these were assigned to a ‘Parent focused’ outcome domain category (table 4). Another group of domains related to the neonatal care delivered; these were assigned to a ‘Healthcare delivery’ outcome domain category (table 5). A group of domains was identified relating to the cost of neonatal care; these were assigned to an ‘Economic’ outcome category (table 6). Finally, a group of outcome domains was identified relating to the relationships neonatal patients develop with others; these were assigned to a ‘Social’ outcome domain category (table 7).
Holistic outcomes
Parent-focused outcomes
Healthcare delivery outcomes
Economic outcomes
Social outcomes
From these outcome domains the most frequently discussed at study level were ‘parental support’ (30 studies, 48%) and ‘healthcare workers—communication’ (30 studies, 48%). The individual outcomes most frequently discussed were ‘normality’ (16 studies, 26%) and ‘survival’ (11 studies, 18%).
Permutation test analysis showed a statistically significant association (p=0.037) between different stakeholder groups and outcome categories identified (online supplementary eFigure 3). The frequency with which patients discussed the outcomes was most divergent from the other groups. In particular, patients discussed outcomes relating to the genitourinary, surgical, developmental and pain outcome domains more than would be expected by chance.
We found no statistically significant association (p=0.114) between gestational age and outcome categories (online supplementary eFigure 2).
Discussion
We have systematically reviewed and synthesised the outcomes reported in qualitative research by those with lived experience of neonatal care: patients, parents and healthcare professionals. We show that the patterns of outcomes discussed by former neonatal patients, parents and healthcare professionals are different. This is in keeping with previous single-centre research31 and case reports.32 This indicates that healthcare professionals should consider whether the outcomes they discuss align with patients and parents’ concerns.33 Acceptance of the differences shown should form part of the process of shared decision-making in clinical practice.34 Poor outcome selection is also a known problem in paediatric research,8 35 involving patients and parents will help reduce research waste.36 37
The outcomes identified extend beyond the organ system-specific outcomes commonly reported in clinical trials and include global concepts such as ‘normality’ of the child in later life, the impact on an infant’s family and the healthcare team, financial and time costs and how patients interact with wider society. Our findings are in keeping with observational studies illustrating the wide-reaching consequences of neonatal illness.38–40 Another feature of the outcomes identified is that rather than relating to a specific diagnosis or disease many reflect the global status of the child. Diagnoses like necrotising enterocolitis or retinopathy of prematurity were mentioned less frequently than their consequences, such as feeding difficulties or visual impairment. In general, the outcomes identified indicate that pathological processes and diagnoses are less relevant to patients and parents than the effects they have on day-to-day life. Priority should be given to identifying efficient ways of measuring more global outcomes of neonatal conditions throughout childhood and later life, for example, through robust linkage of neonatal data with education databases.
This more holistic approach should extend to how babies are categorised. Our work included an undoubtedly heterogeneous population, but this was driven by discussions with former neonatal patients and parents at the planning stages of this project. They strongly stated that ‘a sick baby is a sick baby’ regardless of birth weight or gestational age: a statement that is supported by our finding that there was no significant difference in how frequently outcomes were discussed in relation to babies of differing gestational ages. Splitting research populations by arbitrary landmarks not recognised by parents or former patients32 may be a source of research heterogeneity.
The strengths of our study included identification and synthesis of outcomes from an international and methodologically diverse range of studies, relating to babies of all gestational ages, and a wide range of stakeholders. We included outcomes that stakeholders spontaneously identified. As a result, we were able to include data from a wider range and diversity of stakeholders than a primary research study could. We followed a preregistered protocol with reporting in line with PRISMA guidelines.18 It has been argued that quality assessment is needed in ‘mapping’ reviews to aid in interpretation and uptake of findings,24 but the value of this approach is uncertain.21 The consultation phase of our core outcomes set development work will provide the opportunity to critically reflect on the contribution of these findings to our understanding of what constitutes an ‘important’ outcome in neonatal research.
A limitation of our study is that, in line with many systematic reviews, we are synthesising data from studies that did not explicitly address the research question we are asking. This meant that we combined data about which outcomes parents, patients or healthcare professionals mentioned during research. As a result, we described how frequently outcomes were discussed, rather than the importance assigned by groups to each outcome. Many outcomes were only discussed in a single study. We present them here to show the range and breadth of outcomes discussed, but cannot comment on whether they are more or less important than more frequently mentioned outcomes. Another limitation is that the researchers who undertook the primary qualitative research in the included studies will have influenced our review through their analysis; we reviewed data that was a step removed from the opinions of the stakeholders themselves. However, by following rigorous methodology and employing a comprehensive search strategy we have combined all available data to produce this mapping review.
Trying to measure all of the varied outcomes identified in this work in research would be impractical, if not impossible. This work supports the importance of identifying a core outcomes set, and highlights the importance of input from all stakeholder groups. In other fields, core outcomes sets have successfully aligned patient and healthcare professional research priorities.36
Conclusion
Parents, patients and clinicians report a wide range of neonatal care outcomes. Parents and patients focus on different outcomes than health professionals. Outcomes reported do not map to organ systems commonly addressed in clinical trials, many are global outcomes. We suggest that the views of former patients and parents should be taken into consideration by researchers and funding bodies.
Acknowledgments
The authors are grateful to Louise Wann (West Middlesex University Hospital) for her contributions running the database searches.
References
Footnotes
Contributors JW and CG conceived this systematic review. This protocol was created by JW, GB and CG. Searches were performed by LW. All search results were reviewed by JW and assessed by the eligibility criteria. Quality assurance was completed by CG. Coding and result synthesis was completed by JW, GB and CG. Statistical analysis was completed by NL. The first draft of the manuscript was written by JW, CG, GB and NL. NM edited and reviewed the manuscript. It was approved by JW, CG, GB, SA, LW, NL, NM and the COIN Steering Group.
Funding This research is sponsored by Imperial College London and supported by an MRC Clinician Scientist Fellowship award to CG (MR/N008405/1) and salary support for JW from the Portland Hospital.
Disclaimer The Imperial College London, the MRC and the Portland Hospital had no involvement in the research or this publication.
Competing interests None declared.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Requests for access to data should be addressed to the corresponding author.
Collaborators COIN Project Steering Group: Elsa Afonso; Iyad Al-Muzaffar; Ginny Brunton; James Duffy; Chris Gale; Anne Greenough; Nigel Hall; Marian Knight; Jos Latour; Neil Marlow; Neena Modi; Laura Noakes; Julie Nycyk; Mehali Patel; Angela Richard-Londt; James Webbe; Ben Wills-Eve.