Article Text

Abstract
Objective We investigated the content and quality of communication of interservice interprofessional handover between obstetric nurses and neonatal physicians for high-risk deliveries.
Design Observational study.
Setting Labour and delivery unit at a tertiary care hospital.
Method We audio-recorded handovers between obstetric and neonatal teams (n=50) and conducted clinician interviews (n=29). A handover content framework was developed and used to qualitatively code missing core and ancillary content and their potential for adverse events.
Results 26 (52%) handovers missed one or more clinical content elements; a third of the handovers missed at least one core clinical content element. Increase in the number of missed clinical content elements increased the odds of potential adverse events by 2.39 (95% CI1.18 to 5.37). Both residents and nurses perceived handovers to be of low quality and inconsistent and attributed it to the lack of a structured handover process.
Conclusion Streamlining handover processes by instituting standardisation approaches for both information organisation and communication can improve the quality of neonatal handovers.
- neonatology
- nursing
- qualitative research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is already known on this topic?
Neonatal handovers are a unique example of interprofessional interservice handovers between obstetric nurses and neonatal physicians for high-risk deliveries.
These exchanges are often ad hoc, lack structure and are prone to errors.
What this study hopes to add?
We identified missing core clinical elements, with each additional missed element increasing the potential for adverse events nearly twofold.
Opportunities for improving the neonatal handover process includes standardising the content and associated workflow process.
Introduction
Handovers (also referred to as handoffs) serve as an interactive forum for the transfer of information, responsibility and authority between clinicians.1 Handovers occur at different points in the care delivery process: at routine shift changes and at non-routine service or location changes.2 Although handovers are instrumental for care continuity, evidence suggests that they are a source for medical errors.3
Compared with shift-based handovers, challenges are exacerbated in interservice interprofessional handovers (eg, emergency nurse and medicine resident) because of the differences in clinical expertise, professional backgrounds and varying roles.4–6 One such commonly occurring handover is between obstetric (OB) nurses and the neonatal physicians for high-risk deliveries. Nearly 10% of all deliveries in the USA require an intervention from a neonatologist; 1% of newborns require extensive resuscitation support from a neonatal intensive care unit (NICU) team at delivery.7 As such, these handovers are complex and vulnerable to safety threats affecting care and management needs and demands of both the mother and the newborn.8–10
We investigated the following research questions: (A) what is the nature of clinical content exchanged during OB nurse to NICU physician handover communication?; (B) what is the core clinical content that is discussed? What is missed? What is the potential for missed clinical content for causing adverse outcomes?; and (C) what are OB nurses’ and NICU physicians’ perceptions regarding the quality and effectiveness of handover communication?
Method
Study setting and participants
This study was conducted in the Labor and Delivery (L&D) unit at the University of Illinois Hospital and Health Science Center. The L&D unit performs approximately 2700 deliveries and cares for all pregnant patients in labour including prematurity or any complex maternal or fetal medical conditions as described in the American Academy of Pediatrics Manual.11
Study participants included fellows, residents and nurses from the OB and neonatal teams. The OB team works in the L&D unit and comprises 2 attending physicians, 4 OB residents, 2 family medicine residents, 1–2 midwives, and 8–10 OB nurses. The neonatal team consists of one NICU attending physician, one neonatology fellow, one paediatric–neonatal resident (postgraduate year 2 or 3) and one paediatric intern. Four neonatology fellows, 25 paediatric residents and 4 OB nurses participated in the study over a 6-month period.
Patient involvement
There was no direct patient involvement in this study.
Neonatal handovers
Neonatal handovers involve the communication of patient-related information between the OB nursing team and the neonatal team. Neonatal handover process is initiated when an OB nurse contacts a neonatology fellow for assistance in a high-risk delivery. The fellow coordinates with the paediatric–neonatal resident(s) and meets the OB team (OB nurse, OB resident(s) and OB attending) in the L&D room. An OB nurse then provides a verbal handover to the paediatric–neonatal resident (ie, neonatal handover). This handover includes clinical content related to maternal obstetric history (age, gestational age, lab results, imaging and medications), medical history and pregnancy history (any intrapartum events, rupture of membrane, colour of amniotic fluid, chorioamnionitis, fetal tachycardia or bradycardia). These handovers often follow a narrative format, with each OB nurse following their own conversational style and structure. For example, some nurses used personalised handwritten notes, whereas others used an antepartum assessment sheet as a guide for their handover discussion.
After the handover, the antepartum assessment sheet is provided to the neonatal team. The antepartum assessment sheet, generated from the electronic health record and completed by the mother’s admitting nurse, contains information related to maternal age, gestational age, labs and other relevant information.
Postdelivery, the neonatal team performs resuscitation and stabilisation activities for the newborn, as necessary. Depending on the clinical status of the newborn, decisions regarding the transfer of the newborn to the NICU are also made. Paediatric residents with the neonatal team then create a ‘delivery note’ in the newborn’s chart with updated information regarding labs, resuscitation events, Apgar scores and the newborn’s disposition. This delivery note includes maternal information obtained at the time of delivery handover, information gathered after accessing mother’s patient record and resuscitation events performed in the delivery room.
Data collection
Data collection methods included general observations, clinician shadowing, semistructured interviews and audio recording of neonatal handover communication.
We conducted approximately 20 hours of observation taking detailed field notes to develop a general understanding of clinical workflow of the OB and neonatal teams. These sessions focused on observing the general coordination, decision-making and communication processes and tasks performed by both teams (conducted by the first author).
We shadowed the OB and neonatal teams during neonatal handovers to obtain insights on how the OB nurse requested neonatal consulting service, artefacts used for neonatal handovers (by the OB team) and team interactions. We shadowed 50 neonatal handovers, which involved 4 OB nurses and 29 neonatal team members (neonatal fellows [n=4] and paediatric residents [n=25]).
During these shadowing sessions, we audio-recorded a convenience sample of 50 (n=50) neonatal handovers between the OB and neonatal team. After each handover, we also collected the associated, deidentified antepartum assessment sheets and the resident delivery notes (n=50).
Semistructured interviews
We conducted semistructured interviews with paediatric residents (n=12) and OB nurses (n=3). Separate interview guides were used for residents and nurses (see online supplementary appendix 1). Resident interviews focused on gathering perceptions regarding the neonatal handover process, completeness and quality of maternal information provided by the OB team and potential suggestions for improving the handover process. Nurse interviews focused on the following: ease of data gathering for handover, existing tools and sources, perceptions of an effective handover, identified barriers and suggestions to improve the neonatal handover processes.
Supplementary file 1
Data coding and analysis
Qualitative coding
Observation and shadowing data were coded using an open coding approach12 to identify OB and NICU team workflows. Examples of workflow processes included roles and responsibilities, handover activities, decisions made during handovers, workflow dependencies, artefacts used, communication challenges and information presentation strategies.
All audio-recorded verbal handovers were deidentified and transcribed verbatim for further analysis. Verbal communication for each handover was segmented into functional units called utterances. Utterances are psychological analogues of a single unit of experience including statements, commands and single words (eg, ‘okay’).5 13
Our modified clinical content framework comprised the following data elements: mother’s antepartum history, intrapartum and delivery course (table 1). The clinical content framework was developed in three phases. In the first phase, using a validated labour and delivery checklist for interdisciplinary communication,14 15 we created an initial list of clinical elements that were pertinent for characterising neonatal care continuity. Using this initial but comprehensive list of clinical content elements, an interdisciplinary team of practising clinicians from L&D and neonatal units used a consensus-driven approach to review and modify the initial list of clinical elements. This review and revision were based on the relevance, priority and importance of the clinical elements for neonatal care continuity. Finally, during the third phase, medical and nursing directors and managers of L&D and neonatal units participated in collaborative discussions to finalise and categorise these elements as core and ancillary elements. The core elements constituted essential information required for safe resuscitation and disposition of the newborn.16
Clinical content framework for neonatal handovers (core content elements are represented in bold)
Recent research reports have suggested that missing information regarding one or more of the core content elements can potentially cause adverse outcomes for the newborn and/or the mother.17 18 To identify missing elements, after all handovers were coded using the clinical content framework, we evaluated each handover for content completeness and content relevance. Content completeness was evaluated based on the presence of core and ancillary elements in a neonatal handover. Content relevance was evaluated based on the appropriateness of specific ancillary content elements in a handover. For this, we used the paediatric resident’s delivery note as our ‘gold standard’ for establishing the veracity of the verbal information.
The coding for the presence (or absence) and relevance (or irrelevance) of handover content was conducted in the following manner: when a core clinical content element was discussed during the handover, it was coded as being ‘present’. For example, if a patient’s HIV/hepatitis B was negative and this information was communicated during handover, it was coded as present. Similarly, when an ancillary content element was relevant to the patient, but was not discussed during the handover, it was coded as ‘missing’. For example, fetal heart rate/tracing was a relevant content element in cases where the fetus had bradycardia. In such a case, the fetal heart rate/tracing content element was coded as missing, if it was not discussed. In cases where an ancillary content element was irrelevant (and was also not discussed), it was coded as ‘irrelevant’. For example, maternal drug urine screen, if negative is not an essential core element and was not discussed during handover. Hence, it was coded as irrelevant (table 2).
Content completeness and relevance framework that was used for coding.
A subset of the handovers was coded by a second physician (n=10) with 98% of agreement for content completeness and with 99% agreement for content relevance. Coding discrepancies were resolved through discussion.
Adverse events
Using information from the resident delivery note and handover communication, we investigated whether missing information could have caused potential adverse events. For this, the first author captured the following information from the resident delivery note: resuscitation events including type of resuscitation, Apgar scores and disposition of the newborn. Next, we determined if one or more of the missing (both core and ancillary) elements during the handover communication could have led to adverse outcomes, as represented by greater need for resuscitation, poor 5 min Apgar scores or unexpected disposition to the NICU for the newborn. For example, if antenatal acute haemorrhage was omitted from neonatal handover and the newborn needed full resuscitation, the unavailability of such information could have caused potential delays and unnecessary interventions, leading to potential adverse outcomes.
This coding was performed by the first author and a paediatric fellow using a subset of 10 cases. There was 90% agreement on the cases, and differences were resolved through discussion.
Statistical analysis
We computed descriptive statistics regarding the percentage of missing core and ancillary clinical content elements during handover communication. Next, using logistic regression, we estimated the odds of potential adverse outcomes based on the number of missing clinical content elements per patient. All analyses were performed using R, and an alpha level of 0.05 was used.
Results
Fifty-two per cent (n=26) of the neonatal handovers had at least one missing clinical content element, with an average of 0.98 (median=1, IQR=0, SD=1.15) missing clinical content elements per handover. Thirty-two per cent (n=16) of the handovers had one or more missing core clinical content elements, with an average of 0.48 (SD=0.81) missing core clinical content elements per handover.
The common core missing elements were colour of amniotic fluid (16%, n=8), time of the rupture of membrane (14%, n=7), mother’s blood type (10%, n=5) and HIV/hepatitis B status (4%, n=2). Among the ancillary clinical content elements, the rupture membrane type was missing in 12% (n=6) of the neonatal handovers (figure 1; online supplementary appendix table 1).
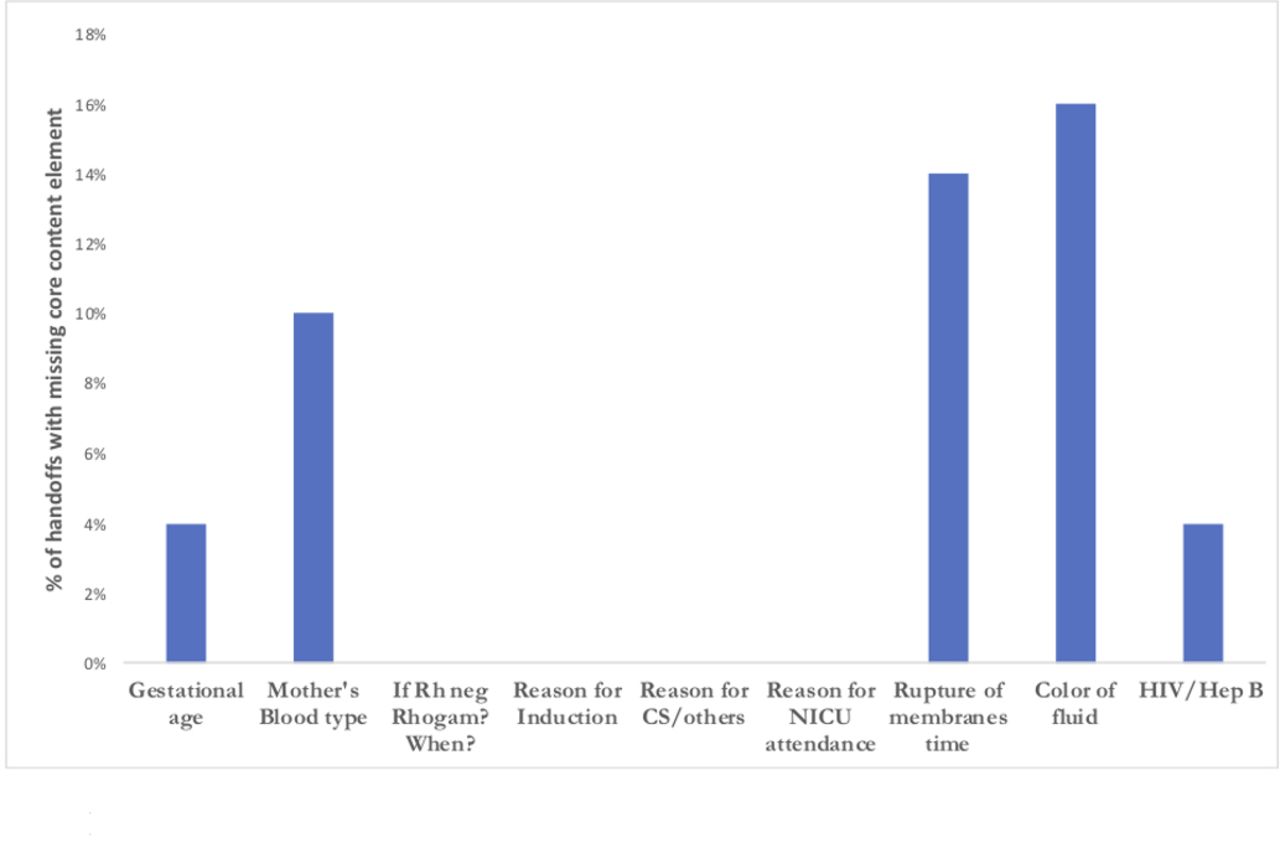
{kind=link}
Percentage of handovers with missing core clinical consent elements. NICU, neonatal intensive care unit.
Based on the logistic regression, we found that with unit increase in the number of missing clinical content elements increased the odds of adverse events by 2.39 (95% CI 1.18 to 5.37).
Interviews with the neonatal and OB teams highlighted the factors contributing to the high degree of missing information shared and its potential effects. Residents were dissatisfied by the content presented during handovers, describing it as of being ‘poor quality’ as they were often ‘one-liners’ with ‘incomplete information’. They described their frustration with the inaccuracies in the presented information. One resident remarked that ‘… a lot of the information is not clear. Sometimes the reason for NICU attendance is not clear and conflicting information provided by the baby nurse, mother’s nurse and the OB residents’. As a result, residents noted that they often do not fully rely on the presented information for their decision-making: ‘I don’t go off of it, because it’s been wrong, so often’.
Nurses attributed the poor quality of the handover content to three factors: limited time available for preparation, fragmentation information that was difficult to assemble in an efficient and quick manner and inconsistent use of information tools for aggregating or supporting handovers (table 3). These coupled with the lack of a structured process for handovers, led to considerable subjectivity in the organisation and varying presentation formats followed for handovers.
Examples from interviews regarding the challenges faced by residents and nurses during handovers
Nurses acknowledged that handover processes were ‘inconsistent’ and highlighted that at times information was simply not available. One nurse remarked that ‘patient information sheets [are] not available all the time’; other times there is not enough time to look up things and as a result ‘some things could be missed’ and at other times the nurses rely on ‘reading out the [information entered by the admitting nurse] on the antepartum assessment sheet, which is sometimes not updated’.
Discussion
Based on an exploratory study of interservice, interprofessional handovers between OB and NICU teams, we found that 52% of the handovers missed one or more clinical content elements. In nearly a third of the handovers, at least one core clinical content element was not discussed, increasing potential for adverse events for both the mother and the newborn. In addition, not discussing clinical content elements during handovers increased the potential for adverse events by over twofold. The high percentage of handovers where one or more core clinical elements was not discussed increases the potential for acute or long-term complications and adverse outcomes.19 Residents and nurses attributed these communication failures to the lack of a formalised mechanism or protocol for capturing or sharing the handover content.
Perceptions of poor handover quality is reflective of the lack of shared understanding between OB nurses and neonatal physicians—a critical function of effective handover communication.2 20 Our study findings highlight two fundamental issues that can impact the development of a shared understanding during neonatal handovers. First, there was mismatch between the expectations of the physicians and nurses regarding the information communicated during handovers. During handovers, OB nurses focused on maternal peripartum events and laboratory tests; although such information was relevant and important for care activities, residents expected additional information-related fetal imaging (including cardiac and ultrasound findings) and anomalies, which are key for determining the disposition of the newborn.
Second, there was considerable subjectivity in the manner in which nurses prepared and organised information for handovers, owing to a variety of factors including lack of time, unavailability of information, differing expertise and experience of the nurses, differences in communication styles and the differences in the tools used (eg, antepartum sheet, maternal admission sheet or personal notes).
Both these factors point to the need for creating a structure to organise the content and process of neonatal handovers. Although patient safety organisations have standardisation goals for handovers, much of these efforts have been on shift-based handovers.13 21 Interservice, interprofessional handovers present a new and unique challenge for handovers. Structured and streamlined communication in time-pressured situations have been supported through the use of standardised approaches such as checklists in surgery, and air-traffic controller–pilot communication using standardised formats have been found to be remarkably successful.22 Such a standardised strategy was repeatedly highlighted by all participants as a feasible and robust mechanism to reduce the inconsistencies in neonatal handover content and process.
This study has several limitations. The study was conducted in a single academic hospital setting, and hence some of our findings may not be generalisable to other settings. We used a convenience sample of 50 neonatal handovers. However, handovers were analysed at a granular level and were supplemented with interviews and observations. Although the potential for adverse outcome measure was independently coded and verified, it is a subjective measure. Finally, we did not use patient-related or clinician-related covariates in the logistic regression analysis.
References
Footnotes
Contributors AA and JA conceived the study; AA collected the data. All authors were involved in the coding, analysis and interpretation of the results. All authors were involved in the drafting of the manuscript and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval The Institutional Review Board approved this study and verbal consents were obtained from all participants.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement This is a qualitative study, and therefore the data generated are not suitable for sharing beyond that contained within the report. Further information can be obtained from the corresponding author.
Patient consent for publication Not required.