Article Text

Abstract
Background Not all children with an out-of-hospital emergency medical contact are transported by ambulance to the emergency department (ED). Non-transport means that after on-scene evaluation and possible treatment, ambulance personnel may advise the patient to monitor the situation at home or may refer the patient to seek medical attention by other means of transport. As selecting the right patients for ambulance transport is critical for optimising patient safety and resource use, we studied outcomes in non-transported children to identify possible risk groups that could benefit from ambulance transport.
Methods In a population-based retrospective cohort study of all children aged 0–15 years encountered but not transported by ambulance in Helsinki, Finland, between 1 January 2014 and 31 December 2016, we evaluated (1) 12-month mortality, (2) intensive care admissions, (3) unscheduled ED contacts within the following 96 hours after the non-transport decision and (4) the clinical status of the child on presentation to ED in the case of a secondary ED visit.
Results Of all children encountered by out-of-hospital emergency medical services, 3579/7765 (46%) were not transported to ED by ambulance. There was no mortality or intensive care admissions related to the non-transport. The risk factors for an unscheduled secondary ED visit after a non-transport decision were young age (p=0.001), non-transport decision during the early morning hours (p<0.001) and certain dispatch codes, including ‘dyspnoea’ (p<0.001), ‘vomiting/diarrhoea’ (p=0.030) and ‘mental illness’ (p=0.019). We did not detect deterioration in patients’ clinical presentation at ED traceable to non-transport decisions.
Conclusions Not transporting all children by ambulance after an out-of-hospital emergency medical contact was not associated with deaths, intensive care admissions or significant deterioration in general condition in our study population and healthcare system. Special attention and a formal non-transport protocol are warranted in certain subgroups, including infants.
- Accident & Emergency
- Outcomes research
- Health services research
- Paediatric Practice
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
In many out-of-hospital emergency medical systems, not all patients are transported by ambulance after an emergency medical contact. Careful selection optimises in-hospital and out-of-hospital resources.
Little is known about patient safety issues associated with not transporting all children to the emergency department (ED) by ambulance after an out-of-hospital emergency medical contact.
It is difficult to determine which children benefit from ambulance transport without evidence-based knowledge of out-of-hospital emergency care in children.
What this study adds?
Not all children with an out-of-hospital emergency medical contact needed ambulance transport to the ED for medical attention.
Not transporting all children by ambulance after an out-of-hospital emergency medical contact was not associated with deaths, intensive care admissions or deterioration in general condition.
Special subgroups, including infants and children with psychiatric conditions, often needed further medical attention after the initial out-of-hospital emergency medical contact.
Introduction
In many out-of-hospital emergency medical systems, not all patients are transported by ambulance to the emergency department (ED).1–4 Non-transport in emergency medical services (EMS) means that after on-scene evaluation and possible treatment, ambulance personnel may advise the patient to monitor the situation at home or may refer the patient to seek medical attention by transport other than ambulance. Selecting the right patients for ambulance transport is critical; not transporting patients in need of emergency treatment may compromise patient safety, whereas transporting low-acuity patients results in inappropriate resource use and increased costs. To optimise the selection of patients for ambulance transport, consultation and non-transport protocols5 6 have been proposed.
Children are a minority group in out-of-hospital emergency care, accounting for 5%–10% of patient contacts.3 7 Ambulance personnel have been reported to experience paediatric contacts as challenging. This may be due to unfamiliarity with paediatric equipment and reference values8 9 and a lack of evidence-based operation protocols. Moderately to severely injured children have been shown to benefit from ambulance transport,10 but there are no evidence-based guidelines to direct non-transport decision-making in out-of-hospital medical emergencies. Accordingly, paediatric transport decisions are suboptimal; ambulances are possibly being used as a taxi service for non-critical or non-medical transport,11 whereas critically ill children often arrive to the ED by means other than ambulance.12 13
Compared with other authors,2 4 we have previously7 14 reported a higher proportion of children not being transported by ambulance after out-of-hospital emergencies without significant patient safety compromise.7 For future protocol development, we studied the non-transport practice in children in a larger setting. Our aim was to determine whether not using ambulance transport for all children encountered by the EMS is safe.
Methods
Study area and population
The study covers all (n=7765) out-of-hospital ambulance responses for children (aged 0–15 years) in 2014–2016 in Helsinki, Finland (population 628 208; population 93 054, aged 0–15 years, in 2015).15
Organisation of EMS and healthcare system
Finland is a Nordic welfare state with a publicly financed universal healthcare system. Private care providers offer some primary and secondary care. The public healthcare system provides all out-of-hospital emergency care, including emergency call dispatching and ambulance transport. The gross domestic product was €38 309/inhabitant in 2015.
All emergency calls in the study area are dispatched through the same number, 112, and the same governmental emergency response centre. All dispatchers have completed at least a 1.5-year professional education, but they are not healthcare professionals. Based on the urgency of the call, a dispatcher first categorises the leading complaint to form a symptom code and then determines a triage class from A to D according to a formal, national questionnaire protocol. Dispatchers only evaluate the symptoms and their possible risks for the patient’s health but do not make any diagnoses. Ambulances are then dispatched according to the combination of symptom code and triage class.
In Helsinki, all out-of-hospital emergencies are responded to by a single provider, consisting of ambulances staffed by emergency medical technicians and paramedics. The ambulance personnel have the option of consultation with an emergency medical physician by phone, or they may call the physician-staffed mobile intensive care unit to the scene for assistance. The ambulance personnel work in 12 hours shifts, 09:00–21:00 or 21:00–9:00.
After examination and treatment, the personnel may decide that the patient does not need ambulance transport. When deciding not to transport by ambulance, the personnel must inform the patient or the caregivers on how to monitor and treat the condition, and on whether or when to visit healthcare services or call for help again. The non-transport decision is documented in the electronic patient record system. The non-transport codes are explained in the Results section (table 1). The cost of the ambulance transport is €14.25 to the patient, which is comparable to a short taxi ride, and is paid afterwards.
Non-transport codes and the proportion of all non-transported patients in the study population
Helsinki University Hospital has the only paediatric ED offering secondary and tertiary care in Helsinki.
Data collection
We obtained data on all out-of-hospital emergency medical encounters with children aged 0–15 years occurring in Helsinki between 1 January 2014 and 31 December 2016 from the electronic patient record system (Merlot Medi®, CGI Suomi Oy). The data cover all out-of-hospital ambulance responses in the study population during the study period. From the Helsinki University Hospital in-hospital patient record (Uranus®, CGI Suomi Oy), we studied the following outcomes as markers of adequacy of the non-transport decision: (1) 12-month mortality, (2) intensive care admissions, (3) ED contacts taking place without recommendation by the ambulance personnel (unscheduled ED contacts) and (4) in the case of an ED contact, the clinical status of the child on presentation to ED during the 96 hours following the non-transport decision.
One author (JO) reviewed all patient records. In the case of an ED contact, if the patient’s general condition was not explicitly stated to be good on arrival, the records were reviewed by two experienced paediatricians (ER and HS) separately. The paediatricians evaluated whether the patient had had possibly or clearly compromised vital functions.
Demographic data were obtained from Statistics Finland.15
Statistical analysis
To compare the factors associated with the risk of an unscheduled ED visit, the patients who were advised by ambulance personnel to visit ED by other means of transport (X-4; see table 1) were excluded. Continuous variables were tested using the Mann-Whitney U test, while χ2 test was used for categorical comparisons. Risk plots for shift duration were plotted using the locally estimated scatterplot smoothing (LOESS) method with ggplot2 package.16 Two-tailed p values were used with p<0.05 being considered significant. The analyses were carried out using R V.3.5.1.17
Patient and public involvement
There was no funding allocated to patient involvement in the study. For further studies aimed at improving non-transport decisions, we will involve patients and caregivers.
Results
There were 199 498 out-of-hospital emergency medical contacts during the study period. Of these, 7765 (3.9%) were for patients aged 0–15 years. The incidence of paediatric out-of-hospital emergency medical contacts was 4/1000 inhabitants and 27/1000 inhabitants aged 0–15 years.
Of the 7765 children encountered by the EMS, 4173 (53.7%) were transported by ambulance. Eight children (0.1%) died at the scene or were dead on arrival of the ambulance. Five children were not found by the ambulance personnel. Thus, 3579 children (46.1%) were not transported after out-of-hospital evaluation or treatment by ambulance personnel.
The age distribution of non-transported patients was U-shaped, and 55% were boys. Their median age was 3.95 years (IQR=8.74). In 3152 cases (88.3%), the non-transport decision was made without consulting an emergency medical physician. The most frequent dispatch codes for non-transported patients were ‘low-energy falls’ (683, 19.1%), ‘dyspnoea’ (553, 15.5%), ‘sudden deterioration of general condition’ (287, 8.0%), ‘slow deterioration of general condition’ (266, 7.4%) and ‘seizures’ (220, 6.1%).
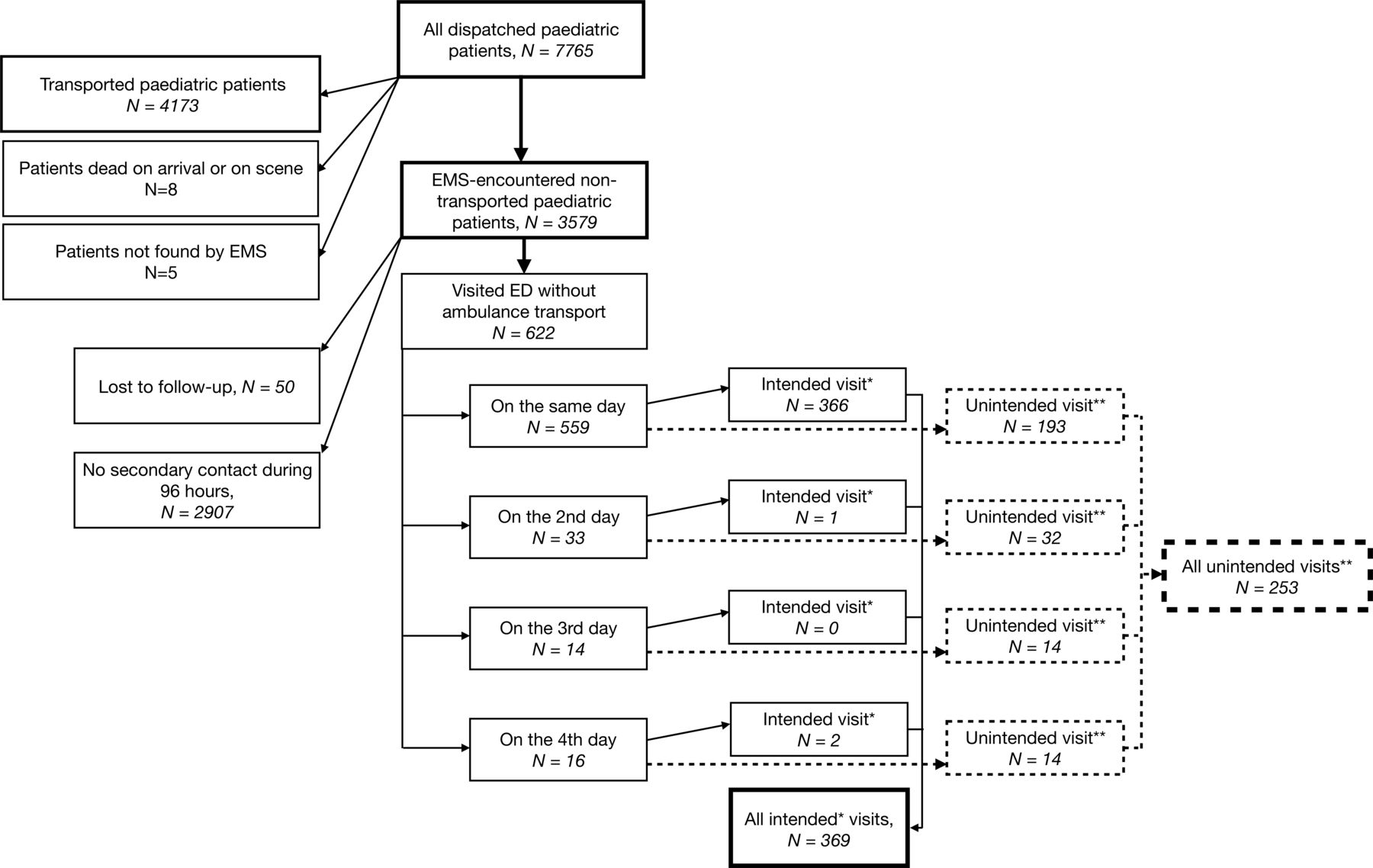
Of the non-transported patients, 622 (17.4%) visited the ED within 96 hours of the initial out-of-hospital emergency medical contact. Of these ED visits, 369 were advised by ambulance personnel; the personnel had judged an ED visit to be appropriate but did not consider ambulance transport necessary (X-4; see table 1). Thus, 253 out of 3579 non-transported patients (7.1%) visited the ED without having been advised to do so by the ambulance personnel. Of these ED visits, 193 (76.3%) occurred during the same day. Data for 50 patients, mostly tourists without a personal security number, were lost to follow-up. The patient flow is described in figure 1.
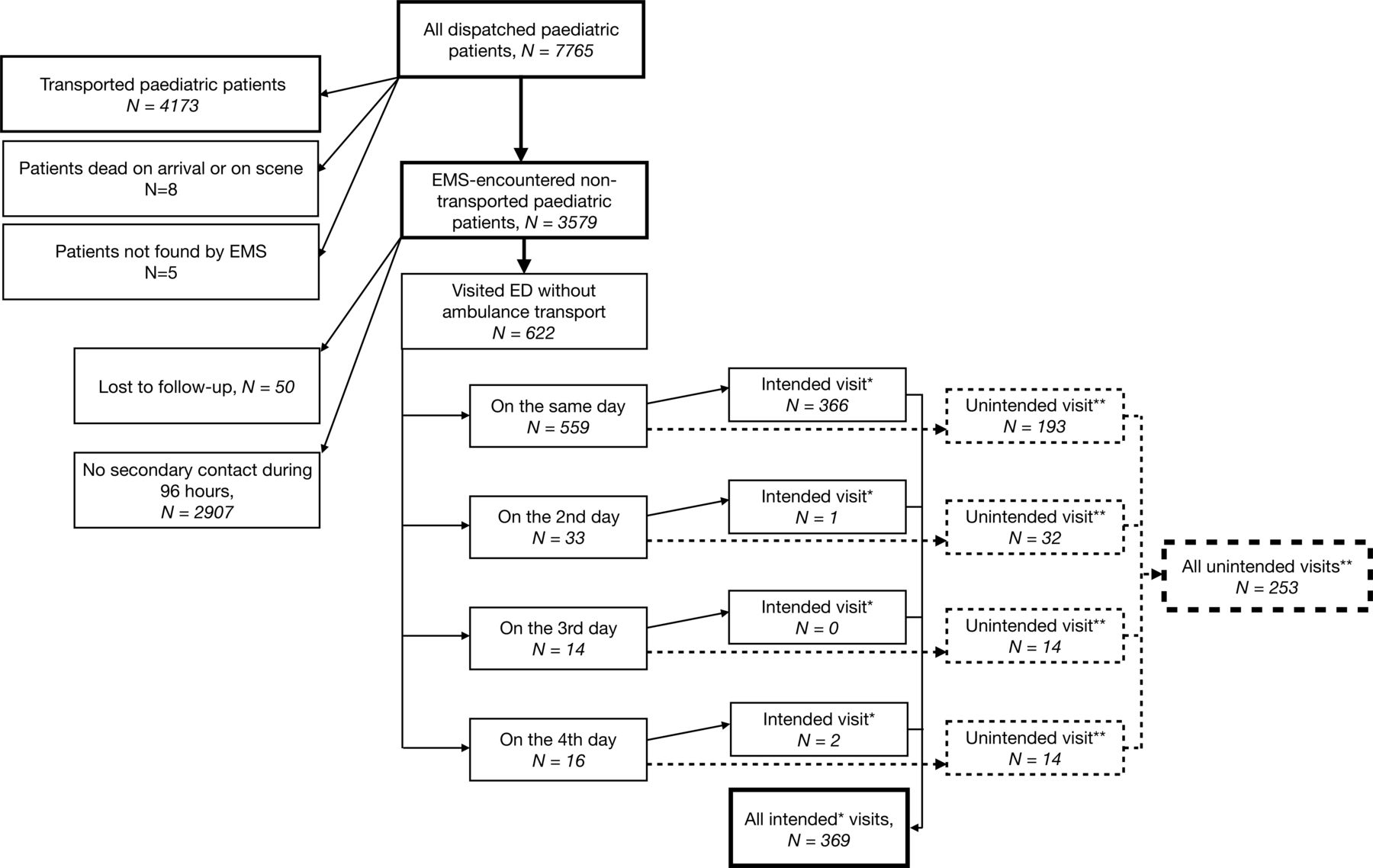
Patient flow in the study; retrieval of patients with unscheduled visits to the ED within 96 hours of the initial contact to out-of-hospital EMS. *Advised by ambulance personnel to visit ED by transport other than ambulance. **After evaluation by ambulance personnel, no need for transport, treatment or follow-up was detected, and the patient was informed that there was no need to visit ED by other means of transport. ED, emergency department; EMS, emergency medical services.
The general condition of 58 patients visiting the ED within the first 96 hours was not explicitly stated to be good on arrival. Two paediatricians (authors HS and ER) evaluated their in-hospital patient records separately and judged seven of them to have presented with possibly or clearly compromised vital functions. These patients are described in table 2. An analysis of their out-of-hospital patient records showed that the condition had progressed after the initial ambulance contact and had not been present at the initial contact. In 15/58 patients, one paediatrician stated that compromised vital functions were impossible to exclude afterwards, while the other paediatrician claimed that they were improbable. Otherwise, the evaluations were uniform.
Patients presenting with possibly or clearly compromised vital functions or in need of immediate life support interventions on arrival to the ED
Two patients were admitted to the intensive care unit within 96 hours of the out-of-hospital emergency medical contact. The first was an infant with atypical collapses and several ED visits over a month. The patient was not transported after a short collapse. Later, the patient was transported to the ED after a similar collapse and was monitored in the intensive care unit because of her young age. The second patient had a spontaneous internal haemorrhage needing operation and postoperative intensive care. According to the paediatric intensive care specialist responsible for the care of both patients, and external to the study group, the treatment in the intensive care unit would not have been avoided or shortened even if the patients had been transported.
Of all patients with a secondary visit, 360 (57.9%) were medicated at the ED. Eighty-one patients (13.0%) were given inhalations or oxygen as respiratory support, and 105 patients (16.9%) were admitted to the hospital ward. During the 1-year follow-up, there was one death clearly not associated with the initial emergency medical contact.
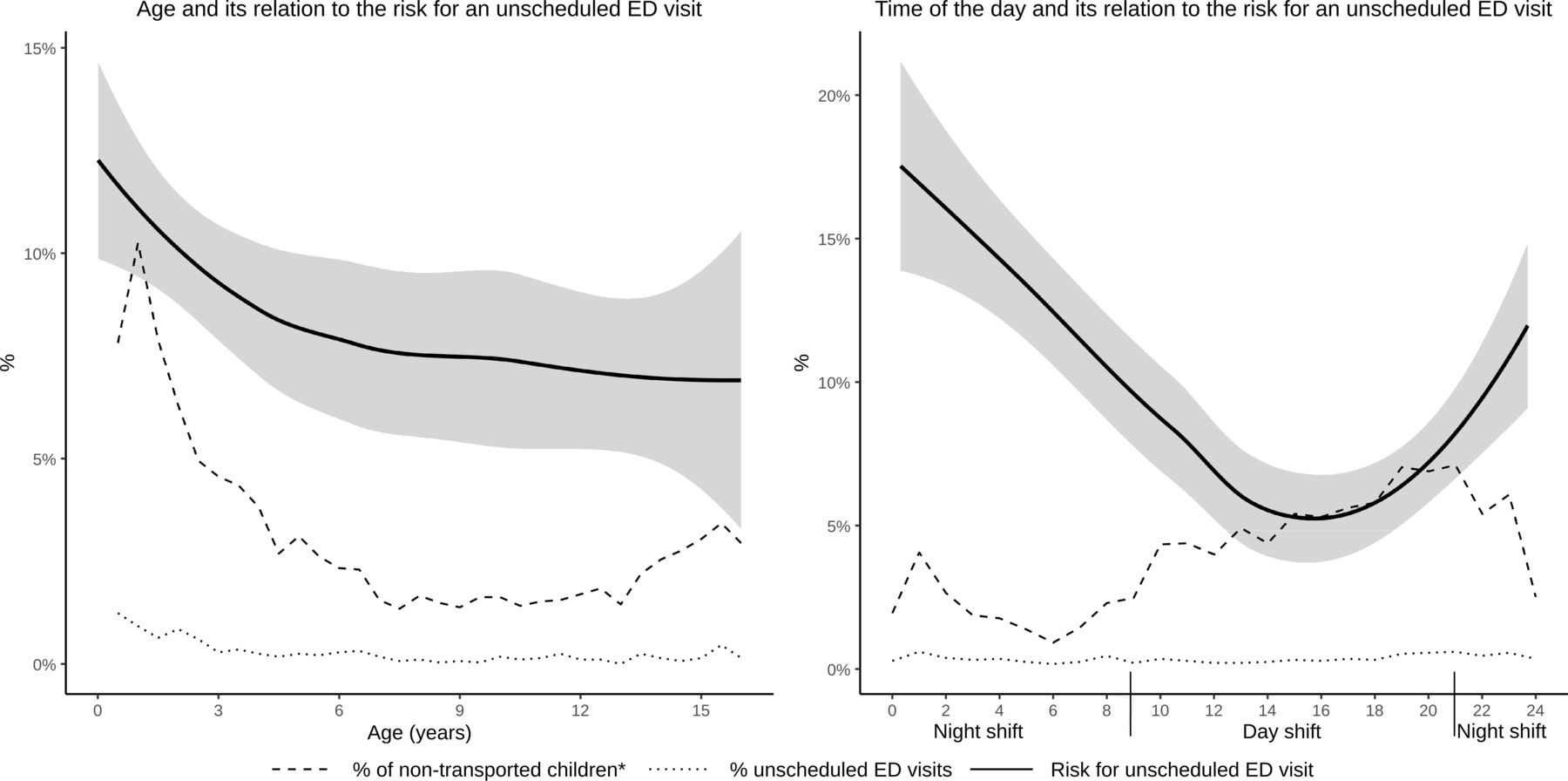
Young age was an independent risk factor for an unscheduled ED visit (p=0.001). The risk for an unscheduled ED visit was greater during the nightshift (p<0.001) and, if the out-of-hospital emergency medical contact occurred in the late hours, around midnight (p<0.001) (figure 2). The triage class of the call did not affect the risk. Symptom codes ‘dyspnoea’, ‘vomiting/diarrhoea’ and ‘mental illness’ were associated with a greater risk, and ‘low-energy fall’ as well as ‘allergic reaction’ with a lower risk of an unscheduled ED visit. The risk factors are shown in table 3. All of the studied factors are presented in online supplementary table 1.
Supplemental material
Factors affecting the risk of unscheduled ED visit within 96 hours after a non-transport decision by ambulance personnel
{kind=link}
{kind=link}
Impact of age of patient and time of day on the risk of unscheduled ED. *Those patients advised by ambulance personnel to visit ED by transportation other than ambulance were excluded from the analysis. ED, emergency department.
Discussion
Aiming to improve out-of-hospital emergency care, patient safety and resource use, we studied outcomes in children who had not been transported by ambulance after an out-of-hospital emergency medical contact. In a 3-year retrospective cohort study with 3579 non-transported children, we did not detect mortality, intensive care admissions or deterioration in patients’ clinical presentation traceable to non-transport decisions. Our results suggest that not all children with an out-of-hospital emergency medical contact need to be transported by ambulance to the ED.
We have repeatedly7 14 reported non-transport rates in children higher than those described by other authors.2 4 This may partly be explained by differences in the proportion of low-acuity emergency contacts, which is related to diverse sociodemographic factors, including patient age,3 12 socioeconomic status12 18 and parental health literacy.18 We think it unlikely that the higher non-transport rate would be due to a greater number of emergency responses for children in our healthcare system. First, the emergency response centre operators adhere to strict protocols while dispatching. Second, the proportion of children of all emergency responses (3.9%) is lower than in other published studies.1–3 7 19 This suggests that unnecessary contacts in children were not over-represented.
Since we did not detect mortality or intensive care admissions due to non-transport, we also investigated the general condition of non-transported children at the time of a secondary ED contact. We hypothesised that by analysing the presentation of these children, we could detect possible patient safety compromises in out-of-hospital care. Of non-transported children, 7.1% had an unscheduled ED visit within 96 hours of the initial contact. Existing studies report varying ED revisit rates for non-transported children.4 7 20 Unscheduled revisits are rather frequent also after evaluation by a physician in the ED setting,21 as predicting disease progression in children is difficult. Thus, we do not consider the 7.1% revisit rate in our study to be high.
Young age was associated with unscheduled ED visits (figure 2). This may be partly explained by age-dependent differences in the causes for out-of-hospital emergency medical contacts. It is also possible that ambulance personnel had difficulties in evaluating infants. Indeed, previous studies have reported confusion and discomfort in emergency medical professionals attending to young children.8 9
The risk of an unscheduled ED visit (figure 2) was greatest during the early morning hours. It would be tempting to conclude that the decision-making process was altered by fatigue. Still, as most non-transport decisions are made in cooperation with the child’s caregivers, it is possible that many parents preferred to wait until office hours. When the child’s condition does not warrant immediate ED care, this kind of decision is also practical for the ED.
The symptom codes associated with greater risk for an unscheduled ED visit were dyspnoea, vomiting/diarrhoea and mental illness. The progression of dyspnoea, vomiting and diarrhoea, typically caused by acute infections, is difficult to predict. The higher risk for unscheduled ED visits with these symptom codes seems inherent to the related diseases themselves.22 Because the number of non-transported children with mental illness is low, it is possible that ambulance personnel did not have sufficient experience to assess their presentation. As this minor patient group would not lead to a significant patient load in the out-of-hospital EMS or ED, non-transport decisions in children with acute psychiatric problems should be critically weighed.
Not transporting all patients highlights several priority issues in out-of-hospital and in-hospital emergency care: the increase in ambulance requests,6 the overuse of ambulances for non-emergency situations7 and the increase in ED visits.5 In addition, overtriaging low-acuity children for ambulance transport may expose them to unnecessary traffic hazards.23 24 Especially infants are seldom transported correctly by ambulance, and family cars are often better equipped for child transport.24 Unnecessary ambulance transport may also inflict stress on parents and children.
Our study has several limitations. First, the lack of out-of-hospital key performance indicators25 or operation protocols19 was a challenge for our study, and we had to rely on subjective criteria to evaluate the accuracy of out-of-hospital care. Second, we did not have access to patient records in primary healthcare. Nonetheless, all children with moderate or severe impairment in health would have been referred to the only paediatric ED in the area and are thus included in our data search. Third, we acknowledge that children aged 0–15 years form a heterogeneous group with various age-related reasons for ambulance contacts. To confirm the results of our study in different age groups, larger studies are needed. Fourth, we are not able to state whether the greater risk of revisits for certain symptom codes represents causality or not. Still, it enables the ambulance personnel to recognise which children may have an elevated risk for ED revisits.
Out-of-hospital non-transport and its safety are highly dependent on accessibility of other health services, the capabilities and training of the ambulance personnel, and the available resources. Thus, the results of this study may only be generalisable to areas with similar circumstances. Still, these results may encourage other emergency medical systems to pilot non-transport protocols and to evaluate the safety and feasibility of existing ones.
Conclusions
Not all children with an out-of-hospital emergency medical contact need ambulance transportation to ED. Not transporting all children by ambulance was not associated with deaths, intensive care admissions or significant deterioration in general condition in our study population and healthcare system. Special attention and possibly a formal non-transport protocol are warranted in certain subgroups, including infants.
References
Footnotes
Contributors JO, HS and HH-R conceptualised and designed the study, collected the data, carried out the initial analyses, drafted the initial manuscript, and reviewed and revised the manuscript. ER and MK participated in the design of the study, reviewed the initial data collection and initial analyses, and critically reviewed and revised the manuscript. ML designed the data analysis instruments, coordinated and supervised data analysis, and critically reviewed the manuscript. All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Funding One of the authors (HS) received a grant from the Foundation for Paediatric Research, Finland (Lastentautien Tutkimussäätiö).
Disclaimer The Foundation had no role in the study design, data collection or interpretation of the results.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study protocol was approved by the institutional review board of Helsinki University Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.