Article Text

Abstract
Background Inhaled corticosteroids are associated with a risk of growth suppression in children. The aim of the present study was to assess what children with asthma, lay people and paediatricians feel about the risk of growth suppression by inhaled corticosteroids.
Methods A questionnaire was completed by seven populations consisting of 9–19 years old children and adolescents with asthma; 9–19 year olds with another chronic illness; healthy 9–19 year olds; parents to children with chronic conditions; parents to healthy schoolchildren; young adults; and paediatricians.
Results A total of 1216 individuals completed the questionnaire. A total of 867 individuals (74.6%) would not worry about a risk of 1-year growth suppression in the range of 0.5–2 cm (range: 233 (63.3%) in parents to patients in a secondary referral centre to 59 (86.8%) in the group of paediatricians (χ 2 53.3, df 12, p<0.001; γ −223, error 0.042, p<0.001). A total of 745 individuals (64.3%) said that a loss in final height of 0.5–2 cm would not worry them (range: 34 (54.0%) in paediatricians to 119 (76.3%) in parents to healthy children (χ 2 49.5, df 12, p<0.001; γ −0.073, error 0.039, p=0.06).
Conclusions Most children with asthma, lay people and paediatricians do not worry about the risk of growth suppression of inhaled corticosteroids in the range up to 2 cm. Paediatricians worry less about the risk of 1-year growth suppression but more about final height suppression than children with asthma and other groups of children and adults. Paediatricians need to address the different concerns of some of their patients on this issue.
- Questionnaire
- growth
- short term growth
- asthma
- inhaled corticosteroids, paediatricians, lay people
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Depending on dose, device and administration regimen, inhaled corticosteroids may be associated with a risk of growth suppression.
The risk of growth suppression appears to be most marked during the first year after treatment is initiated.
The suppression of final height may be in the range of 0.5–2 cm.
What this study adds?
Most children with asthma, lay people and paediatricians do not worry about the risk of growth suppression of inhaled corticosteroids.
Paediatricians may worry less about the risk of 1-year growth suppression but more about final height suppression than children with asthma and other groups of children and adults.
Paediatricians need to address the different concerns of some of their patients on this issue.
Introduction
Inhaled corticosteroids are commonly used as first line in the treatment to improve control of bronchial asthma in children.1 The drugs are efficacious and when used in recommended doses and administration regimens, the risk of serious adverse effects is considered small.1 Depending on the specific corticosteroids used, modulation, device and administration regimen, however, a risk of suppression of longitudinal growth rate may be detectable at daily doses of 200–400 µg.2 The risk has been evidenced by several clinical short and intermediate term trials using treatment periods of few weeks to a year.2–5 Short-term studies of growth rate suppression by inhaled corticosteroids have found that when they are withdrawn catch-up growth occurs compensating for any suppressive effects.6 A prospective, randomised, double blinded clinical trial of inhaled budesonide 400 µg daily during three childhood years was followed by assessment of final height in children who had participated in the study.7 As compared with individuals who did not receive active treatment with budesonide, mean final height in budesonide treated individuals was 1.2 cm shorter.
The risk of serious adverse effects of inhaled corticosteroids may cause concerns in parents, reduce adherence with administration regimens and cause poor asthma control.8–11 To what extent the risk of growth suppression per se may worry children with asthma and their families, however, have not been assessed. The aim of the present study was to assess what children with asthma, lay people and paediatricians feel about the risk of a reduction in height that is similar to that documented in earlier studies.2–7
Patients and methods
Based on previous structured questionnaire studies that included approximately 1200 children and adolescents giving robust data, we aimed at including a similar number of individuals in the present study.12 13 A structured hard copy questionnaire was handed out to and completed by seven populations:
Children and adolescents with asthma 9–19 years attending a secondary paediatric referral centre.
Children and adolescents with chronic conditions others than asthma aged 9–19 years attending a secondary paediatric referral centre.
Healthy school students aged 9–19 years.
Nursing and teacher training college students aged 20–25 years.
Parents to children and adolescents attending a secondary paediatric referral centre.
Parents to healthy school students.
Paediatricians attending The Danish Society of Paediatrics Annual Meeting 2017.
Oral and written information about the rationale of the study was given to all participants individually or in groups. All children in the defined age ranges and all parents attending our clinic during the period of 1 October and 21 December 2016 were asked to participate in the study and defined the groups A, B and E. They were informed individually when attending scheduled appointments in our clinic. Parents in group F were informed in their children’s classrooms at parent–teacher conferences arranged by their children’s schools. On that occasion, the parents were asked for their consent to our inviting their children to complete the questionnaire. Groups C and D were informed in groups in their classrooms. Group G was informed at a plenum session at the 2017 Annual Meeting of the Danish Paediatric Society. All parents to children aged 9–15 years gave consent to their children’s participation, their children gave assent and all children themselves completed the questionnaire. Individuals ≥16 years of age consented themselves to participation.
The questionnaire was anonymous and did not record any personal data. The participants were asked to give information on three items: sex, age and asthma history; however, the groups of E, F and G of adult individuals were not asked about their age. In addition. all groups were asked to answer the questions:
Would you worry about a potential growth suppression of 0.5–2 cm in a child treated with inhaled corticosteroids during a year if it was followed by catch-up growth and had no effect on final height?
Would you worry about a potential suppression of final height of 0.5–2 cm due to many years’ treatment with an inhaled corticosteroid?
If a child with chronic asthma would need continuous treatment with an inhaled corticosteroid, which degree of suppression in final height do you feel would be acceptable?
Answer options to questions 1 and 2 were: a: no; b: yes, I would worry a little; or c: yes, I would worry a lot. Answer options to question 3: were: a: ≤1 cm; b: ≤2 cm; c: ≤3 cm; d: ≤4 cm; e: ≤5 cm; f: ≤10 cm; or g: no suppression would be acceptable.
Statistics
Data were processed and analysed by IBM SPSS V.20 Statistics.14 Pearson’s χ2 test for tables with nominal scaled variables was performed for bivariate analyses. The Goodman Kruskal’s gamma (γ) test was used to test for directions of associations among cross-tabulated ordinal scaled variables.15 The <0.05 significance level was used.
Patient and public involvement
Patients or the public were not involved in the design, conduct and reporting of the research.
Results
A total of 1236 individuals were invited to participate in the study, and a questionnaire was handed out to all of them. Four individuals in group A and seven in group B, however, said that they could not read the questionnaire; six individuals in group E returned the questionnaire without having answered any questions, and three individuals in group G left the auditorium when the questionnaire was handed out. So, 1216 (98.5%) did and 20 (1.5%) individuals did not complete the questionnaire. The number (%) of completing individuals by groups was: A: 146 (12.0); B: 106 (8.7); C: 249 (20.5); D: 114 (9.4); E: 374 (30.8); F: 158 (13.0); and G: 69 (5.7). Mean age of groups A, B, C and D was 12.7, 13.3, 15.6 and 25.3 years, respectively. Information on sex was given by 1149 individuals (94,5%), 658 (57.3%) being males and 491 females (43.7%), and the distribution of sex (males/females) by groups were: A: 83/58; B: 45/46; C: 117/121; D: 6/97; E: 204/158; F: 70/85; G: 17/42 (χ2 99.4, df 6, p<0.001; γ 0.255, error 0.039, p<0.001). A total of 1113 (91.5%) gave information on asthma history. The distribution of asthma/no asthma by groups were: A: 137/0; B: 0/85; C: 37/176; D: 21/81; E: 216/137; F: 31/120; and G: 14/55 (χ2 422.5, df 6, p<0.001; γ 0.547, error 0.033, p<0.001).
Question 1: ‘Would you worry about a potential growth suppression of 0.5–2 cm in a child treated with inhaled corticosteroids during a year if it was followed by catch-up growth and had no effect on final height?’ was answered by 1162 (95.3%) (figure 1). A total of 867 individuals (74.6%) would not be worried about a risk of 1-year growth suppression in the range of 0.5–2 cm (range: 233 (63.3%) in parents to patients in a secondary referral centre (group E) to 59 (86.8%) in the group of paediatricians (group G) (χ 2 53.3, df 12, p<0.001; γ −223, error 0.042, p<0.001). A total of 242 (20.8%) and 53 (4.6%) would worry a little or a lot, respectively.
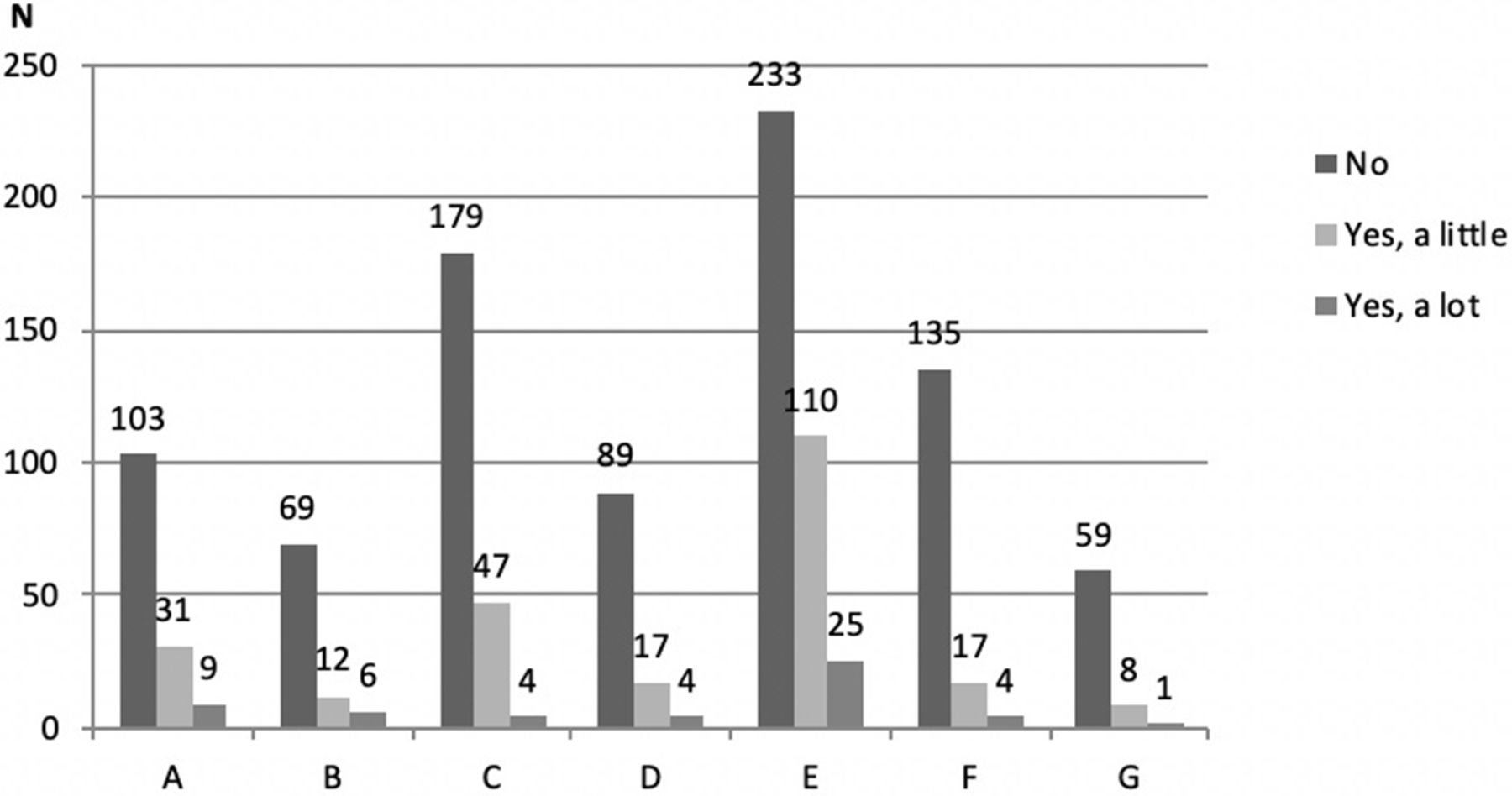
Distribution of answers to question 1: ‘Would you worry about a potential height growth suppression of 0.5–2 cm in a child treated with inhaled corticosteroids during a year if it was followed by catch-up growth and had no effect on final height?’ in n=1162 by groups: A: children and adolescents with asthma aged 9–19 years; B: children and adolescents with chronic conditions others than asthma aged 9–19 years; C: school students aged 9–19 years; D: nursing and teacher training college students aged 20–25 years; E: parents to children and adolescents attending a secondary paediatric referral centre; F: parents to healthy school students; and G: paediatricians attending the Danish Society of Paediatrics Annual Meeting 2017.
Question 2: ‘“Would you worry about a potential suppression of final height of 0.5–2 cm due to many years’ treatment with an inhaled corticosteroid?’ was answered by 1159 (95.3%) individuals (figure 2). A total of 745 individuals (64.3%) said that a loss in final height of 0.5–2 cm would not worry them (range: 34 (54.0%) in paediatricians (group G) to 119 (76.3%) in parents to healthy children (group F) (χ2 49.5, df 12, p<0.001; γ −0.073, error 0.039, p=0.06). A total of 321 (27.7%) and 93 (8.0%) would worry a lot.

{kind=link}
{kind=link}
Distribution of answers to question 2: ‘Would you worry about a potential suppression of final height of 0.5–2 cm due to many years’ treatment with an inhaled corticosteroid?’ in n=1159 individuals by groups: A: children and adolescents with asthma aged 9–19 years; B: children and adolescents with chronic conditions others than asthma aged 9–19 years; C: school students aged 9–19 years; D: nursing and teacher training college students aged 20–25 years; E: parents to children and adolescents attending a secondary paediatric referral centre; F: parents to healthy school students; and G: paediatricians attending the Danish Society of Paediatrics Annual Meeting 2017.
Question 3: ‘If a child with chronic asthma would need continuous treatment with an inhaled corticosteroid which degree of suppression in final height do you feel would be acceptable?’ was answered by 1156 (95.1%) individuals. The distribution of answers by groups is given in table 1. The distribution was statistically significant (χ 2 100.4, df 30, p<0.001; γ −0.065, error 0.023, p<0.005). The highest degree of accepted suppression was seen in group C of school students in whom a final height suppression of ≤5 cm was accepted by 31.7%. The highest percentage of accepted suppression was found in group E of college students in whom a suppression of ≤2 cm was accepted by 37.7%. The highest percentage of individuals (25.3%) who would only accept a ≤1 cm suppression was found in group B of children with other conditions than asthma and in group E consisting of parents to such children (25.3%). A ≤3 cm suppression was accepted by 23% of group A consisting of children with asthma and by 35.2% of group G consisting of paediatricians and children with asthma would accept less suppression a of final height at all levels than paediatricians.
Distribution of answers to question 3: ‘If a child with chronic asthma would need continuous treatment with an inhaled corticosteroid which degree of suppression in final height do you feel would be acceptable?’ in n=1156 individuals by groups: A: children and adolescents with asthma aged 9–19 years; B: children and adolescents with chronic conditions other than asthma aged 9–19 years; C: school students aged 9–19 years; D: college students 20–25 years; E: parents to children and adolescents attending a secondary paediatric referral centre; F: parents to healthy school students; and G: paediatricians attending the Danish Society of Paediatrics Annual Meeting 2017
Cross-tabulations of the item sex showed no statistically significance in question 1 (χ 2 0.01, df 2, p=0.99; γ 0.005, error 0.067, p=0.94) or 2 (χ 2 4.45, df 2, p=0.11; γ 0.101, error 0.059, p=0.09). In question 3 bivariate analysis of sex found more women (27.9%) than men (21.9%) accepting ≤3 cm suppression (χ 2 12.4; df 5, p=0.03); however, ordinal by ordinal testing was not statistically significant (γ 0.008, error 0.044, p=0.86) (table 2).
Distribution of answers to question 3: ‘If a child with chronic asthma would need continuous treatment with an inhaled corticosteroid which degree of suppression in final height do you feel would be acceptable?’ cross-tabulated with the items sex (n=981)* and asthma (n=1046)*
Cross-tabulations of the item asthma with the answers to questions 1–3 showed no statistically significance in question 1 (χ 2 3.2, df 2, p=0.20; γ 0.121, error 0.068, p=0.08) or 2 (χ 2 1.1, df 2, p=0.58; γ −0.053, error 0.060, p=0.39). In question 3, there was a statistically significant tendency for individuals with asthma to accept less growth suppression than individuals without asthma with 31.3% and 20.9% of individuals with asthma accepting ≤2 cm and ≤3 cm suppression, respectively, and 24.5% and 28.8% of individuals without asthma accepting ≤2 cm and ≤3 cm suppression, respectively (χ 2 19.6, df 5, p=0.01; γ 0.102, error 0.045, p=0.02) (table 2).
Discussion
Most parents to children with asthma feel that inhaled corticosteroids are needed for optimal control of the condition, and they may acknowledge the need for efficacious anti-inflammatory treatment; however, they may also worry about adverse effects.8–11 A qualitative interview study of 18 North American families found that the families seemed to have an understanding that the benefits of the drugs outweighed the risk of side effects.9 Using a questionnaire in 622 families of whom 80% were Caucasians, 72% of parents were reported to say that the inhaled corticosteroid therapy was necessary; however, 30% had strong concerns about the medications.8 When 170 Malaysian parents were asked about important aspects about administering inhaled corticosteroids to children, only 15% reported difficulties in using the inhaler, whereas 91% said that important issues were worries about adverse effects.10 A structured questionnaire of 500 Turkish parents to children on inhaled corticosteroids reported that more than 50% of the parents were afraid of corticosteroids.16 Corticophobia was associated with poor adherence rates8 and asthma control.16 That was evidenced also in a Dutch population of 8-year-old children with asthma in whom 45% were found to have uncontrolled asthma.11 In addition to low maternal education and parental necessity beliefs about medications, concerns about potential adverse effects were associated with poor asthma control. Finally, a questionnaire in 182 Dutch 12–18 years old adolescent inhaled corticosteroid users found that 10% of them had serious concerns about adverse effects, though, details about their concerns were not assessed.17
To our knowledge, specific elements in families’ worries about inhaled corticosteroids have not previously been assessed. The first randomised, double blind trial of inhaled corticosteroids that investigated longitudinal growth in children with asthma treated with inhaled corticosteroids was published in 1991 finding a dose-related suppression.18 During the subsequent decades, much focus has been on the growth suppressive effect of these drugs as evidenced by several trials.2–5 7 Furthermore, the issue has had continuous interest in the lay public and media.19 Therefore, we decided to focus on the risk of growth suppression in children. Considering the evidence that the risk of mean growth suppression of inhaled corticosteroids appears to be around 1 cm with ranges between approximately 0.5–2 cm during the first year of treatment and at final height assessments, these were the data that were used in the present questionnaire.2–5 7 In addition to assessing adult populations and a population of paediatricians, we aimed at evaluating children’s own feelings about the risk. We have previously shown that when age-adjusted information is given, children may themselves consent to participation in clinical non-interventional studies from around age 10 years.12 Therefore, the questionnaire was designed to be as simple and straightforward as possible excluding information on race, ethnicity, parental education and socioeconomic factors even though such factors may be suggested to influence patient beliefs of effects of medical treatments.8–11 20 21 Though an individual’s own weight and height might be speculated to influence their feelings about the risk of growth suppression, such data were not included because in our experience children’s perception of their own height may be even more unreliable than parental perceptions.22
Since we wanted to perform comparative analyses of subgroups, we defined seven populations consisting of children and adolescents with and without asthma, parents to chronically ill children in our clinics and parents to healthy schoolchildren in addition to young adults and doctors. Data from individuals presenting in our clinic were collected during approximately 3 months. That explains the variations among the number of individuals in the patient groups and parent group in our clinic since often two parents attended the clinic as opposed to only one child per family. Though a majority of college students were women, we felt it was important to include the group of non-parent young adults. We speculated that young adults might feel differently about growth suppressive risks than parents since many perspectives on life changes with parenthood.23 That, however, seemed not to be the case.
In the total population, 74.6% of the individuals would not be worried about a risk of 1-year growth suppression in the range of 0.5–2 cm, and 64.3% said that a loss in final height of 0.5–2 cm would not worry them. The variations among groups were statistically significant, and the most conspicuous findings were that of all groups paediatricians worried the least about the risk of 1-year growth suppression but the most about suppression of final height. However, the ≤3 cm level of suppression was accepted by only 23% of children with asthma but by 35% of paediatricians and, generally, children with asthma would accept less final height suppression than paediatricians. The trend was supported by the cross-tabulation analyses with asthma and the levels of accepted final height suppression showing a statistically significant tendency for individuals with asthma to accept less growth suppression than individuals without asthma with 31.3% and 20.9% of individuals with asthma accepting only up to 2 cm or 3 cm suppression of final height, respectively. To some extent perhaps, variations in feelings about the risk of 1-year growth suppression may reflect that paediatricians may be more familiar with the concept of catch-up growth than lay people or, indeed, children. However, paediatricians may not appreciate that children with asthma due to their chronic condition may worry to a greater extent than themselves about the severity of suppression of adult height. Finally, experience from clinical management of children with asthma and evidence from the literature have indicated that in many conditions patients and doctors may not agree on factors influencing adherence with drug administration regimens.24 The present data highlight the need for paediatricians who take care of children with asthma treated with inhaled corticosteroids to engage in effectively communicating pros and cons of the inhaled anti-inflammatory treatments to a substantial number of patients.
References
Footnotes
Contributors The protocol was written by ODW, who also informed all participants, collected, processed and interpreted the data and wrote the paper.
Funding The study was supported by a grant from ‘The Foundation for Research and Development in Secondary Referral Centres’.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethics Committee Region Midtjylland, Denmark, and the Data Protection Agency, Denmark, decided that the questionnaire did not require authorisation.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.