Article Text

Abstract
Background Expired carbon dioxide (ECO2) indicates degree of lung aeration immediately after birth. Favourable ventilation techniques may be associated with higher ECO2 and a faster increase. Clinical condition will however also affect measured values. The aim of this study was to explore the relative impact of ventilation factors and clinical factors on ECO2 during bag-mask ventilation of near-term newborns.
Methods Observational study performed in a Tanzanian rural hospital. Side-stream measures of ECO2, ventilation data, heart rate and clinical information were recorded in 434 bag-mask ventilated newborns with initial heart rate <120 beats per minute. We studied ECO2 by clinical factors (birth weight, Apgar scores and initial heart rate) and ventilation factors (expired tidal volume, ventilation frequency, mask leak and inflation pressure) in random intercept models and Cox regression for time to ECO2 >2%.
Results ECO2 rose non-linearly with increasing expired tidal volume up to >10 mL/kg, and sufficient tidal volume was critical for the time to reach ECO2 >2%. Ventilation frequency around 30/min was associated with the highest ECO2. Higher birth weight, Apgar scores and initial heart rate were weak, but significant predictors for higher ECO2. Ventilation factors explained 31% of the variation in ECO2 compared with 11% for clinical factors.
Conclusions Our findings indicate that higher tidal volumes than currently recommended and a low ventilation frequency around 30/min are associated with improved lung aeration during newborn resuscitation. Low ECO2 may be used to identify unfavourable ventilation technique. Clinical factors are also associated with persistently low ECO2 and must be accounted for in the interpretation.
- Resuscitation
- Neonatology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Expired CO2 (ECO2) is low immediately after birth before the lung liquid is cleared.
ECO2 may serve as a marker for effective ventilations in intubated patients.
What this study adds?
The quality of ventilations are more important than the clinical condition for measured ECO2 during the first minutes of bag-mask ventilation in newborn resuscitation.
Ventilation frequency around 30/min gives the highest ECO2.
Tidal volumes of 10–14 mL/kg are associated with the highest ECO2 and the shortest time to reach ECO2 >2%.
Introduction
Around 3%–6% of newborns receive positive pressure ventilation at birth to facilitate transition and establish cardiorespiratory stability.1–3 Heart rate (HR) response is an important indicator of effective resuscitation,3 4 but cannot directly assess ventilation. Hooper et al found that expired carbon dioxide (ECO2) indicates degree of lung aeration immediately after birth.5
Newborn lungs are liquid filled. Before functional residual capacity is sufficiently established, gas exchange is diffusion limited.6 To detect ECO2, liquid must be cleared and air must enter the alveoli. ECO2 increases rapidly in the first minute of extrauterine life during spontaneous breathing, but slower if positive pressure ventilation is needed.7–9 Capnography may help identify unfavourable technique and guide ventilations during newborn resuscitation.10–14 There is currently insufficient evidence that ECO2 monitoring during newborn resuscitation affects outcome.3 15 ECO2 depends, in addition to ventilation, on metabolism and pulmonary circulation.16
Optimal ventilation strategies for rapidly establishing effective pulmonary gas exchange in non-breathing newborns have not been fully determined. Recent studies indicate that larger tidal volumes (VTE) than the 4–8 mL/kg currently recommended may cause faster increase in HR.4 17 18 Guideline recommendations for ventilation frequency vary between the USA (40–60/min) and Europe (30/min), and evidence for any recommendation is sparse.19 20
In this study, we aimed to explore the relative impact of ventilation factors (VTE, frequency, mask leak and pressure) and clinical factors (birth weight (BW), Apgar scores and initial HR) on ECO2 during bag-mask ventilation (BMV) in resuscitation of term and near-term newborn infants. Better understanding may improve interpretation of ECO2 measurements and help determine optimal ventilation strategies.
Methods
Study design and setting
Observational study performed between 1 March 2013 and 1 June 2017 at Haydom Lutheran Hospital, a rural Tanzanian referral hospital with 4–5000 deliveries annually. The study was part of Safer Births, a research consortium on labour surveillance and newborn resuscitation in low-income settings.4 21 22 Midwives and nursing students conducted most vaginal deliveries. Newborn resuscitation was mainly the responsibility of midwives.
Data collection, equipment and training
Trained non-medical research assistants observed all deliveries, documented time intervals and recorded perinatal information.2 A newborn resuscitation monitor developed for research by Lærdal Global Health, Stavanger, Norway was mounted on the wall above all resuscitation tables (23). Each monitor was equipped with a self-inflating bag (230 mL standard or 320 mL Upright bag-mask; Laerdal Medical, Stavanger, Norway) and a dry-electrode ECG sensor to be easily placed around the newborns’ trunk. Sensors for side-stream CO2 (ISA; Masimo, Irvine, California, USA), pressure (Freescale semiconductor, Austin, Texas, USA) and flow (Acutronic Medical Systems, Hirzel, Switzerland) to record ECO2 and ventilation parameters were placed between the mask and bag; the attachment device added a dead space of 1 mL. The monitors provided HR feedback. ECO2 and ventilation parameters were not displayed.
The local newborn resuscitation procedure followed the Helping Babies Breathe (HBB) guidelines.24 HBB was introduced at the study site in 2009. Midwives participated in full-day HBB courses one to two times yearly, and were educated to use clinical signs including chest rise and HR feedback to guide resuscitation. Low-dose, high-frequency skills training as described by Mduma et al was encouraged.22
Formation of the cohort
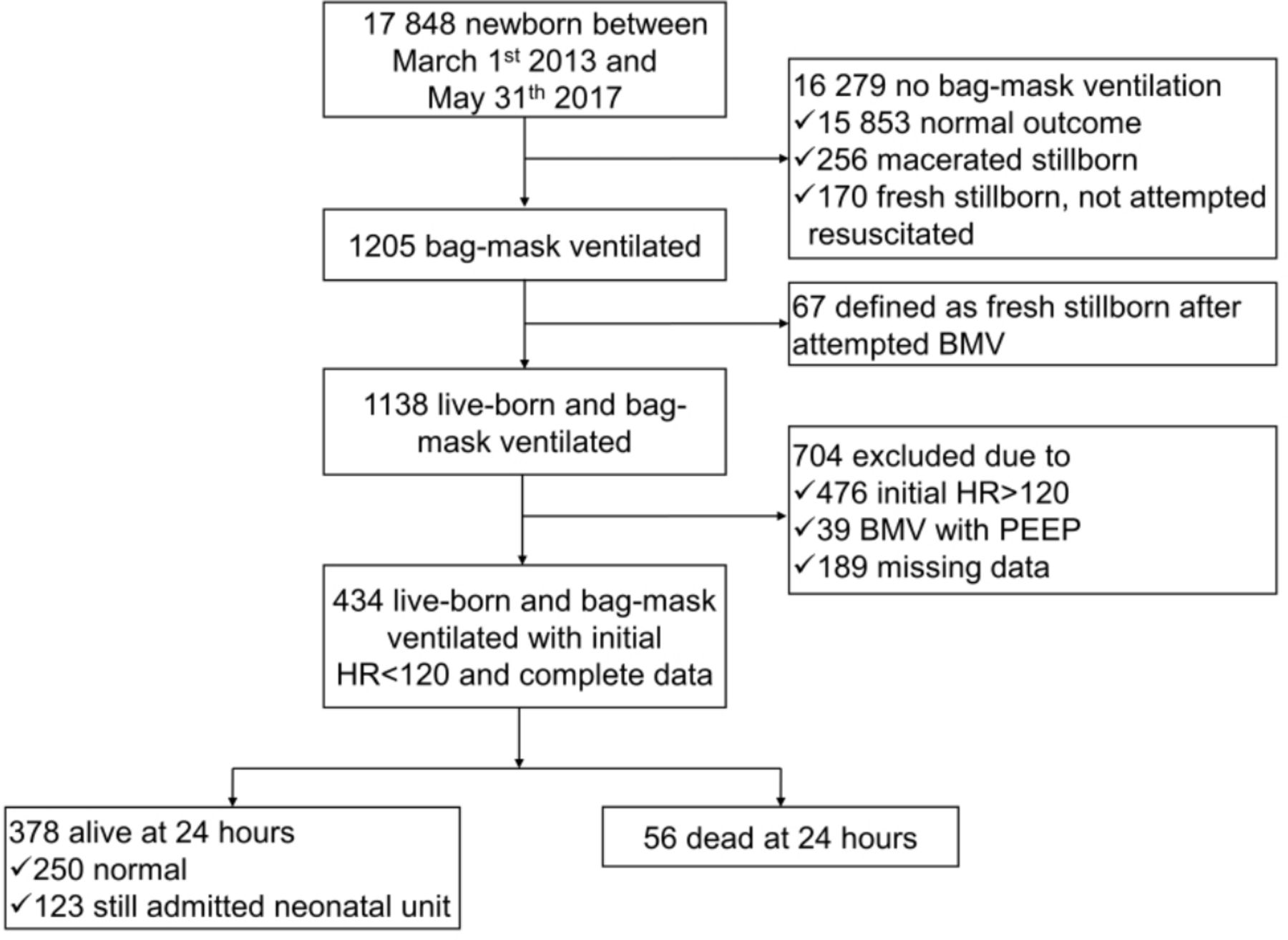
We included all live-born newborns with initial HR <120 bpm who had received BMV at birth, and had available HR, ventilation and observational data (figure 1). Our research group recently showed that normal HR is around 120 bpm in the first seconds of life.25 Low initial HR is a known risk factor for unfavourable outcome.21 Newborns who received BMV but had HR ≥120 bpm at onset of recording were excluded as these are likely different in pathophysiology and prognosis. Newborns randomised to receive BMV with positive end-expiratory pressure (PEEP) valve in a parallel intervention study were excluded due to potential impact of PEEP on ECO2.
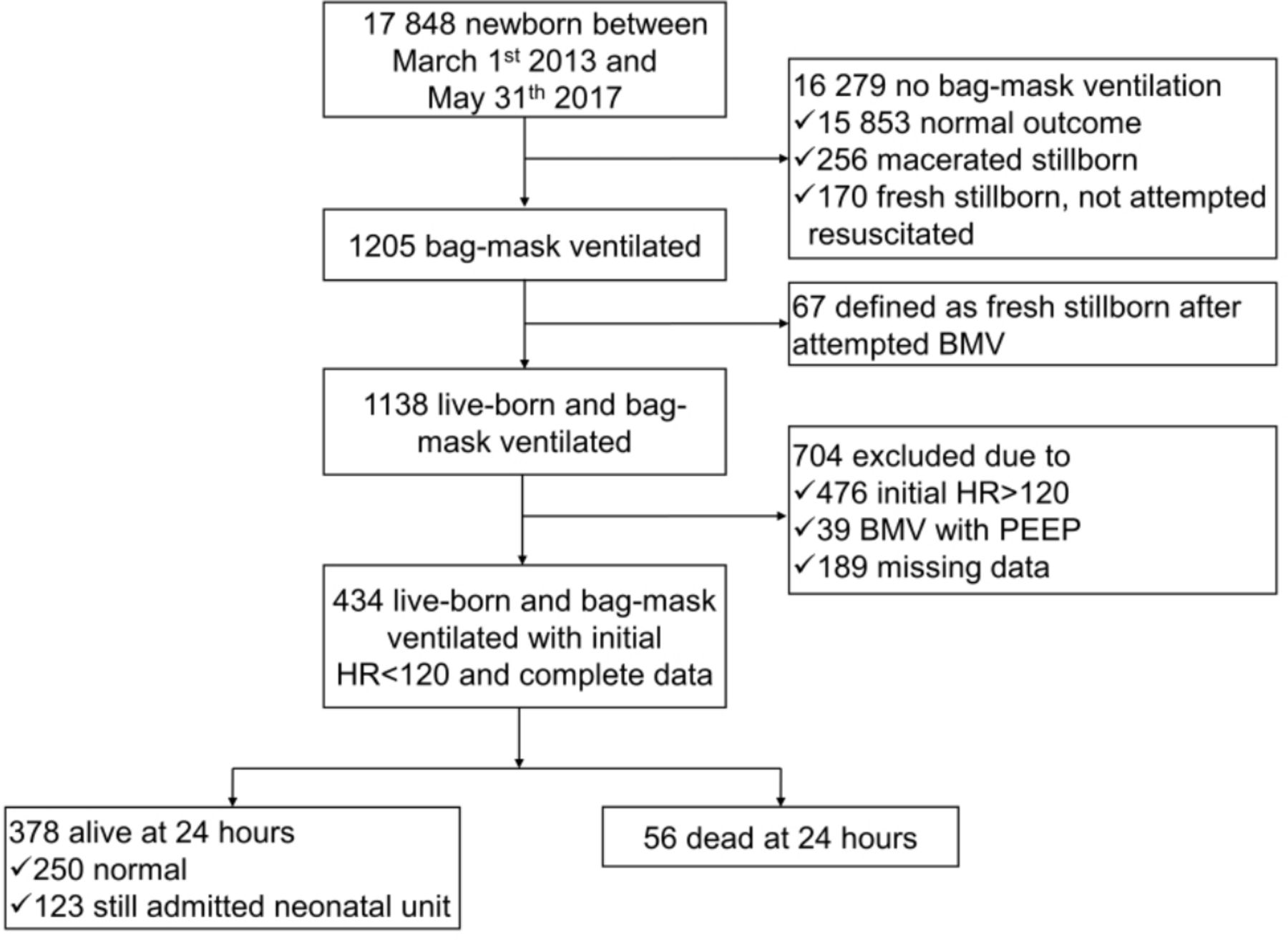
Overall newborn mortality at Haydom Hospital during the study period was 31 per thousand births. Among these, 28 were defined as still births, 13 fresh and 15 macerated. BMV, bag-mask ventilation; HR, heart rate; PEEP, positive end-expiratory pressure.
Outcome and covariates
The primary outcome was the maximum percentage of CO2 in expired air per ventilation. Secondary outcome was time to ECO2 >2% from the first BMV.
To characterise assisted ventilations (‘ventilation factors’), we used repeated measures for expired VTE, ventilation frequency, peak inflating pressure (PIP) and mask leak smoothed as means per five ventilations. The threshold to detect a ventilation was set to PIP >5 mbar.
As markers of clinical condition (‘clinical factors’), we used the initial HR and 5 min Apgar score. Initial HR was defined as the mean of the first five HR values recorded for each newborn. The 5 min Apgar score was selected due to established association with asphyxia.26 In a sensitivity analysis, we substituted Apgar score at 5 min with 1 min because 5 min score may be affected by treatment.
We also included BW and time as covariates. In the primary analyses, within the first 5 min of ventilation, time was recorded from the first detected ventilation. In the secondary analyses, per ventilation sequences, time was recorded from the first detected ventilation per sequence. We defined a ventilation sequence as continuous BMV with <5 s pause between two ventilations.
VTE >30 mL/kg were considered unlikely to be correct measurements and were excluded. We also excluded individual observations with ventilation frequency >120/min as this is twice the upper limit of recommended ventilation frequency.
Statistical analyses
For cohort and data description, we report percentages, means with SD or medians with IQRs, as appropriate (table 1). For ventilation parameters, we include intercorrelation coefficients due to variation both within and between patients.
Baseline characteristics and covariates
We fitted random intercept regression models to study changes in ECO2 by variations in clinical and ventilation factors for newborns who received BMV. Associations with ECO2 were not linear for all covariates, thus we performed log transformation for time, and included a quadratic term for VTE and PIP guided by Akaike’s information criteria and inspection of the residuals. To compare the effect of covariates measured on different scales, we report beta values per standardised units ((x−mean)/SD) in addition to the measured scale for each covariate and coefficients of determination (R2 values). R2 was calculated as the proportional reduction in prediction error variance comparing models with and without the covariate of interest.27 For closely correlated parameters, we excluded both parameters simultaneously.
The primary analysis was performed in the first 5 min of BMV. Second, we compared the effects per ventilation sequence for newborns who had three or more sequences lasting for more than 10 s to evaluate build-up effects and the impact of pauses. We used Cox regression to study predictors for time from first BMV until ECO2 reached 2% (≈2 kPa or 15 mm Hg at sea level). ECO2 threshold was set at 2% as this corresponds well with changes on the colorimetric CO2 detectors11 and the ECO2 level found to be most predictive for HR >60 bpm.28 Kruskal-Wallis test was used to compare clinical and ventilation factors in three groups of infants differing by when ECO2 >2% was achieved: never, during ventilation or spontaneously.
Data analysis was performed using Matlab (MathWorks, Natick, Masschusetts, USA) and Stata SE V.14.2 (StataCorp, College Station, Texas, USA). We used a purposeful selection approach to build regression models; only significant covariates (p<0.05) were included in the final models.
Patient and public involvement
The study was performed in an area with high illiteracy rate, and patients and public were not directly involved in the planning of the study. Oral feedback from patients and personnel were taken into account for solving practical issues concerning data collection during the study period.
Ethical considerations
All women were informed, but consent was not considered necessary by the ethical committees.
Results
During the study period, 17 484 babies were born in the hospital; 6.9% received BMV (figure 1). Among 434 included newborns, 400 had a minimum of one ventilation sequence that lasted for more than 10 s (baseline data in table 1).
Predictors of ECO2 during first 5 min
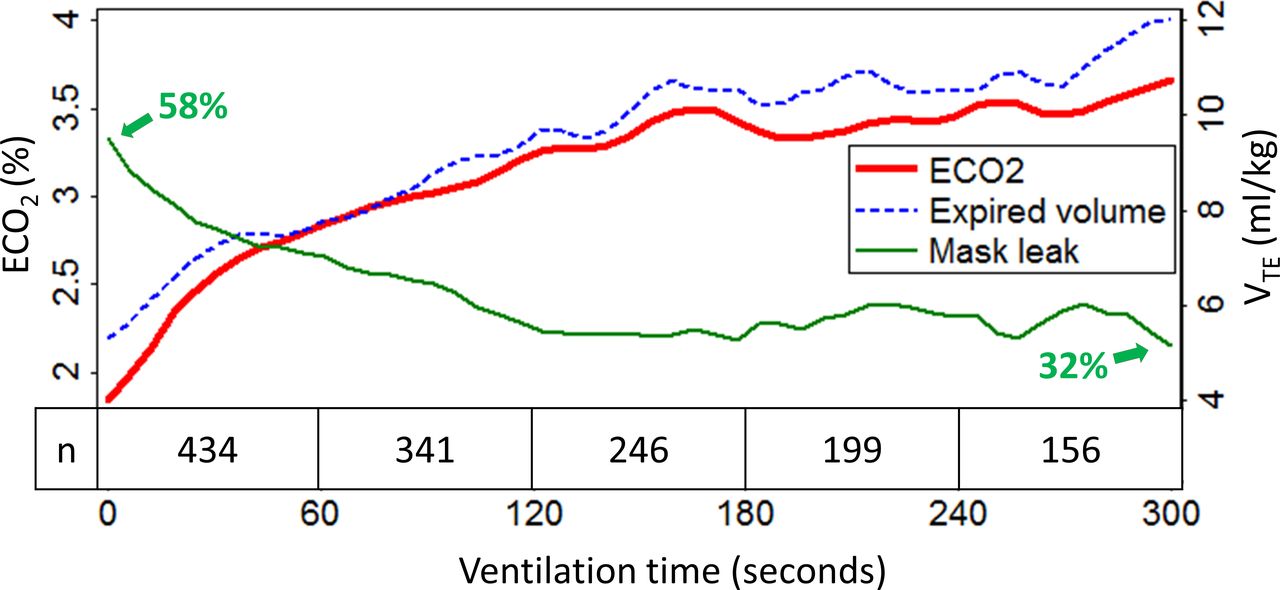
Both clinical and ventilation factors were significantly associated with ECO2, but ventilation explained substantially more of the variance than clinical factors (R2 30.8% vs 10.9%); VTE was the strongest single predictor (table 2). The association between VTE and ECO2 was positive and close to linear for VTE <10 mL/kg, levelling off at 10–20 mL/kg and negative >20 mL/kg (figure 2A). Mask leak and VTE were negatively correlated, and together explained 23% of the variance in ECO2. Low ventilation frequency around 30/min was associated with the highest ECO2 (figure 2C). PIP <15 or >60 mbar were associated with low ECO2 (figure 2D). ECO2 increased rapidly in the first minute of BMV, VTE increased and mask leak decreased simultaneously (figure 3). BW and initial HR were positively associated with ECO2 in univariate and multivariate models, 5 min Apgar score only in the multivariate model (table 2, figure 2E–G).
Linear random intercept model for predictors of expired carbon dioxide (ECO2) in the first 5 min of bag-mask ventilation

ECO2 by covariates. Smoothed local polynomial plots for predicted values of expired carbon dioxide (ECO2) per covariate in univariate (dashed, grey line) and multivariate model (solid, black line). The graphs display ECO2 versus (A) expired tidal volume (VTE, mL/kg), (B) mask leak (percentage leak), (C) ventilation frequency (ventilations per minute), (D) peak inflation pressure (PIP, mbar), (E) birth weight (kg), (F) initial heart rate (beats per minute), (G) 5 min Apgar score and (H) time (seconds). Table 2 display effect measures (beta coefficients), p values and explained variance (R2) for the regression models.
{kind=link}
{kind=link}
{kind=link}
Change in expired carbon dioxide (ECO2), expired volume and mask leak by time the figure illustrates trends for changes in ECO2 (red, solid line), VTE (blue, dashed line) and mask leak (green, dashed line) by time. The graphs are smoothed local polynomial plots. The integrated table displays the number of newborns (n) who received ventilations in each minute since start of ventilations.
Predictors for ECO2 by ventilation sequence
Analysing the first three ventilation sequences with duration >10 s (online supplementary appendix table S1 A–C) gave similar results as the primary analysis, with VTE as the strongest predictor. ECO2 increased significantly with time in the first two ventilation sequences, but not in the third (online supplementary appendix figure S1).
Supplemental material
Predictors for time to reach threshold
The Cox model found higher VTE up to 14 mL/kg to be associated with shorter time to reach ECO2 >2% (table 3). Higher 5 min Apgar score, initial HR, BW and PIP were also associated with shorter time to reach ECO2 >2%.
Cox regression for time to ECO2 >2% (n=321)*
Interactions and stratified analyses
In the primary analysis, we found a significant interaction for VTE and frequency. We found no relevant differences stratified by BW ≥2500 g versus <2500 g, initial HR ≥60 versus <60 bpm, vaginal delivery versus Caesarean section or for newborns ventilated within versus after 60 s from birth (data not shown). Substituting VTE and ventilation frequency with respiratory minute volume, we found a non-linear positive association between ECO2 and minute volumes (online supplementary appendix table S2). Substituting 5 min Apgar scores with 1 min scores did not affect the main conclusions.
Other analyses
Table 4 groups included newborns in three: (A) ECO2 >2% at onset of BMV, (B) reached ECO2 >2% during BMV and (C) never reached ECO2 >2%. Group A had significantly higher BW, Apgar scores and VTE and lower mask leak and ventilation rate in the first 30 s of ventilations compared with groups B and C. We found no significant differences in the clinical parameters between group B and C. However, infants in group C were ventilated with higher frequencies, had more mask leak and had lower VTE in the first 30 s of BMV.
Comparison of groups by time to threshold ECO2 >2%
Discussion
In this large observational study, ventilation factors were stronger predictors for ECO2 than clinical markers of asphyxia during initial resuscitation of term and near-term newborns. VTE >10 mL/kg, low mask leak and a ventilation frequency around 30/min were associated with the highest ECO2.
Simultaneous collection of ventilation parameters and observation of clinical factors in a large sample of newborns allowed for analyses considering both clinical differences and quality of delivered ventilations. The main findings were replicated in alternative statistical models. The major burden of death and morbidity due to neonatal asphyxia occurs in low-income countries.29 Even if the midwives’ ventilation skills may not be representative for all places, the physiological factors affecting ventilation parameters and ECO2 must be expected to be similar for newborns all over the world. High baseline morbidity is more likely to strengthen than hide associations with clinical factors. We do not find obvious reasons limiting the validity of the main findings in a global context.
As in any observational study, our results may be affected by unmeasured or residual confounding. It is likely that subtle interactions occurred between clinical and ventilation factors due to variations in lung compliance and muscle tone. The first detected HR defined as ‘initial HR’ was collected with variable delay after birth depending on when the HR sensor was applied. Apgar scores are subjective measures, and interobserver variability large.26 30 Measures of umbilical artery pH, base excess or lactate are more objective to assess degree of asphyxia, but were not available at the study site.
We propose that ventilation characteristics associated with higher and a faster increase in ECO2 during initial BMV are favourable to quickly establish effective gas exchange. The observed close association between VTE and ECO2 supports studies pointing to ECO2 as an indicator of lung aeration immediately after birth.5 6 An increase in ECO2 with increasing minute volumes, different from later in life, further strengthens the theory that ECO2 is diffusion limited during initial ventilation of fluid-filled newborn lungs.31 As we observed an increase in ECO2 for VTE 10–20 mL/kg, and shorter time to reach ECO2 >2% up to 14 mL/kg, we speculate that higher VTE than the commonly recommended 4–8 mL/kg may promote a faster lung aeration. Two other studies from our group found a positive relationship between delivered VTE and HR, with the most rapid increase in HR during BMV at volumes around 10 mL/kg.4 17 Larger VTE may be needed during BMV than in intubated patients to compensate for upper airway distension.32
We found that ventilation frequency was negatively associated with ECO2, suggesting less effective lung aeration at high frequencies. Highest observed ECO2 at ventilation frequencies around 30/min points to inflation rates in the lower range of recommended values as potentially more favourable, as suggested by the European resuscitation guidelines.19 20
Several authors have proposed that capnography may serve as feedback to identify airway obstruction during newborn resuscitation.10 13 33 Our findings partly support this. Low ECO2 associated with high PIP may be due to obstructed airway or low lung compliance. Mask leak and PIP effects were substantially reduced in our models when adjusting for VTE, likely because they mainly worked through VTE modifications. We do not see obvious ways to discriminate between airway obstruction and liquid-filled lungs as explanation for low ECO2 before higher levels have been observed.34 Stronger positive linear association between PIP and ECO2 in the first ventilation sequence compared with later sequences supports a need for higher opening pressure during initial inflations.35
We observed a fast ECO2 increase in the first minute of ventilation. This is line with previous studies indicating a gradual lung aeration.7–9 Efforts to improve ventilation, like clearing the airway and reducing mask leak, probably contributed to ECO2 increase over time. Reduced ECO2 after ventilation pauses suggests re-entry of lung liquid and supports a recommendation for continuous, effective ventilation to non-breathing newborns.18
The process of lung aeration has been found to be slower during BMV than in spontaneously breathing newborns.8 9 36 37 Newborns with gasping or spontaneous breaths before initiation of BMV have already started the lung-aeration process. This may explain higher initial ECO2 in newborns with higher Apgar scores. Moreover, larger newborns may have higher respiratory drive and better reserves to handle complications during labour despite low initial HR and low Apgar scores, explaining the positive association between ECO2 and BW.
Significant but weak negative associations found between Apgar scores, initial HR and ECO2 underline that severely compromised circulation may cause persistently low ECO2.16 28 Waste of valuable time trying to improve correctly performed ventilations based on ECO2 feedback may be a pitfall. To measure VTE in combination with ECO2 may reduce this risk.36 38
Our findings indicate that somewhat higher VTE than currently recommended and a low ventilation frequency may be favourable during bag-mask ventilation of term and near-term infants at birth. However, this is an observational study and long-term outcomes have not been studied. Near-term newborns have more mature and less vulnerable lungs than premature infants, and asphyxia is often the cause when they do not start breathing spontaneously.39 Still, the optimal VTE needed to balance fast establishment of adequate ventilation to avoid brain damage against the risk for lung injury remains unclear.6 40 Our findings alone are not sufficiently strong to change guideline recommendations, but may provide background information for future randomised studies of VTE, ventilation frequency and the use of ECO2 feedback during newborn resuscitation.
Conclusions
Ventilation factors are important predictors for ECO2 during the first minutes of bag-mask ventilation in newborn resuscitation. VTE of 10–14 mL/kg and ventilation frequency around 30/min are associated with the highest ECO2 and the shortest time to reach ECO2 >2%. Low ECO2 may be useful to detect inefficient ventilation. Low BW, HR and Apgar scores are also associated with low ECO2, and this must be accounted for in the interpretation.
Acknowledgments
We are deeply grateful to all midwives, research assistants, research nurses and other personell at Haydom Lutheran Hospital—and the participants, mothers and children—for making the Safer Births project possible. We also want to thank Professor emeritus Petter Andreas Steen at the University of Oslo who provided valuable advice and critical review of the manuscript.
References
Footnotes
Correction notice This article has been corrected since it was published.
Contributors KH, KS, HLE and JE had full access to all the data in the study, and take responsibility for the integrity of the data and the accuracy of the data analysis. HK, KS, JE and CK designed the study protocol. JE, JL, SJ, HK, JE and MT practically implemented, supervised and carried out the study and the data collection on site. JE gave technical support, extracted and processed the data. RH, KS, RH and JE performed the statistical analyses. KH drafted the initial manuscript. All authors have reviewed and approved the final manuscript as submitted.
Funding The study was partly funded by the Global Health and Vaccines Research (GLOBVAC) programme at the Research Council of Norway (project no. 2280203), Laerdal Global Health and the Laerdal Foundation. KH received a PhD grant from Helse Sør-Øst, Norway. MT and JL received unrestricted PhD grants from the Laerdal Foundation. KS is supported by an unrestricted grant from Oak Foundation, Geneva.
Disclaimer The funding sources had no role in the design and conduct of the study, collection, management, analysis and interpretation of the data, preparation, review or approval of the manuscript, and the decision to submit the manuscript for publication.
Competing interests JE is an employee of Laerdal Medical. JL is married to an employee at Laerdal Global Health.
Patient consent for publication Not required.
Ethics approval Ethical approval was granted by the National Institute for Medical Research in Tanzania (Ref. NIMR/HQ/R.8a/Vol.IX/1434) and the Regional Committee for Medical and Health Research Ethics for Western Norway (Ref. 2013/110).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.