Article Text

Abstract
Introduction Children with congenital heart disease have complex medical and neurodevelopmental needs. We aimed to develop a multi-professional consensus-based referral pathway applicable to action the results of the brief developmental assessment (BDA), a validated early recognition tool, that categorises the neurodevelopmental status as green (appropriate for age), amber (equivocal) or red (delayed) in children aged between 4 months and 5 years.
Methods A Delphi consensus survey detailing two scenarios—a child categorised as delayed (red) and another as equivocal (amber) on administration of the BDA at the time of discharge from the tertiary centre—was sent to 80 expert professionals from primary, secondary and tertiary care seeking agreement on next steps and referral pathways. An iterative process was proposed with a pre-defined rule of 75% for consensus.
Results The survey was completed by 77 Delphi panel experts in Round 1, 73 in Round 2 and 70 in Round 3. Consensus was achieved (1) for the child with amber or red BDA, the child should be under the care of a paediatrician with expertise in cardiology (PEC) (or general paediatrician if no PEC) based at their local hospital, (2) for the child with red BDA, the PEC should initiate referral to community services at first assessment, (3) for child with amber BDA, a re-assessment by the health visitor should occur within 1–2 months, with referral to community services and notification to the PEC if on-going concerns.
Conclusions The Delphi process enabled a consensus to be reached between health professionals on referral pathways for specialist neurodevelopmental assessment/treatment for children with heart disease, in response to amber or red BDA results. The agreed referral pathway, if implemented, could underpin a national guideline to address and intervene on the neurodevelopmental difficulties in children with heart disease.
- cardiology
- comm child health
- general paediatrics
- neurodevelopment
- multidisciplinary team-care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Children with congenital heart disease (CHD) have complex medical and neurodevelopmental needs with neurodevelopmental abnormalities leading to potentially devastating long-term sequelae.
Routine neurodevelopmental surveillance, screening and evaluation in children with CHD is well-established in cardiothoracic programmes in USA and parts of Europe unlike in UK.
An early recognition tool leading to intervention is an important first step in identifying children with delayed development in a high-volume cardiology service.
What this study adds?
A multi-professional Delphi consensus identified referral pathways for children (4 months-5 years) with congenital heart disease (CHD) using early recognition tool-Brief Developmental Assessment-BDA.
Consensus that children with delayed development (red BDA) should be referred immediately and those suspected (amber) should be re-assessed before referral to community paediatricians.
The paediatrician with expertise in cardiology is central to the management of children with CHD and follow-up of suspected and/or confirmed neurodevelopmental delay.
Introduction
Children with congenital heart disease (CHD) have complex medical requirements (cardiac surgery, multiple hospitalisations, medications, associated syndromes), which may negatively impact their neurodevelopment—a key factor in their general well-being and educational attainments.1–7 Currently, there is no formalised neurodevelopmental screening or surveillance pathway for children with CHD in the UK above that offered to healthy children. Research in the USA has identified neurodevelopmental abnormalities in as many as 25% of surgical survivors1 8–17 and the American Heart Association in their scientific statement18 has outlined an algorithm for a surveillance, evaluation and management for children with CHD. In the UK, a recent consultation exercise with clinicians from primary, secondary and tertiary care and lay stakeholders as part of the National Institute for Health Research (NIHR)-funded paediatric cardiac morbidity surgery study19 ranked neurodevelopmental problems as the number one complication concern for those undergoing intervention for CHD.20 Our research indicates that there are gaps in the follow-up of children with CHD with developmental difficulties.21 While there are many screening tools, all require specialised personnel, are time-consuming, expensive and undeliverable on a wide-scale in a resource-constrained nationalised health service (NHS). Hence, within the context of this NIHR study, an innovative, easy to administer ‘early recognition tool’—brief developmental assessment (BDA)—was developed and validated in 971 children aged 4 months–5 years in three paediatric tertiary cardiac centres in London, UK.22 23 The BDA covers different age bands (17–34.9 weeks, 35–60 weeks, 15 months–2.9 years, 3.0–4.9 years) accounting for different stages of child development and covers domains of gross motor skills, fine motor skills, daily living skills, communication, socialisation and general understanding. The BDA allows categorisation of a child’s current neurodevelopment as green (appropriate for age), red (delayed) or amber (equivocal) to help direct care through early recognition, enabling children with concerns to be referred for specialist assessment/treatment. The ultimate goal is for the BDA to be used in the NHS by practitioners who are not neurodevelopmental specialists, as resources do not exist for specialist assessments to be carried out on every child with CHD.
Aim and objectives of the Delphi survey
The aim was to develop a multi-professional consensus-based protocol for actions on the application of the BDA in age groups (from 4 months to 5 years) in children with CHD in the UK. The main objectives were to (1) recruit a multidisciplinary group of health professionals from primary, secondary and tertiary healthcare caring for children with CHD and (2) seek agreement on referral pathways for managing a child with amber or red BDA result to maximise effectiveness of the BDA tool.
Methods
Recruitment and selection of the Delphi panel
We identified a multidisciplinary group of primary, secondary and tertiary healthcare professionals within the CHD networks in the UK, comprising of paediatric cardiologists, paediatric neurologists, paediatric neurodisability professionals, paediatricians with expertise in cardiology (PEC), general paediatricians, community paediatric nurses, community paediatricians, health visitors (HVs), cardiac nurse specialists, advanced nurse practitioner/nurse consultant, general practitioners (GP) and parent representatives. To ensure an adequate knowledge base, those who had been in their role for at least 2 years were invited by email giving information on the BDA and requesting participation in the Delphi panel. Those who formally agreed were sent the Delphi survey. The regions identified were London, East of England, South East, North East, East Midlands, West Midlands, South West of England, Yorkshire and Humber, Wales, Scotland, Northern Ireland and North West of England. The Delphi Consensus Survey was registered as a service improvement project and ethical approval was not required.
Study design for Delphi consensus survey
The survey was designed using SurveyMonkey software containing two scenarios, each presenting a BDA result for a child with CHD aged between 4 months and 5 years at discharge from the tertiary centre. This age bracket has been chosen as the BDA was validated in this age group.23 Alongside each scenario, respondents were sent a relevant example of the BDA along with standard information to be shared with all relevant health professionals. Scenario 1 described a child with amber BDA admitted to the tertiary centre for an intervention (surgery or catheter treatment), who is found to have developmental concerns on the BDA (score of amber=not fulfilling some of the milestones based on population norms, equivocal result). Scenario 2 described a child with red BDA admitted to the tertiary centre for an intervention (surgery or catheter treatment), who is found to have developmental concerns on the BDA (score of red=lagging behind the milestones based on population norms). The survey consisting of a mix of open questions with free-text response and specific closed questions on the two scenarios was electronically sent with a unique web link to participating professionals, who were asked to rate responses on a Likert scale: strongly disagree=1, disagree=2, moderately disagree=3, mildly disagree=4, undecided/don’t know=5, mildly agree=6, moderately agree=7, agree=8, strongly agree=9. Non-responders would be sent reminder emails to complete the survey.
Development process of the Delphi survey
A 4-step process was followed in the development of the Delphi survey. A core team—AH, KB, JW—developed the Delphi survey based on findings from two previously published studies in which the BDA was developed22 and then validated23 (funded by NIHR Health Services and Delivery Research). This draft survey was refined by the fourth author—ML. Following this, the Delphi survey and the proposed methodology were reviewed by an independent expert on Delphi methodology, which led to further refinements. The final step was pilot use of the survey with two paediatricians, leading to further minor modification based on their feedback.
Data analysis
The results were grouped as: agree—if the level of agreement was 7, 8, 9; middle ground—if the level of agreement was 4, 5, or 6; and disagree—if the level of disagreement was 1, 2 or 3 to facilitate identification of areas of agreement or disagreement or middle ground with the main goal of reaching a consensus. This methodology has been well described in several widely used paediatric guidelines in the UK.24–26 Free-text responses were categorised and analysed as follows: in line with the Delphi methodology,27 three of the authors—AH, KB, JW—independently looked at all of the comments and identified the key themes. These themes were then discussed by the authors, and were then collated, summarised and synthesised to inform the next round of questions. Comments from the participants were also used to provide additional context for the findings.
Definition of consensus
We established an a priori criterion of 75% approval to define consensus—75% of the panellists selecting 7, 8 or 9 of the 9-point Likert scale. Any questions or statements with (1) clear disagreement or (2) middle ground (no clear agreement or disagreement) would be revised and re-sent on a subsequent Delphi round until consensus was reached. The results would be sent with each iterative round.
In accordance with current national healthcare provisions, we stated a presumption that there would be a PEC in most district general hospitals, and if not, the default would be a general paediatrician. We also presumed that children<5 years of age will have a HV in their local community.
Patient and public involvement
Lay stakeholders including parents were consulted along with clinicians from primary, secondary and tertiary care as part of the National Institute for Health Research-funded paediatric cardiac morbidity surgery study19 and they ranked neurodevelopmental problems as the number one complication concern for those undergoing intervention for congenital heart disease20. Parent representatives and other stakeholders have been involved with the design, conduct and dissemination at every stage of the project.
Results
Of the 164 invited professionals across the UK, 87 (53%) agreed to participate (table 1). The geographical distribution was weighted towards South East of England (table 2). There were no differences in professional background or geographical location between participants and non-participants. All panellists were experienced with >5 years of experience in their specialty, at the time of completing the survey, 53 (66%) had been in the role within their current organisation for >5 years, while the rest were in the role for 2–5 years.
Professionals who participated in the Delphi consensus rounds
Distribution of Delphi panel experts
Round 1
(online Supplementary material)The results of Round 1 are outlined in table 3. The respondents supported their choice by giving open text comments. Selected pertinent comments and themes that emerged were as follows:
Supplemental material
Delphi consensus survey—results from round 1
Amber BDA scenario: (1) the tertiary cardiac team who has administered and identified the amber BDA will be aware of the child’s GP and PEC, but will not be familiar with the community paediatric services in the child’s local area, (2) the GP needs to be the health professional initiating new referrals, because referrals may not be accepted if made by one consultant to another (ie, bypassing the GP), (3) the PEC or general paediatrician may not be equipped to assess child development and hence undertake re-assessment, and (4) there were contradictory comments about the HV skills (positive from secondary/primary care) and comments that cardiac professionals may have limited understanding of the HV service.
Red BDA scenario: there was no consensus on which health professional should be undertaking the referral to the community paediatrician which necessitated a second Delphi round. Respondents cautioned against referral delays and suggested that ‘it did not matter who made the referral as long as it happened’ online supplementary material.
Round 2
The results of Round 2 are outlined in table 4. For amber BDA scenario: the required level of consensus of 75% was not reached on (1) referral by HV to PEC and (2) whether the child should be re-assessed before referral to the community paediatrician, resulting in a third Delphi round.
Delphi consensus survey—results from rounds 2 and 3
For red BDA scenario: the panel agreed that referral with red BDA result should be made by the PEC to the community paediatrician (82%). The Delphi panellists commented that (1) there should be robust communication between primary, secondary and tertiary professionals, (2) delays in referral communication and multiple referral/appointments should be avoided and (3) referral to community services should be prompt online supplementary material.
Supplemental material
Round 3
For amber BDA scenario, the panel agreed that if the HV had concerns in the 1–2 month assessment after discharge from the tertiary centre, the HV should refer to the community paediatrician (with notification to the PEC); however, only 73% of the panel agreed that the child should be re-assessed by the HV 1–2 months after discharge (table 4). On analysing the free text comments, it appears that the response was influenced by the perception that (1) there is significant variation in HV service within the UK, (2) HV service is overburdened and (3) children who have started school (at 4 years) may no longer be under HV in some areas. Of note, all the HVs/GPs in the panel agreed that re-assessment should be undertaken by the HV online supplementary material.
Supplemental material
The results from 3 Delphi rounds are summarised in table 5.
Delphi consensus survey—summary of results from rounds 1, 2 and 3
Discussion
Neurodevelopmental difficulties can potentially be the most devastating long-term sequelae for children with CHD28–30 and as the number of survivors with complex cardiac conditions increase, there is a growing demand for these children to have adequate support within the wider healthcare system. Routine formal neurodevelopmental testing can be difficult to enforce within the constraints of the NHS. The validated BDA would theoretically function as an early recognition tool to sign-post those children with CHD who have neurodevelopmental problems. However, implementation of such a tool serves no useful purpose unless intervention and referral pathways are established. Using the Delphi consensus process with iterative rounds and feedback loops, with a panel comprising experts from primary, secondary and tertiary care within different parts of the UK, our study showed that consensus on referral patterns can be established for children with CHD who have been identified to have neurodevelopmental concerns by the BDA.
Consensus
The Delphi expert panel reached consensus that: children with either amber or red BDA should be under the care of the PEC and referred at the time of discharge from the tertiary centre by the child’s primary cardiologist with results shared with the GP, HV, cardiologist and other relevant health professionals (figure 1). Children with a red BDA should be referred to a community paediatrician and local child development team (if not already under one) at the time of the assessment to minimise any delay. Children with an amber BDA should have a re-assessment by the local HV 1–2 months after discharge and be referred to the community paediatrician if there are persisting concerns, with a notification to the PEC. The PEC or designated paediatrician at the local hospital and the HV (in the case of younger babies and toddlers) were identified as the key health professionals in an ideal position to link up a child with CHD with developmental problems and their local child development team. In addition, the PEC was identified as an important link with the tertiary cardiac centre. Of note, the Delphi responses did not support a new referral to the PEC/paediatrician coming from the specialist nursing team in the tertiary hospitals.
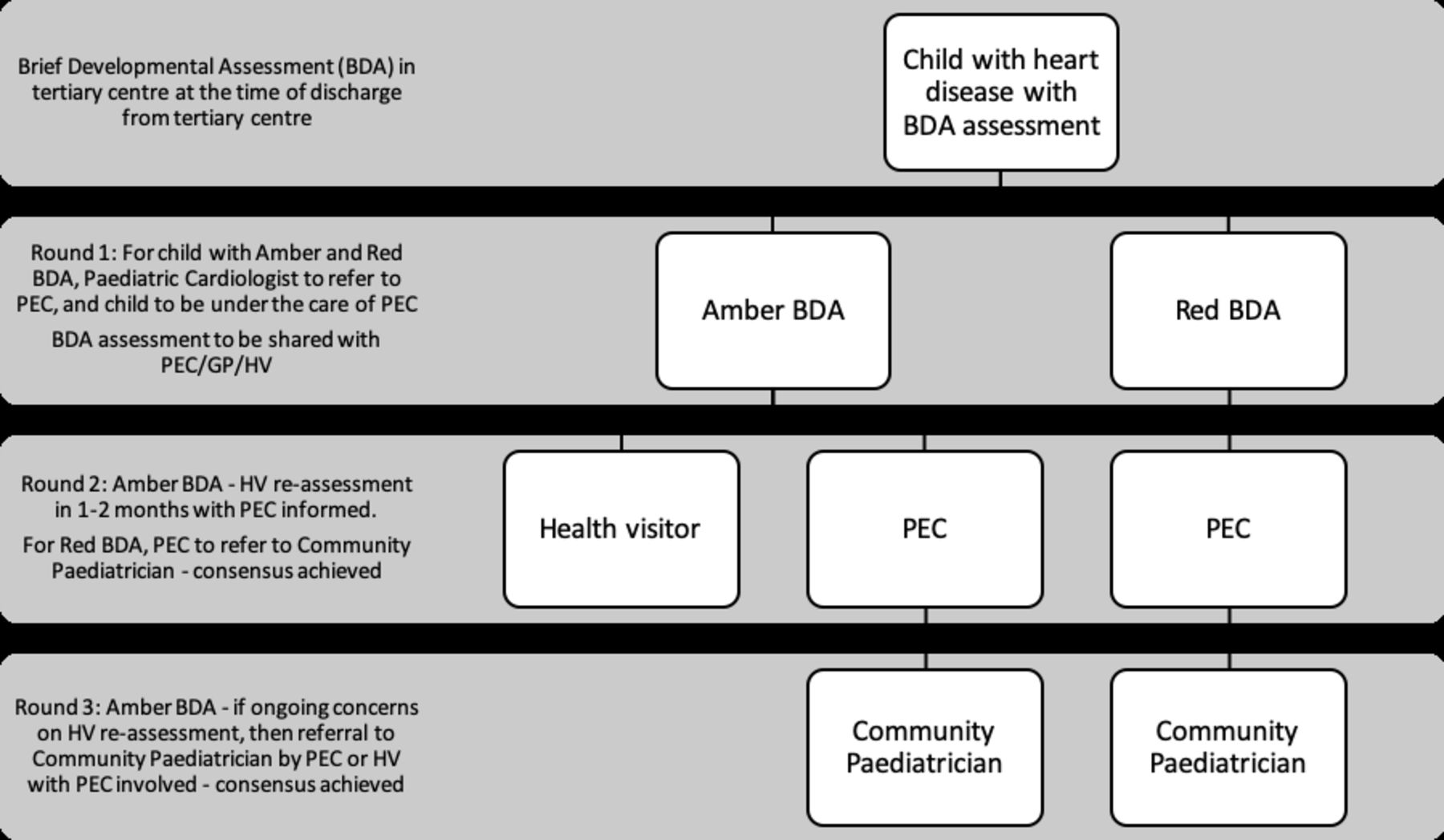
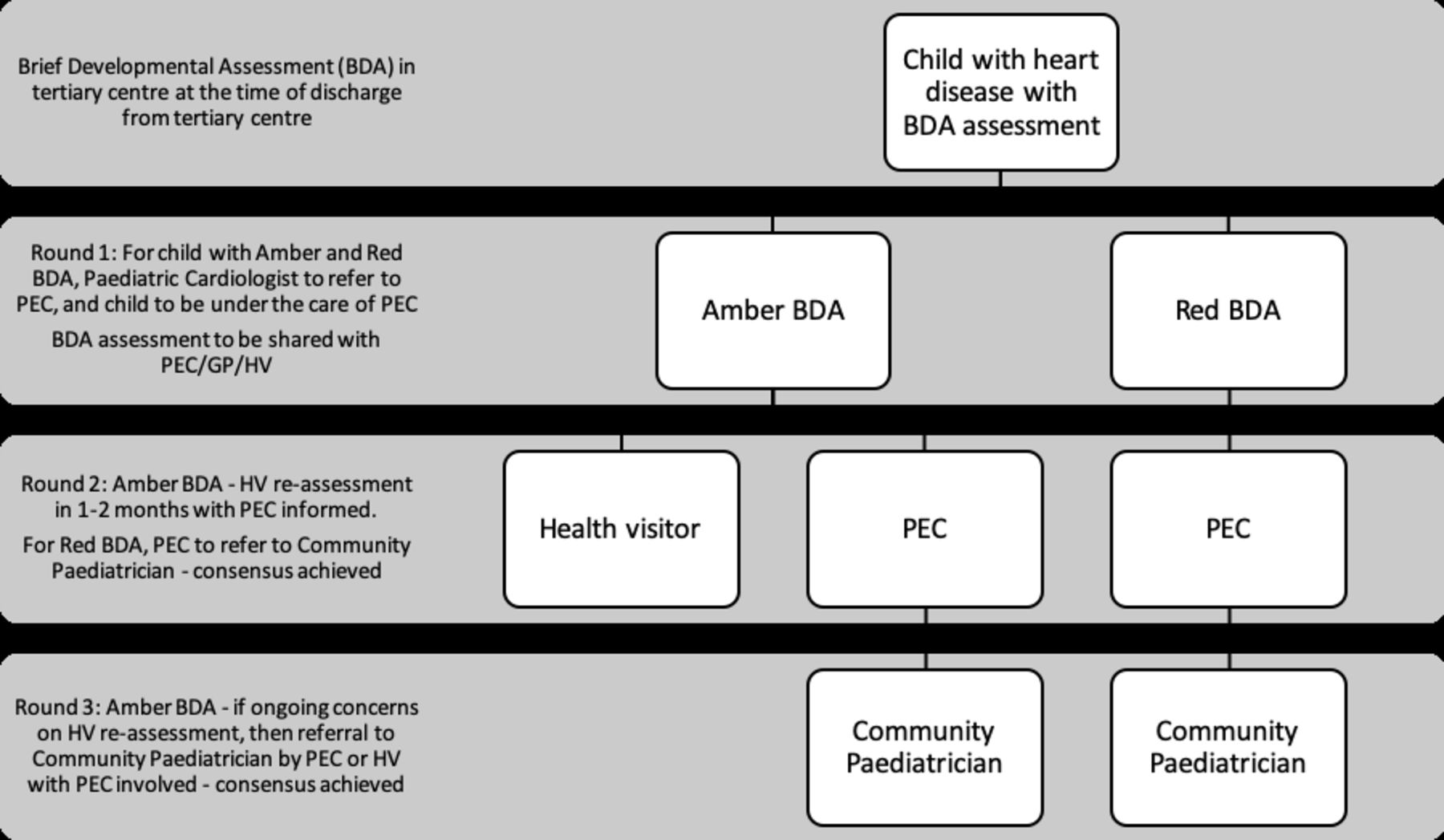{kind=link}
Delphi consensus for referral pathway for child with heart disease who has neurodevelopmental concerns—amber or red BDA—at discharge from tertiary centre. The consensus for referral pathway for amber or red BDA agreed from the iterative rounds of the Delphi consensus process is shown in the figure. For the child with amber BDA, this may need to be locally/regionally defined and adapted to local resource availability. BDA, brief developmental assessment; GP, general practitioner; HV, health visitor; PEC, paediatricians with expertise in cardiology.
Healthcare across sectors
As a background to this consensus process, it is important to acknowledge the current care provision relevant to developmental needs for children with CHD, although this can be highly variable.
Tertiary care: Children with CHD are always under a cardiologist and a cardiac specialist nursing team, who may not necessarily have ‘general paediatric’ and ‘child development’ expertise but assess the child at critical time points particularly in early infancy. The BDA is intended for use as an early recognition tool for child neurodevelopment in this setting.
Secondary care: Within the setting of a non-specialist hospital, children with CHD are under the care of a PEC. In a small number of hospitals where a PEC is not in post, a named paediatrician will have designated responsibility for the paediatric needs of cardiac children. Not all cardiac children are formally under the care of a PEC or paediatrician (eg if they have never been to the local hospital); however a PEC or paediatrician with designated responsibility is available for a cardiac child should the need arise. The PEC (unlike the tertiary hospital team) will be aware of child development services available locally.
Primary and community care: all children, including those with CHD, are under a GP and at pre-school age, a HV. Both GP and HV are experienced in the referral of children with possible developmental problems to child development teams and will be cognisant of the local services. It is well known that HV services are under pressure, with recent reports indicating that many children miss out on these visits.31–33 Child development teams are based within individual areas that they serve and are often linked to specific non-specialist hospitals. A child with CHD will be under the care of a child development team only if specifically referred.
Areas where agreement was more challenging
The main area where there was lack of agreement related to the child with an amber BDA. Of note, a child with suspected developmental delays may benefit from close follow-up and re-assessment given that these are crucial to identify the need for early intervention. Early identification and timely intervention contribute significantly towards a child’s overall adjustment and quality of life.34 There was moderate support for HV re-assessment, PEC re-assessment and referral to community paediatrics if on-going concerns with the child’s development, but the consensus for re-assessment by the HV fell slightly short (73%) of the required 75% level for agreement. However, despite being in the minority in the panel, all the primary care representatives (HVs included) agreed that the child with amber BDA should have a re-assessment by the HV, and this response pattern was similar to that of the secondary and tertiary professionals. While there was no agreement for a child with amber BDA to be under the care of the community paediatrician, there were also conflicting opinions over whether or not the PEC or paediatrician is equipped to assess child development and hence undertake the recommended re-assessment. This may reflect lack of clarity between health professionals from different sectors as to each others roles and skills. In addition, the initial lack of consensus about who should make the referral to the community paediatrician in the case of a child with a red BDA may reflect the lack of familiarity with the way local services operated across sectors. Furthermore, bearing in mind that there are significant regional and sub-regional variations in the delivery of healthcare, the process for the re-assessment of a child with amber BDA needs to be locally/regionally defined, and adapted to local resource availability. A particular hallmark of child development in those with CHD is that this is an issue that spans sectors and hence may fall through the gaps, and the responses of the Delphi survey were consistent with this, although eventually reaching consensus as to responsibilities for each sector/professional group.
Strengths and Limitations
This is the first time a consensus has been developed using the Delphi process to outline referral pathways for potentially abnormal neurodevelopment from a group of primary, secondary and tertiary care professionals looking after children with CHD. The Delphi process does not involve any face-to-face contact unlike a consensus development conference or a structured discussion. While every attempt was made to enrol experts into the Delphi panel from primary healthcare, there were few GPs and HVs who accepted the invitation. While every attempt was made to enrol experts into the Delphi panel from primary healthcare, there were few GPs and HVs who accepted the invitation. Despite this, the pattern of responses was similar across the groups. Furthermore, utilising only two virtual scenarios—one example each of amber and red BDA—may have limited the generalisability of the survey, and offering more scenarios may have generated a heterogeneous response but achieving consensus may have been difficult, and may have negatively impacted on the response rate.
Conclusions
The Delphi process has provided the initial platform for developing consensus on a national pathway for the management of children with CHD who have either equivocal or delayed neurodevelopment. The consensus supported the vital role of the PEC as a coordinating link between the primary cardiologist and the community services. The HV as a close link to community services in liaison with the PEC was felt to be the point of contact for re-assessment of the child with borderline or equivocal results. Having developed and validated the BDA as an early recognition tool, and having established consensus for the referral pathway within primary, secondary and tertiary care sectors for a child with suspected neurodevelopmental problems based on the BDA results, the next step will be a formal healthcare evaluation of the BDA. It is hoped that referral of children in accordance of the consensus reached in this study will ensure earlier identification of neurodevelopmental problems and timely interventions to address neurodevelopmental deficits.
Acknowledgments
We would like to acknowledge Ms Jana Gurasashvili for the administrative help with the study, Dr Roz Ullman, Senior researcher, Riches & Ullman LLP as the independent expert in Delphi methodology for her help in the initial development of the survey and all the Delphi panellists for their participation in the iterative rounds and the support from the NIHR Great Ormond Street Hospital Biomedical Research Centre, Great Ormond Street Institute of Child Health, Great Ormond Street Hospital NHS Trust, University College London, London.
References
Footnotes
Twitter @aparnahoskote
Contributors Conceptualisation and study design: AH, JW, KB and ML. Administration of the survey and drafting of survey questions for the iterative rounds of Delphi: AH, JW, KB and ML. Analyses of the study data: VB, AH, JW, KB and ML. Write-up: AH, JW, KB and ML Editing and final approval of the final manuscript: AH, JW, VB, KB and ML.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.