Article Text

Abstract
Background There is limited knowledge about the prevalence and stability of insomnia defined by the Diagnostic and Statistical Manual of Mental Disorders (DSM). We therefore provide such estimates from preschool to early adolescence and explore potential sex differences.
Methods We followed a representative community sample (n=1037) biennially from 4 to 14 years of age (2007–2017). Insomnia diagnoses and symptoms were captured by a semistructured clinical interview of parents and children (from age 8 years).
Results At ages 4 and 6 years approximately 2.5% of children met the criteria for insomnia, whereas at ages 8, 10, 12 and 14 years the prevalence ranged from 7.5% to 12.3%. During the 10-year period examined nearly 1 in 5 children had insomnia at least once (18.7%). Sex differences were apparent with DSM-IV, but not DSM-5, criteria: boys (8.1%) had more insomnia than girls (4.5%) did at ages 4–10 years, whereas girls (11.4%) had more insomnia than boys (7.1%) did at ages 12 and 14 years. Insomnia proved stable, with 22.9%–40.1% of children retaining their diagnosis 2 years later. Having current insomnia produced medium to large ORs of between 5.1 (95% CI 2.6 to 9.8) and 15.3 (95% CI 4.4 to 52.9) for subsequent insomnia 2 years later compared with not having preceding insomnia.
Conclusions Insomnia was less prevalent than previous research indicates, with nearly 1 in 5 participants having insomnia at least once between the ages of 4 and 14 years. Female preponderance emerged in early adolescence. Having insomnia at one time point was a considerable risk for subsequent insomnia, indicating that insomnia is persistent and warrants clinical attention.
- sleep
- general paediatrics
- epidemiology
- comm child health
- child psychology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
There is a dearth of studies on the prevalence and stability of interview-based DSM-IV and DSM-5 diagnosable insomnia in childhood.
Previous work is characterised by differing estimates depending on the definition of sleep difficulties (eg, from problems to disorders) and methodological approach (ie, time-span, informants).
In early adolescence, a female preponderance in the prevalence of insomnia is typically reported.
What this study adds?
Both DSM-IV and DSM-5-defined insomnia were less prevalent in this study than previous research indicates.
Sex differences were apparent with DSM-IV, but not DSM-5, criteria: male preponderance at ages 4-10 years and female preponderance at ages 12 and 14 years.
Insomnia was moderately to highly stable; those with current insomnia (compared with those without) were 5–15 times as likely to have subsequent insomnia.
Introduction
Childhood insomnia is associated with negative outcomes that include emotional, behavioural and cognitive problems.1–3 Prevalence estimates and a description of the course of insomnia may aid preventative and treatment efforts. However, most previous research on this topic in children has examined insomnia symptoms4–11 that may not have the severity, duration, intensity or associated impairment that warrants a clinical diagnosis. Moreover, research has almost exclusively relied on questionnaires/checklists,12–14 with various biases.15 In clinical interviews, on the other hand, the interviewer probes until it is clear whether a symptom is present or not according to diagnostic criteria.
Only three previous studies have estimated the prevalence of childhood insomnia through clinical interviews,16–18 two addressing early childhood16 17 and one reporting averaged rates for the age span 8–18 years.18 In addition, two questionnaire-based longitudinal studies have assessed insomnia into early adolescence.12 13 Hence, there is a dearth of studies on the prevalence of diagnosable insomnia from preschool to adolescence based on interview data. We will therefore provide such estimates.
If, once established, childhood insomnia evinces a chronic course, early intervention may be warranted. However, if insomnia is transient there is less need to intervene. Preschool-age insomnia has been found to increase the risk of later insomnia,17 and studies of preadolescents indicate that insomnia symptoms are moderately stable.6–8 12 13 However, these studies used questionnaires and checklists; thus, the stability reported may reflect the stability of the rater rather than of the symptoms. By using clinical interviews, as we do here, rater bias and common method biases are reduced and hence more accurate stability estimates can be obtained.
From the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV)19 to the fifth (DSM-5),20 the symptom of experiencing sleep as non-restorative has been replaced with that of early morning awakenings accompanied by the inability to return to sleep. The impact of this change on prevalence estimates and course in children is unknown but will be examined here.
Using a semistructured clinical interview in a large and representative community sample (over six waves, from age 4 to 14 years) we tested the following hypotheses: (1) the rate of insomnia will decrease from preschool to middle childhood and rise again in early adolescence; (2) insomnia is more prevalent in girls than in boys in early adolescence, as shown earlier regarding insomnia symptoms;4 18 21–23 (3) the 2-year persistence of insomnia is of medium effect size.
Methods
Procedure and participants
Data came from the Trondheim Early Secure Study (TESS).24 All children born in 2003 and 2004 in Trondheim (n=3456), Norway, were invited to participate through a letter of invitation ahead of an ordinary community health check-up at the age of 4 years. Health nurses informed parent(s) about the study and obtained written consents to participate (82.2% of those invited). Included in the letter of invitation was the Strengths and Difficulties Questionnaire (SDQ) for 4–16 year-olds,25 which the parents completed and brought with them to the check-up. The SDQ has proven to be an excellent tool in screening for mental health problems in preschoolers.26 To increase variability and thus statistical power, children with mental health problems were oversampled. Children were divided into four strata based on their SDQ score: 0–4, 5–8, 9–11 and 12–40. The probability of being selected increased with increased SDQ scores (37%, 48%, 70% and 89% from the respective strata). Parents with insufficient proficiency in Norwegian to fill out the SDQ were excluded (n=176) and 166 parents were missed being asked to participate in the study. Of the 2477 eligible families, 1250 were drawn and invited (three children with SDQ score >25), 997 (79.7%) attended at baseline. Details of procedure and participation rates are presented in online supplementary eFigure 1. Mean age in years at initial testing (T1, descriptive statistics in online supplementary eTable 1) was Mage=4.59, SD=0.25, and at subsequent assessments was as follows: T2: Mage=6.72, SD=0.19; T3: Mage=8.79, SD=0.23; T4: Mage=10.51, SD=0.17; T5: Mage=12.50, SD=0.14; T6: Mage=14.35, SD=0.16. In all, we had diagnostic information on at least one time point for 1037 participants, thus forming the analytical sample. To examine attrition at each time point, attrition (ie, not attending) was regressed on every study variable on the preceding time points. None of the study variables predicted attrition, except that boys had higher attrition at 10 (OR=1.39, 95% CI 1.07 to 1.81), 12 (OR=1.31, 95% CI 1.01 to 1.69) and 14 years of age (OR=1.40, 95% CI 1.09 to 1.80). The proxy R2 values for sex were all <1%.
Supplemental material
Supplemental material
Participant and public involvement
The planning, implementation, carry through and dissemination from TESS is guided by a user group consisting of participating adolescents and parents, researchers from TESS, St Olavs Hospital, the municipal education officer in Trondheim, the youth division of the user group Mental Health Norway and Department of Education—Trøndelag county. Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Measures
At ages 4 and 6 years, DSM-IV-defined insomnia was measured by the Preschool Age Psychiatric Assessment (PAPA),27 a parent interview that follows a structured protocol. PAPA is a revised version of the Child and Adolescent Psychiatric Assessment (CAPA), which is appropriate for older children and hence was used in this study when the children were 8, 10, 12 and 14 years of age.28 Children and parents were interviewed separately and the interview questions are presented in online supplementary file 3. Symptoms of insomnia were considered present if reported by either parent or child.
Supplemental material
The interviewers (n=7) had at least a bachelor’s degree in a relevant field and extensive prior experience working with children and families. Blinded raters recoded 9% of audio-recorded interviews and inter-rater reliability between multiple raters for insomnia was k=0.75.
Diagnosing insomnia
According to the DSM-IV,19 the International Classification of Sleep Disorders-3 (ICSD-3)29 and the International Classification of Diseases, 10th Revision,30 insomnia is characterised by difficulties initiating and/or maintaining sleep and/or a subjective experience of non-restorative sleep despite adequate opportunities for sleep, which lasts for a considerable amount of time and causes clinically significant distress or impairment in important areas of functioning. However, in the absence of a cut-off for the frequency or duration of insomnia symptoms, epidemiological research on insomnia has been challenging. As no child-specific insomnia criteria exist in the DSM, we relied on normative sleep latency, night awakenings and sleep duration in childhood.10 31–34 Our data allowed assessing DSM-IV insomnia from age 4 to 14 years and DSM-5 insomnia from age 10 to 14 years. From age 10 years prevalence estimates for DSM-IV and DSM-5 insomnia were analysed in parallel. DSM-IV insomnia at 4 and 6 years of age was classified as preschool insomnia, at ages 8–10 and 12–14 years as middle childhood insomnia and early adolescence insomnia, respectively.
DSM-IV insomnia
Based on these studies and the DSM-IV criteria with suggested cut-offs, we defined DSM-IV insomnia as: (1) ≥30 min to fall asleep or the use of sleep medication; (2) ≥20 min awake after sleep onset; or (3) non-restorative sleep (insufficiently rested after sleep). The symptom(s) had to have occurred at least three times a week and had to be present over the previous 3 months, as this is the inquiry period of PAPA and CAPA, and be accompanied by reports of clinically significant distress or impairment in important areas of functioning. Because CAPA probes sleep onset or night awakenings in hours rather than minutes, it should be noted that we used ≥1 hour as the cut-off at age 8 years before correcting this by expanding the insomnia interview from age 10 years onwards to include time in minutes too. Hence, data from age 8 years should be viewed as yielding a conservative, proxy insomnia measure.
DSM-5 insomnia
In recent years both the DSM-520 and the ICSD-329 have suggested cut-offs for subjective sleep latency and time awake after sleep onset of greater than 20–30 min. The DSM-5 parts with DSM-IV criteria regarding non-restorative sleep, replacing it with early morning awakening before 8 hours of sleep and being unable to return to sleep. In addition, DSM-5 acknowledges that symptoms of sleep latency and nocturnal awakenings may be masked by caregiver intervention. We therefore regarded always relying on parental help to initiate or maintain sleep as validation of these symptoms.
Statistical analyses
All analyses were performed in Mplus V.8.35 We used a full information maximum likelihood approach to handle missing data,36 which uses all available data to estimate the most likely values for the population parameters in the model. As the sample was screen stratified, probability weights where the number of children in the stratum was divided by the number of participants in the same stratum were calculated to arrive at corrected population estimates. A robust maximum likelihood estimator was used, which is robust to deviations from normality because it provides corrected error terms with respect to oversampling. Some categorical variables served as both predictor and outcome (eg, insomnia at ages 6, 8, 10 and 12 years). Because Mplus cannot specify an endogenous variable as categorical, we performed bivariate regressions to assess the stability of insomnia (eg, insomnia at age 6 years was regressed on insomnia at age 4 years). To investigate both the sex differences in the prevalence of insomnia at each time point and the stability between time points, we compared a model in which prevalence/stability was constrained to be equal in the two sexes with another model in which prevalence was freely estimated, using Wald tests. Supplementary analyses were performed to investigate the growth of parent and child reports of insomnia over time. We did latent linear growth curve analyses where the slopes reflected yearly mean change (Mgrowth) in insomnia prevalence (%). The growth was allowed to correlate with the intercept, set at age 4 and 8 years for parent and child analysis, respectively. Further, we analysed sex differences in insomnia symptoms to elucidate any sex differences found at disorder level.
Results
Prevalence
Table 1 presents the prevalence, incidence and recurrence of DSM-IV and DSM-5-defined insomnia at all ages. The prevalence of insomnia increased sharply from 6 to 8 years. However, bear in mind that children were not included as informants before the age of 8 years and separate growth curve analyses for parents (Mgrowth=−0.05, p=0.56) and children (Mgrowth=0.13, p=0.49) showed no increase in insomnia prevalence with age. Thus, the increase from age 8 years onwards might be due to having two sets of informants, as opposed to only the parents as informants at earlier ages. Close to every fifth child had DSM-IV insomnia at one point between 4 and 14 years of age (18.7%, 95% CI 16.2 to 21.2); 12.8% had insomnia at one time point only, 4.1% at two points, 1.5% at three points and 0.3% at four points.
Prevalence, incidence and recurrence (%) of DSM-IV and DSM-5-defined insomnia (n=1037)
The prevalence of insomnia for the two sexes is displayed in online supplementary eFigure 2. DSM-IV insomnia was more common in girls (13.7%, 95% CI 9.6 to 17.7) than in boys (6.7%, 95% CI 3.5 to 10.0) at the age of 14 years (Wald=6.79, df=1, p=0.009), and marginally more common in girls (11.4%, 95% CI 8.2 to 14.6) than in boys (7.1%, 95% CI 4.5 to 9.8) when comparing the mean prevalence of DSM-IV-defined insomnia in early adolescence (ages 12–14 years; Wald=4.02, df=1, p=0.045). Additionally, DSM-IV insomnia was more common among boys (11.5%, 95% CI 7.9 to 15.1) than among girls (5.4%, 95% CI 3.1 to 7.8) at the age of 8 years (Wald=7.64, df=1, p=0.006), and more common among boys (8.1%, 95% CI 6.1 to 10.2) than girls (4.5%, 95% CI 3.1 to 5.8) when comparing means for insomnia for the two sexes in childhood overall (ages 4–10 years; Wald=8.98, df=1, p=0.003). No sex difference in insomnia was found using DSM-5 insomnia criteria.
Supplemental material
The prevalence of the specific symptoms of DSM-IV and DSM-5 insomnia is displayed in table 2. Prolonged latency of sleep onset was the most common insomnia symptom throughout the study period. The least frequent DSM-IV symptom was nocturnal awakenings, while none of the participants were troubled with the DSM-5 symptom of early morning awakenings. Comparing the prevalence of DSM-IV and DSM-5 symptoms for the two sexes revealed that the symptom of non-restorative sleep (DSM-IV) was more common in girls (17.8%) than in boys (8.0%) at the age of 14 years (Wald=11.87, df=1, p=0.001).
Prevalence (%) of symptoms of DSM-IV and DSM-5 insomnia (n=1037)
Stability and course
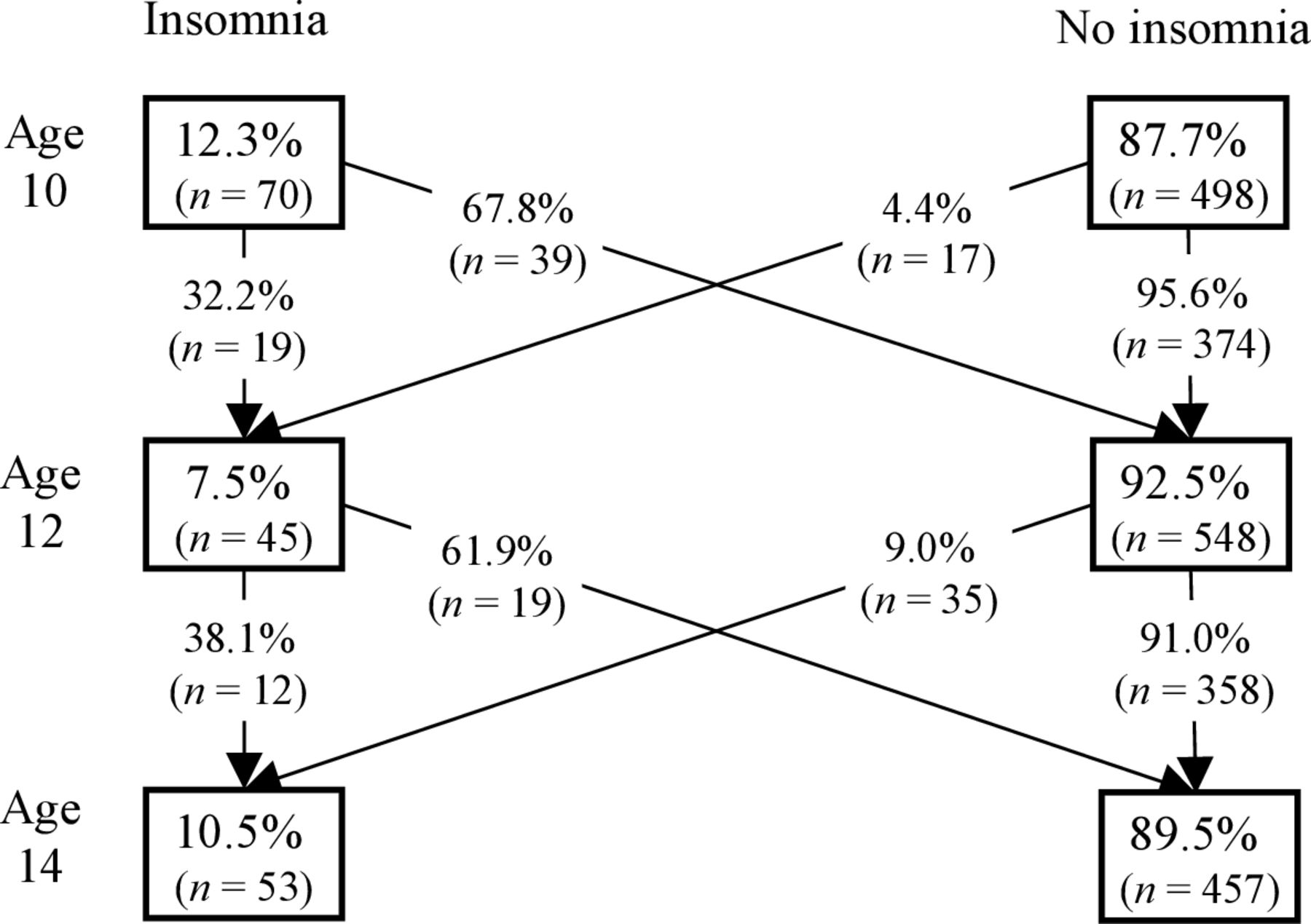
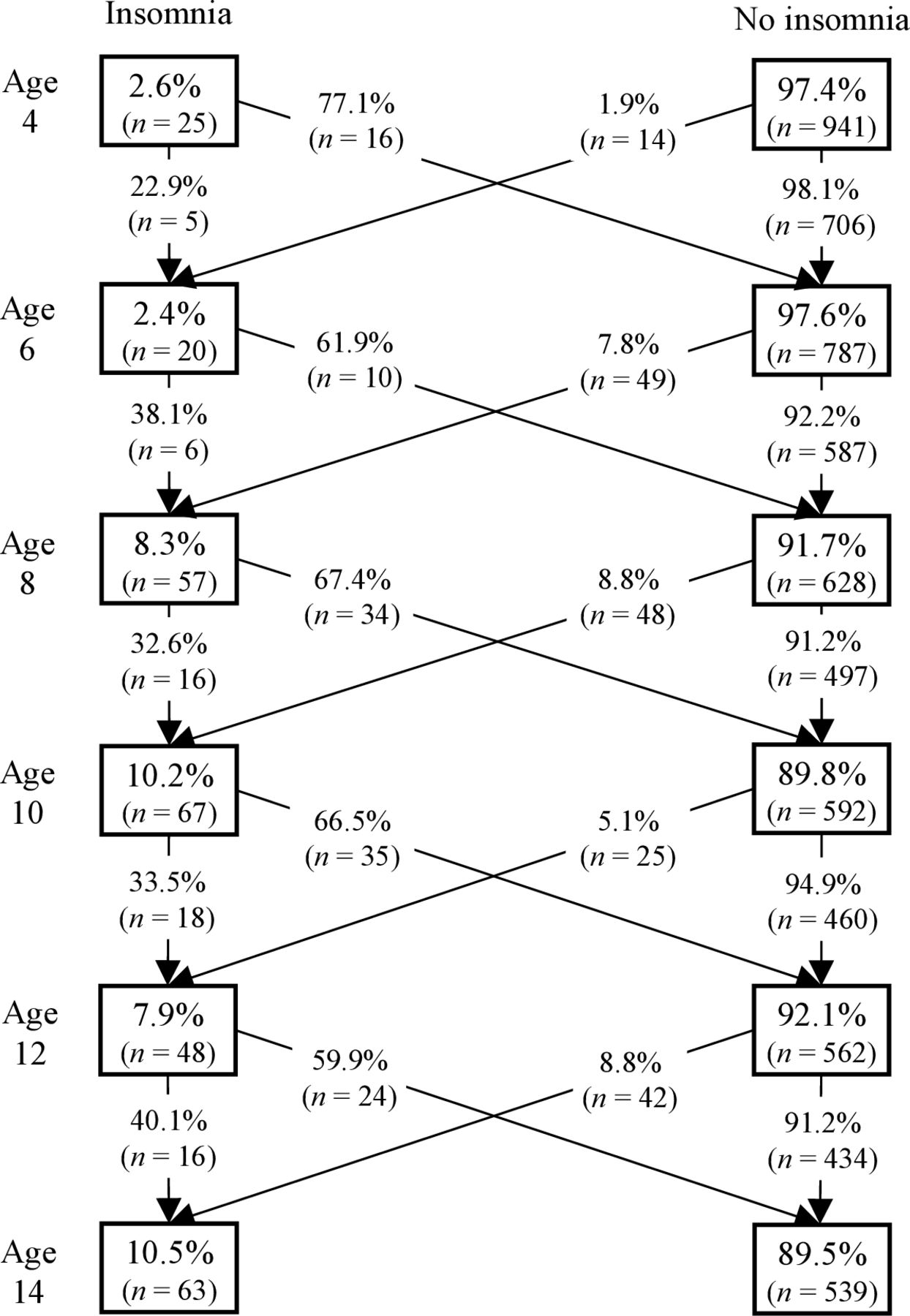
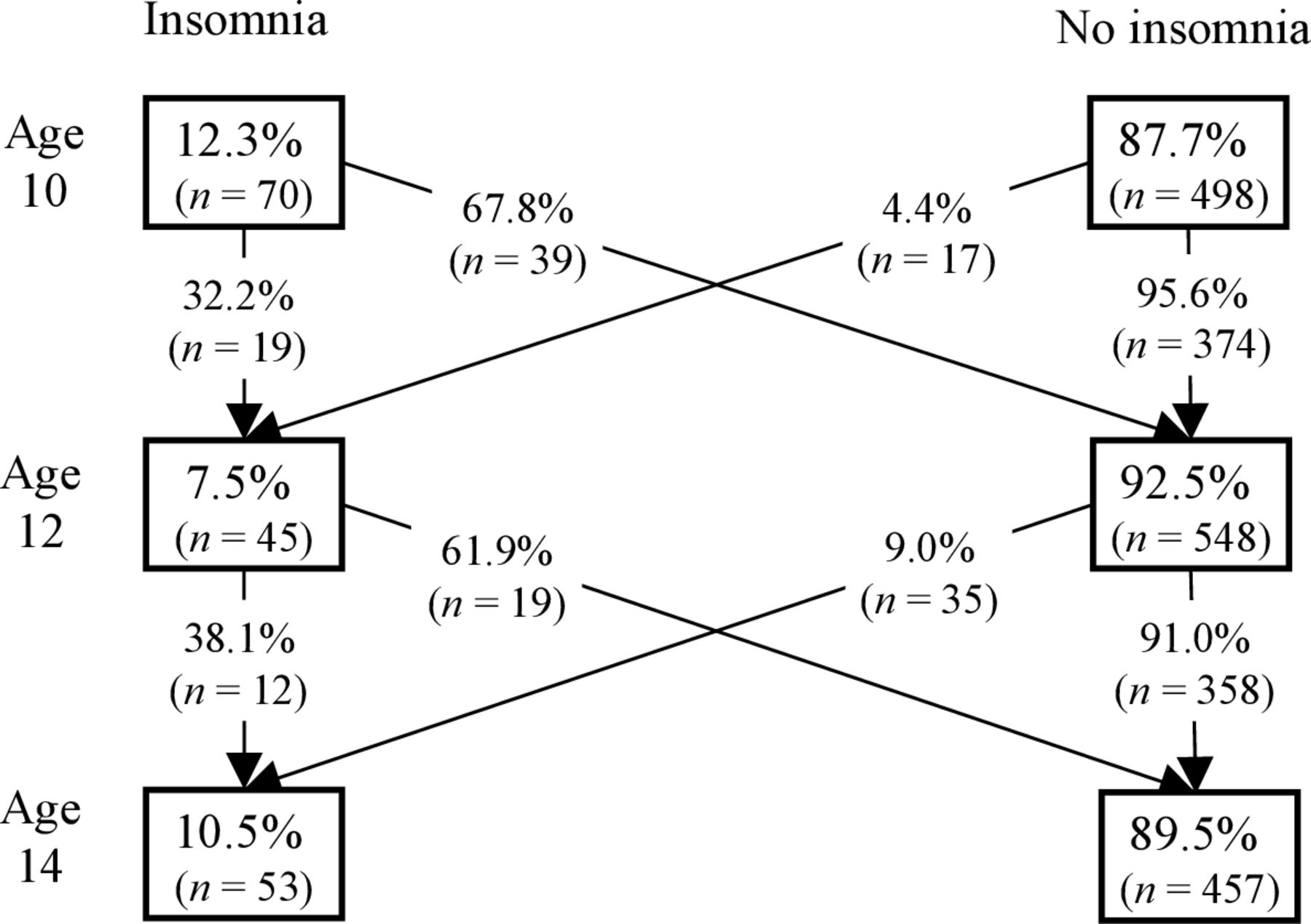
Figures 1 and 2 display the course of DSM-IV and DSM-5 insomnia. Between 32% and 40% of those with an insomnia diagnosis at one time point experienced the same disorder 2 years later, participants aged 4–6 years being the exception (23%). Table 3 reveals insomnia to exhibit a moderate to high 2-year stability, with current insomnia increasing the probability of subsequent insomnia by 5–15 times compared with not having an insomnia disorder at the preceding time point. In addition, insomnia during preschool years (ages 4–6 years) increased the risk of insomnia in middle childhood (ages 8–10 years), and insomnia in middle childhood predicted insomnia in early adolescence (ages 12–14 years).
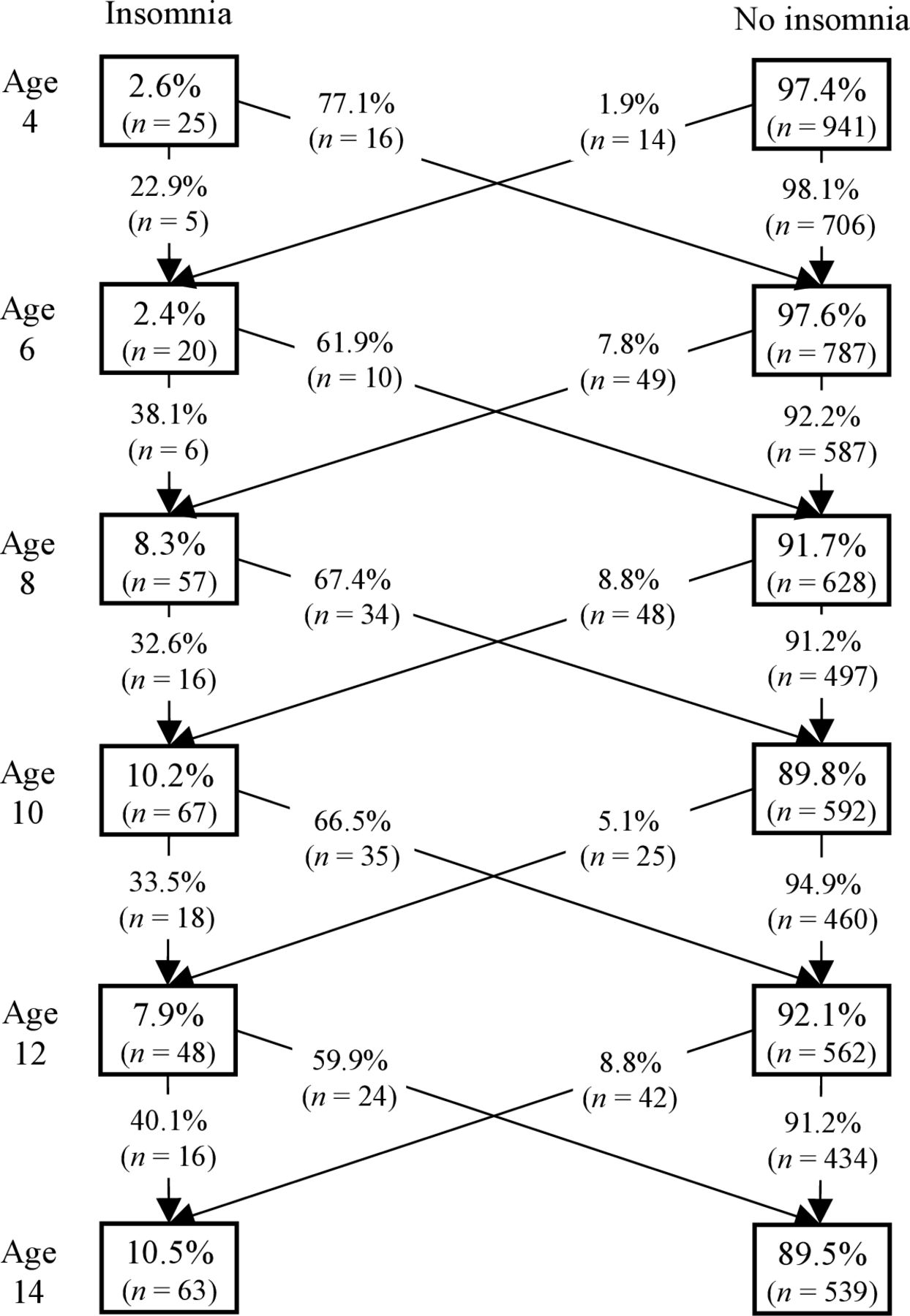
Course of DSM-IV insomnia. Numbers in boxes are prevalence estimates while numbers outside boxes are from pairwise crosstabs (only those present for the two ages in question). Number of subjects rounded to closest whole number, as they are originally population estimates. DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition.
{kind=link}
{kind=link}
Course of DSM-5 insomnia. Numbers in boxes are prevalence estimates while numbers outside boxes are from pairwise crosstabs (only those present for the two ages in question). Number of subjects rounded to closest whole number, as they are originally population estimates. DSM-5, Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition.
Stability of DSM-IV and DSM-5 insomnia (n=1037)
Sex-specific analyses showed that DSM-IV insomnia was more stable in boys from age 4 to age 6 years than in girls (who displayed no stability; Wald=58.81, df=1, p<0.001). No other sex differences in stability were found. There was no difference in 2-year stability between DSM-IV and DSM-5-defined insomnia.
Discussion
Biennial interview-based assessments from age 4 to 14 years revealed that approximately 2.5% of children met the criteria for insomnia diagnosis at 4 and 6 years of age, whereas at ages 8, 10, 12 and 14 years the prevalence ranged from 7.5% to 12.3%. Insomnia proved to be stable; 23%–40% of children had retained their diagnosis 2 years later and current insomnia increased the probability of insomnia 2 years later by 5–15 times.
Prevalence of insomnia diagnosis
No previous study has examined the prevalence of diagnosable insomnia from preschool to early adolescence. The three studies employing semistructured interviews that have been carried out reported considerably higher prevalence estimates, ranging from 16.6% to 21.2%,16–18 compared with the present findings. The discrepancy may be due to these former studies employing broader age ranges18 or using DSM-IV criteria with more liberal cut-offs for sleep latency and time awake after sleep onset.16 17 Notably though, our estimate of the prevalence of insomnia substantially exceeds the rate of children and adolescents receiving insomnia diagnoses in primary care (0.05%–1.20%),37 38 suggesting that insomnia is underdiagnosed in children aged 4–14 years. Given that receiving treatment for insomnia usually depends on being diagnosed with insomnia, this gap is problematic and might indicate that many children who need treatment do not receive it.
The increase in insomnia from preschool to middle childhood does not match previous research on childhood insomnia,12 13 17 18 probably due to our inclusion of children as informants from age 8 years and onwards. As children grow older, parents may be unaware of their offspring’s sleeping difficulties (eg, staying in bed despite difficulty falling asleep), thus insomnia prevalence research relying on parents only probably underestimates prevalence estimates.
In the current study female preponderance emerged in early adolescence, which is in line with the typical 11–12 years of age reported in the literature.21 22 39 The sex difference found with DSM-IV criteria indicating that insomnia is more common in boys than in girls in the period from 4 to 10 years of age is novel in the insomnia literature and should therefore be interpreted cautiously. Notably, no sex differences were found with DSM-5 criteria. This may be due to the observed sex difference at age 14 years in non-restorative sleep (DSM-IV), the symptom that was replaced by early morning awakenings in the DSM-5 which we found to be non-existent and therefore not contributing to a sex difference. The absence of early morning awakenings in our study may be a consequence of emerging circadian delay in early adolescence, yet this probably does not explain the non-existence at earlier ages. Alternatively, not finding any sex differences with DSM-5 criteria may be a consequence of more missing data than with DSM-IV criteria (see figures 1 and 2 for numbers) from 10 to 14 years of age and thus reduced statistical power in gender-specific analyses, although our analytical sample of 1037 with the full information maximum likelihood procedure to account for missing data tried to compensate somewhat for the reduced power.
The course of insomnia
Our results reveal that for approximately 23%–40% of children, insomnia is stable over a 2-year span. Thus, for most children insomnia is transient. In adults, on the other hand, insomnia usually fosters further sleep problems through maladaptive coping behaviours (eg, daytime naps) and negative beliefs about sleep (eg, exaggeration of the consequences of the lack of sleep)40 as well as conditioning.41 That said, for a subgroup of children insomnia is persistent and warrants clinical attention. Hence, research identifying the characteristics of those with persistent insomnia is much needed.
Limitations
Aside from the strengths of the current study—including entailing a large longitudinal community sample followed up biennially for 10 years and administering clinical interviews based on formal diagnostic criteria—there are notable limitations. First, we applied a 3-month period for insomnia symptoms as this was the inquired period in PAPA and CAPA and might thus have underestimated the prevalence of DSM-IV insomnia. This underestimation may be especially prominent at 8 years of age, with our conservative proxy insomnia diagnosis (a 1-hour threshold for sleep latency and night awakenings). Conversely, the lack of possibility to exclude other sleep disorders (eg, circadian disorders, sleep-disordered breathing) may have led to overestimation of insomnia prevalence. Second, as the sample was mainly of Norwegian origin our findings may not apply to more ethnically diverse populations or other geographical locations. Third, although there are numerous similarities between the DSM-IV and DSM-5 criteria, this study applied only DSM-IV insomnia data for the whole study period as this was the diagnostic manual in use at the start of the study. Still, our results from age 10 to 14 years with both diagnostic criteria indicate that DSM-IV and DSM-5 insomnia criteria do not yield significantly different prevalence or stability estimates. Lastly, with regard to the revealed sex differences in DSM-IV-defined insomnia at both disorder and symptom level, it should be acknowledged that these analyses by sex and age led to multiple estimations, which increases the risk of false positives.
Conclusions
The present study is the first to provide age-specific population prevalence estimates and chronicle the stability of insomnia, from preschool to early adolescence, obtained through clinical interviews. DSM-defined insomnia was less prevalent (ie, 2.4%–12.3%) than has been indicated by previous research. No difference in prevalence or stability estimates for insomnia was found using DSM-IV versus DSM-5 criteria. Girls had marginally more DSM-IV insomnia in early adolescence (ages 12–14 years) than did boys, while boys had more insomnia than did girls in childhood (ages 4–10 years). Yet no sex differences were found using the DSM-5 criteria, probably due to no child having the newly added DSM-5 symptom of early morning awakenings. Insomnia proved moderately to highly stable, as illustrated by results showing that between 23% and 40% maintained their insomnia disorder over a 2-year period, and those with current insomnia (compared with those without) were 5–15 times as likely to have subsequent insomnia.
References
Footnotes
Contributors All authors have participated in the concept and design of the study and the drafting and revision of the manuscript and have approved the manuscript as submitted. All authors are responsible for the reported research. JFM carried out the main part of the analyses and interpretation of data and drafted, revised and finalised the manuscript. LW and SS conceptualised and designed the study, organised the acquisition of data, reviewed and revised both analyses and the manuscript. SP contributed to the study design and tools for data acquisition and critically revised the text for important intellectual content.
Funding This research was funded by grants from the Research Council of Norway (grant numbers 228685 and ES611813) and a grant from the Liaison Committee between Central Norway RHA and NTNU, the Norwegian Council for Mental Health (NCMH) and the Dam Foundation (project number: 2017/FO143510).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Regional Committee for Medical and Health Research Ethics Mid-Norway approved the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. Participants have not consented to data sharing.