Article Text

Abstract
Background Congenital anomalies are the fifth leading cause of under-5 mortality globally. The greatest burden is faced by those in low/middle-income countries (LMICs), where over 95% of deaths occur. Many of these deaths may be preventable through antenatal diagnosis and early intervention. This systematic literature review investigates the use of antenatal ultrasound to diagnose congenital anomalies and improve the health outcomes of infants in LMICs.
Methods A systematic literature review was conducted using three search strings: (1) structural congenital anomalies; (2) LMICs; and (3) antenatal diagnosis. The search was conducted on the following databases: Medline, Embase, PubMed and the Cochrane Library. Title, abstract and full-text screening was undertaken in duplicate by two reviewers independently. Consensus among the wider authorship was sought for discrepancies. The primary analysis focused on the availability and effectiveness of antenatal ultrasound for diagnosing structural congenital anomalies. Secondary outcomes included neonatal morbidity and mortality, termination rates, referral rates for further antenatal care and training level of the ultrasonographer. Relevant policy data were sought.
Results The search produced 4062 articles; 97 were included in the review. The median percentage of women receiving an antenatal ultrasound examination was 50.0% in African studies and 90.7% in Asian studies (range 6.8%–98.8%). Median detection rates were: 16.7% Africa, 34.3% South America, 34.7% Asia and 47.3% Europe (range 0%–100%). The training level of the ultrasound provider may affect detection rates. Four articles compared morbidity and mortality outcomes, with inconclusive results. Significant variations in termination rates were found (0%–98.3%). No articles addressed referral rates.
Conclusion Antenatal detection of congenital anomalies remains highly variable across LMICs and is particularly low in sub-Saharan Africa. Further research is required to investigate the role of antenatal diagnosis for improving survival from congenital anomalies in LMICs.
PROSPERO registration number CRD42019105620.
- screening
- neonatology
- congenital abnorm
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Introduction
Congenital anomalies are one of the leading causes of neonatal morbidity and mortality globally. The greatest burden of disease is faced by those in low/middle-income countries (LMICs), as 94% of congenital anomalies occur in these regions.1 Congenital anomalies comprise 9% of the total global burden of surgical disease and account for 57.7 million disability-adjusted life years lost annually across the globe.2 Recent estimates suggest that approximately 303 000 neonates die annually from congenital anomalies before reaching just 4 weeks of age.3 However, many experts believe that this is an underestimate, due to a lack of congenital anomaly registries and some neonates dying without a diagnosis or inclusion within current statistics.
The WHO defines congenital anomalies as either structural or functional abnormalities which occur during intrauterine development.3 Structural anomalies are physical abnormalities that occur when the organs or skeletal structure are improperly formed. These can often be detected on ultrasound antenatally and are the focus of this review. Some common structural congenital anomalies include heart defects, cleft lip and palate, neural tube defects, limb deformities and abdominal wall defects. Many structural anomalies require immediate surgical intervention at birth to avoid death or preventable disability. In such cases, antenatal diagnosis permits delivery at a centre where the appropriate surgical care can be provided on delivery, for example, gastroschisis where the intestines protrude through a hole in the abdominal wall at birth. In high-income countries (HICs), where the majority of cases are antenatally diagnosed, mortality is less than 5%, while in many LMICs, with limited antenatal diagnosis, the mortality rate can be as high as 100%.4–6
The use of ultrasound technology in LMICs has significantly increased in recent years, as ultrasound machines have become more compact, transportable and affordable.7 Yet, a great number of congenital anomalies that can be detected antenatally via ultrasound go undiagnosed. Factors identified as barriers to effective antenatal ultrasound include limited training, equipment shortages, faulty ultrasound equipment and lack of maintenance services.7 In recent years, higher global priority has been given to neonatal health. Sustainable development goal 3.2 aims to end all preventable under-5 deaths and reduce neonatal mortality in every country to 12 per 1000 live births.8 In 2010, the WHO released the 63rd World Health Assembly Report on Birth Defects, recommending ‘prevention whenever possible, to implement screening programs and to provide care and ongoing support to children with birth defects and their families’.9
To develop a better understanding of antenatal ultrasound provision in LMICs, this study aimed to systematically investigate the availability and effectiveness of antenatal ultrasound in the diagnosis of structural congenital anomalies in LMICs. It further aimed to evaluate the effects of antenatal ultrasound diagnosis on mortality and morbidity outcomes, termination rates and referral for further antenatal care and management planning. Additionally, it assessed the level of training of ultrasonographers undertaking antenatal scans and relevant antenatal ultrasound policies in LMICs. This information is vital to help clarify the existing disparities in antenatal ultrasound provision and the potential benefits for improved health outcomes.
Methodology
Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines have been followed when conducting this systematic review (online supplementary file 1).10 11 A protocol for this systematic review was published in BMJ Paediatrics Open.12
Supplemental material
Search strategy
A search was conducted using three search strings: (1) structural congenital anomalies, (2) LMICs and (3) antenatal diagnosis using ultrasound (online supplementary file 2). Using the Ovid programme, an electronic database search was conducted on Medline, Embase, PubMed and the Cochrane Library. These searches were filtered to only include studies with human subjects. An example of the search in Medline can be found in online supplementary file 3. Only fetuses with a structural congenital anomaly as listed in search string 1 were included. Only studies from LMICs were included; these were limited to the English language. Studies with less than five patients were excluded. A further search was conducted on the WHO website to identify relevant grey literature, particularly related to antenatal ultrasound policy. The following terms were searched in the WHO Reproductive Health Library: ultrasound, ultrasonography, congenital anomalies, congenital abnormalities, congenital anomaly, congenital abnormality, birth defect, antenatal detection, prenatal detection, antenatal diagnosis and prenatal diagnosis. Following the search of each term, the results were expanded using a snowball strategy to optimise the inclusion of all relevant data.
Supplemental material
Supplemental material
Study design
All forms of evidence-based research were included. This includes systematic reviews, meta-analyses, randomised controlled trials, descriptive observational studies, case-control studies, cohort studies and case series.
Methodological quality
Although the researchers intended to use the Cochrane Risk of Bias for Non-Randomised Studies of Interventions and the revised tool to assess Risk of Bias in Randomised Trials V.2.0 to evaluate methodological quality, the majority of studies included in this systematic review were not interventional studies. Overall, the data were heterogenous and descriptive in nature, which was not suitable for existing quality assessment tools.
Study screening
References produced from the search results were added to EndNote V.X8 and duplicates were removed. The articles were then uploaded to Covidence and screened in duplicate. Articles that did not meet the study criteria were removed.
Data extraction and synthesis
Data extraction was undertaken by the principal investigator. The data extraction table can be found in online supplementary file 4. The primary analysis focused on the availability and effectiveness of antenatal ultrasound for structural congenital anomalies. Secondary outcomes included neonatal morbidity and mortality, termination rates and referral rates for further antenatal care. The results are presented in tables and descriptive statistics (range and median) have been calculated regionally.
Supplemental material
Patient and public involvement
Given that this is a systematic literature review, there was no patient or public involvement for the collection of data and literature review. Public involvement will be important for prioritising antenatal ultrasound on the political agenda and improving antenatal care programmes. To disseminate the results of this study, international charities and organisations involving structural congenital anomalies will be approached to assist in circulation.
Results
Study screening
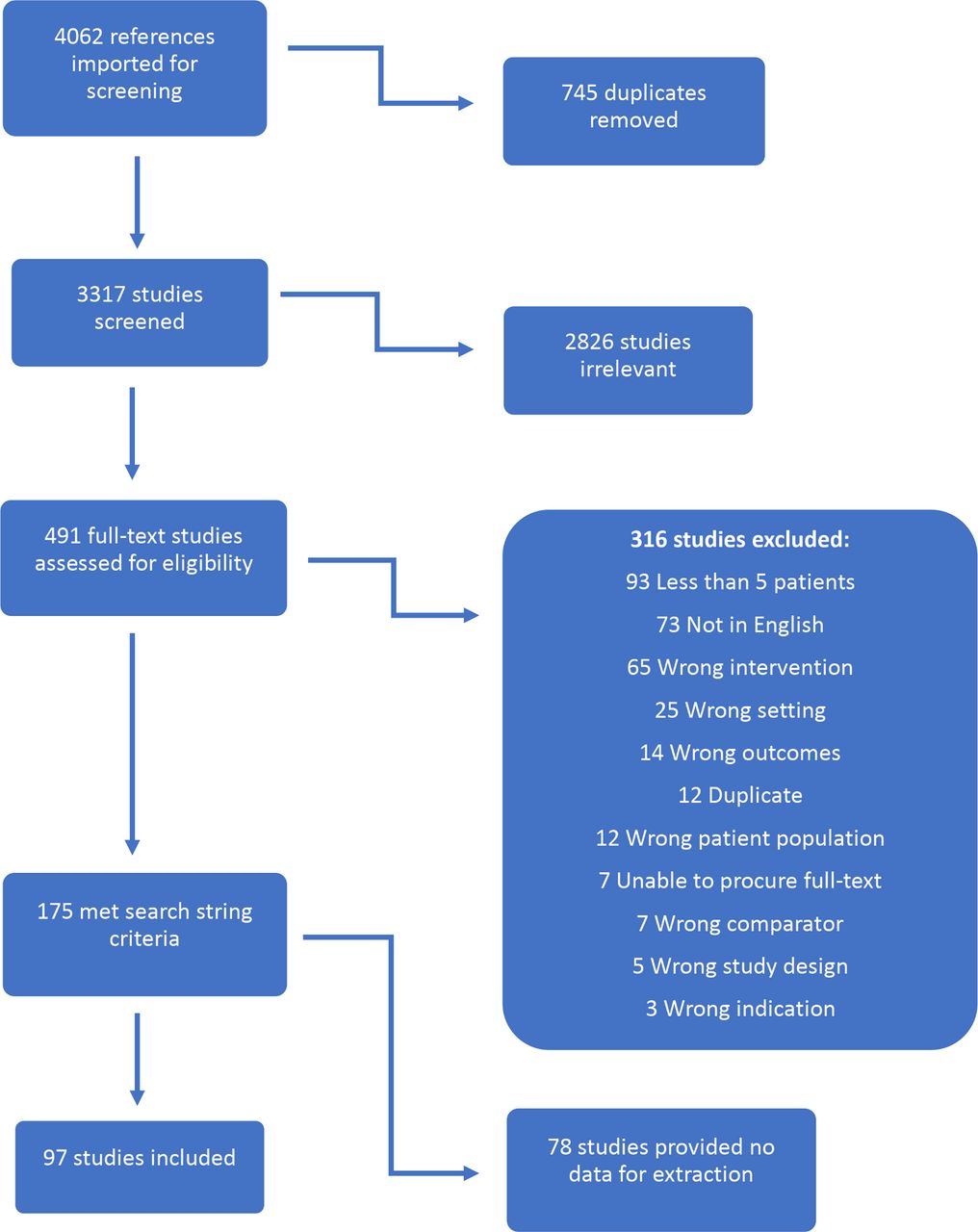
The search produced 4062 articles. Of these, 745 duplicates were removed. The remaining 3317 articles underwent abstract and title review by two independent reviewers. Of the 3317 articles screened, 2826 were excluded. Four hundred and ninety-one articles were then reviewed by two independent reviewers in full text. At this stage, 316 articles were excluded; 73 for non-English language (online supplementary file 5).
Supplemental material
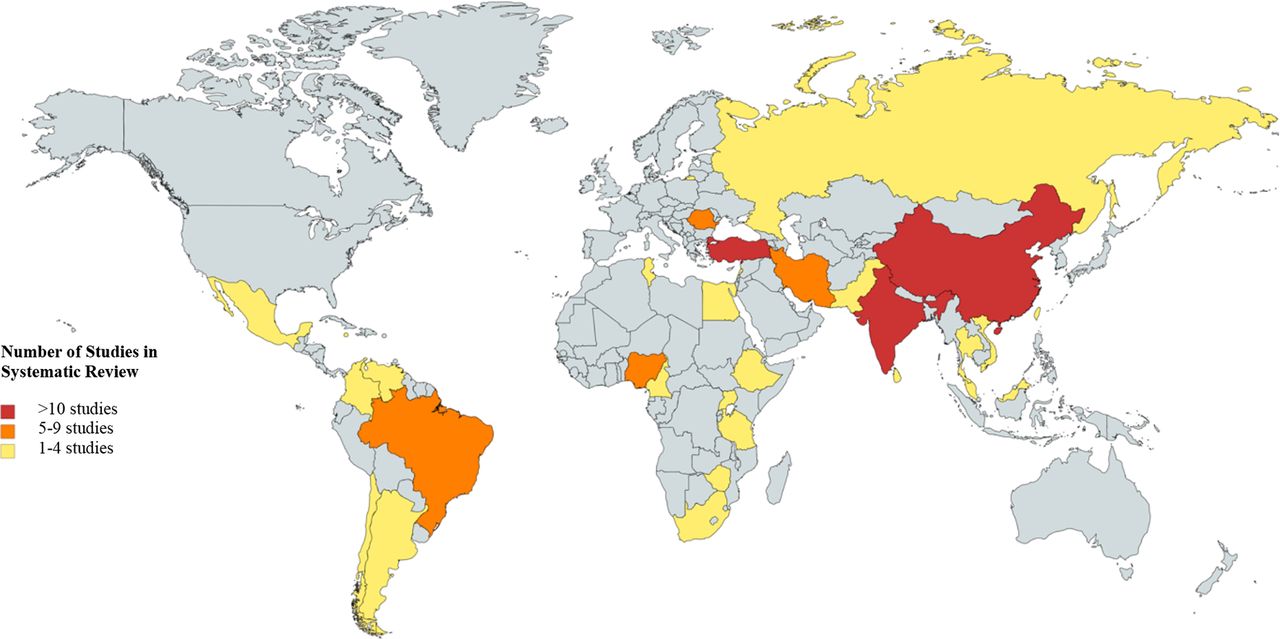
One hundred and seventy-five articles were found to meet all inclusion criteria listed in the search strings. Of these, 78 provided no data relevant to the study and thus were excluded. Ninety-seven studies were included in the data extraction phase (figure 1). Although all LMICs as defined by the World Bank were included in the search, not all countries yielded results in the text screening. One hundred and thirty-eight LMICs were included in the literature search; however, only 29 countries (21%) had any data that met the inclusion criteria (figure 2, online supplementary file 6).
Supplemental material

Flow chart of the screening process.

{kind=link}
{kind=link}
Regional depiction of articles included in the systematic review.
It is also notable that the majority of included studies were conducted on an institutional level. Thus, while the data from these studies provide important information from the countries of this review, they are by no means a representative sample of an entire country or even an entire city. Each article also varied widely in the information it provided, ranging from antenatal detection rates to policy analysis. Given the heterogeneity of data extrapolated from these articles, it was not feasible to perform a meta-analysis.
Percentage of women receiving antenatal ultrasound
Twenty-one studies (12 retrospective and 9 prospective observational studies) in 12 countries provided data on this (table 1). There was significant variation in the percentage of women receiving antenatal ultrasound scans, ranging from 6.8% in a Tanzanian study to 98.8% in a study from China. The data suggest a particularly low rate of women receiving antenatal ultrasound in Africa, with a median of 50.0% compared with 90.7% in Asia. No studies were conducted in Europe or South America, and only one study was conducted in North America (Jamaica, 98.2%).
Percentage of women receiving antenatal ultrasound
Effectiveness of antenatal ultrasound
Sixty-five studies (46 retrospective and 18 prospective observational studies and a parent survey) in 22 countries provided data on detection rates (table 2). Detection rates varied widely across studies, from 0% to 100%, with little correlation according to geographical region or type of anomaly. In Africa, the median detection rate was 16.7%, which is low compared with other LMICs, with 34.3% in South America, 34.7% in Asia and 47.3% in Europe. There was only one study from North America (Jamaica, 77.2%). Of the studies conducted from Africa, 8 of the 15 were in Nigeria and hence may not be representative of the whole region.
Effectiveness of antenatal ultrasound
Training of personnel performing ultrasound examination
Fifteen of the studies detailed the training of the personnel providing the ultrasound scans (table 3). Several of the included studies mentioned that the scans were performed by ‘experienced sonographers,’ but provided little detail as to the actual level of training of these providers. This makes it difficult to accurately assess the role that training may have in the detection of structural congenital anomalies.
Training of personnel performing ultrasound examination
Morbidity and mortality outcomes
Only four studies produced any data comparing the morbidity and mortality outcomes between neonates with an antenatal diagnosis versus neonates with a postnatal diagnosis (table 4). In the study that addressed gastroschisis, outcomes were more favourable for neonates who had received an antenatal diagnosis compared with those who had not (20% vs 66.7% mortality). This was not the case for the study which addressed congenital diaphragmatic hernia (CDH); however, this may reflect that more severe forms of anomalies are easier to detect antenatally.
Morbidity and mortality outcomes
Termination rates
Twenty-five studies (21 retrospective and 3 prospective observational studies and an ethnographic study) in 15 countries provided data on termination rates (table 5). Termination rates were highly varied, with a median of 17.1% in Africa, 34.4% in Asia, 50.2% in Europe and 62.4% in South America (range 0%–98.3%). Only one study from Africa evaluated termination rates for lethal anomalies and had just five participants. Thus, it is difficult to compare the termination rate of lethal anomalies with other regions, which contain such data. Termination rates can also be affected by the type of anomaly, the severity, the gestational age at diagnosis, the national termination policies and the cultural appropriateness of termination. Hence, while these termination rates offer valuable insight, it is necessary to also consider the underlying determinants that have impacted termination decisions.
Termination rates
Referral rates for further antenatal care and management planning
No studies addressed this issue.
Policy data
Thirteen articles provided policy data from 10 countries (table 6). Only two studies, in India and Brazil, mentioned national policies for antenatal ultrasound simply stating that they did not exist. Termination of pregnancy remains a highly sensitive topic in many communities, which is reflected in the variation of policies across the globe.
Policy data
Policy assessment
WHO guidelines recommend the need for one antenatal ultrasound scan prior to 24 weeks gestation.13 Studies suggest that the ideal detection window for structural congenital anomalies is 19–21 weeks of gestation.14 At this point, it is possible to detect most structural congenital anomalies and is within the legal termination timeframe for many countries. Of note, many of the congenital anomalies detected antenatally in this review were not diagnosed until after 24 weeks gestation. This may be explained by the timing of the first antenatal ultrasound and/or the level of ultrasonographer training. The WHO recommends that ultrasound trainees receive at least 3–6 months of training, culminating in 300–500 ultrasound examinations.15 A recent study found that the majority of ultrasound providers in LMICs do not have the minimum training as set by the WHO.16 Hence, many ultrasound practitioners in LMICs may not have the skills to accurately detect congenital anomalies.
Discussion
The median proportion of women receiving an antenatal ultrasound varied from 50.0% in Africa to 90.7% in Asia. It is likely that these are an overestimate of the true population rates considering that the majority of studies were undertaken at tertiary facilities. To fully understand what percentage of women receive antenatal ultrasound, further studies must be conducted at a population level, regionally and nationally, rather than at an institutional level. Research must also address the availability and accessibility of antenatal ultrasound and the barriers to receiving a scan.
Detection rates varied widely, from 0% to 100%, with the lowest reported rates in Africa (16.7%). Low detection rates may be because ultrasound providers did not specifically screen for congenital anomalies. Currently, many women in LMICs receive antenatal ultrasound examinations for the assessment of pregnancy progress, such as to determine the gestational age, sex of the baby and to hear the heartbeat, rather than to detect anomalies. This is in contrast to HICs where the majority of women receive an anomaly scan around 20 weeks gestation.14 Another possible reason for low detection may be the training level of the ultrasound provider; there appears to be a trend between higher levels of training and higher detection rates. This warrants further investigation to determine minimum training requirements and associated policy and monitoring.
The First Look Study is an important randomised controlled trial which assessed the use of antenatal ultrasound in the Democratic Republic of the Congo, Guatemala, Kenya, Pakistan and Zambia.17 Although 95% of women in their intervention group received antenatal ultrasound scans (compared with 43% in the control group) and detection rates improved, hospital delivery did not increase for complicated pregnancies and thus there was no resultant improvement in neonatal mortality. In an additional survey by the same group, barriers to referral attendance included cost, distance and lack of transportation.18 For women who did attend referral, barriers included not being connected to the correct provider and being told to return at a later time.18 The authors conclude that without improvement of subsequent care, antenatal ultrasound offered limited impact.17 Hence, to reduce neonatal morbidity and mortality, detection of an anomaly must be followed by referral for antenatal counselling and delivery at a tertiary centre which can provide the necessary surgical care at birth where required. It is also necessary to offer termination for conditions which are incompatible with life, where culturally acceptable.
Hence, it is vital to further investigate barriers to accessing delivery at a paediatric surgery centre once a congenital anomaly has been diagnosed and ways to address these barriers. Future studies must also investigate the effects of both antenatal diagnosis and delivery at a tertiary paediatric surgery centre on morbidity and mortality outcomes in the LMIC setting; this systematic review highlighted a severe lack of such vital data. The recently completed Global PaedSurg study may provide such data for a selection of common gastrointestinal congenital anomalies globally, which collectively have a particularly high mortality in the LMIC setting.19 As anomaly screening rates increase in LMICs, it will be also be important to monitor termination rates along with reasons for termination, to ensure the benefits of antenatal diagnosis are optimised both clinically and ethically.
To address some of these issues, there is a need for global collaboration. This collaboration must include members from multidisciplinary backgrounds, including policymakers, obstetricians, neonatologists, paediatric surgeons, midwives and allied professionals. The Global Initiative for Children’s Surgery (GICS) is a multidisciplinary collaborative whose aim is to improve health outcomes for children requiring surgery in LMICs.20 This initiative connects the expertise of providers in LMICs and HICs and is committed to expanding the representation and leadership of stakeholders in LMICs. GICS has recently created a congenital anomalies working group, which is planning some of the following projects: (1) to produce guidelines on how to diagnose structural congenital anomalies via antenatal ultrasound; (2) to produce referral and management guidelines following an antenatal diagnosis; and (3) to produce information sheets that can be translated into various languages for parents that contain details about common congenital anomalies. Global collaboration must also extend to the level of the WHO and the Ministries of Health to ensure that recommendations are detailed in policy and implemented into practice.
If these steps are taken, improvements in neonatal health outcomes may be realised, as seen in HICs. Early detection and immediate surgical intervention of congenital anomalies, such as gastroschisis, has been effective in significantly reducing neonatal mortality in HICs.5 The mortality of gastroschisis has significantly improved in HICs over a period of 50 years, to less than 5% today.5 This can be attributed to improvements in accurately diagnosing gastroschisis antenatally, monitoring the fetus for complications, and planning for delivery at a facility with paediatric surgeons available.21 Similar trends have been seen for other congenital anomalies in HICs such as intestinal atresia, CDH, omphalocele, oesophageal atresia and posterior urethral values. By understanding the current role of antenatal ultrasound in LMICs and the barriers to detection, referral and management of structural congenital anomalies, appropriate interventions can be implemented to help improve outcomes.
Although this systematic review provides useful data, it is also important to note a few of the limitations of the study. First, only articles in English were included in this systematic review, which may exclude other relevant studies. This study used four electronic databases for the search. The expansion of search databases to include African Journals Online, Scielo and Regional WHO’s African Index Medicus may have provided other studies from LMICs that were not indexed in the search engines used. It is vital to include these databases in future research focusing on LMICs. Furthermore, it is important to note that antenatal ultrasound has further diagnostic capabilities, such as detecting abnormal growth or improper placental position and this review only focused on the detection of structural congenital anomalies. Further studies could also include other uses of antenatal ultrasound for improving neonatal and indeed maternal health outcomes. Finally, the policy data in this study represent what was accurate when the studies were published. Some of the policy data may now be out of date.
Conclusion
The data from this review suggest that the percentage of women in LMICs who receive an antenatal ultrasound examination varies considerably and is particularly low in sub-Saharan African countries. Even when antenatal ultrasound scans are performed, accurate detection rates are often very low. The level of training (and the type of training) of the sonographer may be indicative of the accuracy of diagnosis. Only four studies delineated the morbidity and mortality outcomes among neonates with an antenatal diagnosis compared with postnatal diagnosis. Hence, although the benefits of antenatal ultrasound are widely documented in HICs, data are severely lacking in LMICs. It is clear that the use of antenatal ultrasound in LMICs is not maximised to its highest potential.
What is known about the subject?
Congenital anomalies are the fifth leading cause of death in children under 5 years of age globally.
Ninety-seven per cent of congenital anomaly deaths occur in low/middle-income countries (LMICs), many of which may be preventable with antenatal diagnosis and planned surgical intervention following birth.
Antenatal ultrasound examinations in HICs are commonplace and highly accurate, but accessibility and effectiveness are limited in LMICs.
What this study adds?
Rates of antenatal ultrasound examination vary significantly in LMICs, ranging from 6.8% to 98.8%.
There is significant variation in the accuracy of antenatal diagnosis in LMICs, with detection rates varying from 0% to 100% (median of 16.7% in Africa).
Available data suggest that the level of ultrasonographer training may affect the accuracy of diagnosis, but further research into this is required.
Acknowledgments
The authors would like to thank the library services at King’s College London for help with the systematic review process.
References
Footnotes
Contributors NW conceived the idea for this study. NW, AK and SMG devised the study design. SMG, SS-B, NA-A, LIN, MTB and NW performed the literature review. SMG drafted the manuscript with significant contributions from NW and AK. All authors reviewed and approval the final submitted manuscript.
Funding NW receives funding from the Wellcome Trust to undertake a Clinical PhD in Global Health at King’s Centre for Global Health and Health Partnerships, King’s College London (Funder Reference: 203905/Z/16/Z).
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests There are no competing interests.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.