Article Text

Abstract
Head injury is the largest cause of mortality in paediatric trauma. Infants (<1 year old) are a high-risk group and vulnerable to non-accidental injury. A single-centre retrospective study at a major trauma centre collected data on infants presenting with a head injury over a 48-month period. 1127 infants presented with a head injury. 135 CT heads were performed. 38% of scans showed intracranial pathology. The decision about which infants to send for CT scans remains complex. Liberal use risks over-exposure to ionising radiation while restrictive use may miss subtler injuries.
- child abuse
- neuropathology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
The burden of paediatric trauma is significant. Head injury represents the highest cause of mortality due to childhood trauma.1 Up to 5% have intracranial pathology with potential long-term repercussions on development.
Infants (<1 year old) are a vulnerable group. They often present to hospital late after injury, with a high injury severity score and mortality. Non-accidental injury (NAI) is an important cause, representing 30%–50% of cases.1 In view of this, we decided to look into this high-risk cohort.
Methods
This is a single-centre retrospective study from 2015 to 2018 at a major paediatric trauma centre in London. Data were obtained from the Collector Registry Trauma Database. Forty-one head injury coding entries were used to identify infants (<1 year old) presenting with a range of head injuries from minor lacerations to the catastrophic. This was cross referenced with all CT heads performed in the emergency department (ED) to ensure that any patients who did not presented as trauma were not missed from our data.
Patient and public involvement
Patients were not involved.
Results
One thousand one hundred and twenty-seven infants presented with a head injury from 2015 to 2018. On average, one infant was seen every 1.3 days. One hundred CT heads were performed for these head injuries 100/1127. Most indications were for known trauma (n=74, 55%; table 1).
Total number of CT scans <1 year old and presenting problems and number of positive CT scans for intracranial pathology
Of 135, 11 (8%) of CT head indications were based on suspicion of NAI (1 trauma presentation, 3 peri-arrest/arrests and 7 as NAI screening).
Thirty-eight per cent (n=28) of CTs performed due to trauma demonstrated intracranial pathology. Scan numbers reduced after 2017; 46 (8.3%) versus 28 (4.8%).
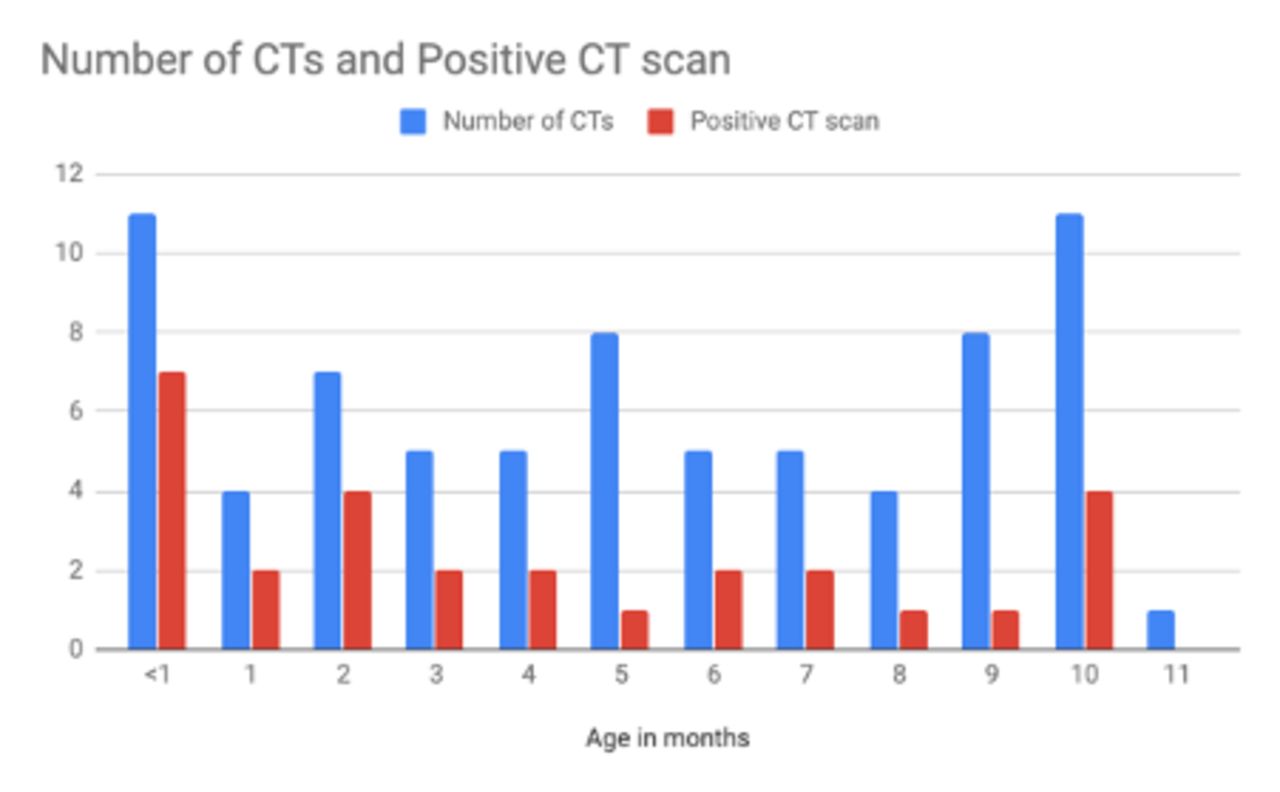
Older infants (approaching 1-year old) presented more frequently while younger infants were more likely to be scanned; 18%<1 month had a CT compared with <1% 11 months old (figure 1). The CT was more likely to show pathology in younger infants, (63%<1 month old vs 36% 11 months old).

{kind=link}
Total CTs performed and number positive for intracranial pathology (for all infants who presented as a trauma).
Reattendance to ED was low at 2.6% (n=27). Three infants re-presenting were scanned with one demonstrating pathology on CT. None of them were initially scanned on their first presentation or required surgical intervention.
Discussion
When an infant presents with suspicion of a moderate head injury but at time of review appears clinically well, the decision regarding imaging is difficult. In our dataset, 38% of scans demonstrated intracranial pathology. The reduction in scan numbers after 2017 may reflect the change in the National Institute for Health and Care Excellence guidance published in 2014.2 A high percentage of positive scans suggests that scanning frequency is appropriate and selected for obvious cases. However, the question has to be asked if subtle pathology is potentially being missed?
Frequently little to no surgical intervention occurs post imaging. Valid concerns exist involving the sensitivity of the developing brain to radiation and the increased vulnerability of children to certain cancer types. The although low risk of obtaining imaging under sedation or general anaesthesia must be considered.3
The argument for scanning is to help detect subtle pathology. Although much has been written about the ‘plasticity’ of the paediatric neuron as it grows, this does not necessarily translate to healthy development. Increasing evidence shows that moderate brain injury can lead to developmental changes. One study showed 20% of children with milder brain injuries had ongoing concentration problems and education difficulties.4 Suspected NAI cases tend to present in extremis.5
In our trust, only severe head trauma admissions have an 8-week follow-up appointment. We propose a longer study to look at later life sequelae including moderate cases, to see if subtle pathology is potentially being missed.
Footnotes
Contributors All authors involved in data collection and the writing of the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.