Article Text

Abstract
Background Children are less vulnerable to serious forms of the COVID-19 disease. However, concerns have been raised about children being the second victims of the pandemic and its control measures. Therefore, we wanted to study if the pandemic, the infection control measures and their consequences to the society projected to paediatric prehospital emergency medical services (EMS) contacts.
Methods We conducted a population-based cohort study concerning all children aged 0–15 years with EMS contacts in the Helsinki University Hospital area during 1 March 2020–31 May 2020 (study period) and equivalent periods in 2017–2019 (control periods). We analysed the demographic characteristics, time of EMS contact, reason for EMS contact, priority of the dispatch, reason for transportation, priority of transportation, if any consultations were made or additional units required, any medication or oxygen or fluids given, if intubation was performed, and whether paramedics took precautions when COVID-19 infection was suspected.
Results The number of paediatric EMS contacts decreased by 30.4% from mean of 1794 contacts to 1369 (p=0.003). The EMS contacts were more often due to trauma (+23.7%, p<0.05), dispatched in the most urgent category (+139.9%, p=0.001), additional help and the mobile intensive care unit were more frequently requested (+43.3%, p=0.040 and+46.3%, p=0.049, respectively). However, EMS contacts resulted less often in ambulance transport (−21.1%, p<0.001). Alarmingly, there were four deaths during the study period compared with 0–2 during the control periods.
Conclusions The number of EMS contacts decreased during the pandemic. Nevertheless, the children encountered by the EMS were more seriously ill than during the control periods.
- epidemiology
- health services research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Compared to adults, children are less affected by the COVID-19 infection but may be affected by its control measures.
Children may experience collateral damage because of the infection control measures, mainly designed to protect adults.
The pandemic has decreased paediatric emergency department (ED) visits, but it is not clear how or if prehospital care has also been affected.
What this study adds?
The use of prehospital emergency medical services decreased in children after declaration of the state of emergency in Finland.
During the pandemic, ambulance calls for children were more often in the most urgent category and due to trauma. Paradoxically, almost 60% of children were not transported to the ED.
Societal measures targeted to protect adults against the pandemic affected children and their emergency medical care.
Introduction
Children seem to be less vulnerable to the serious forms of the COVID-19 disease by the new pandemic coronavirus SARS-CoV-2 than adults.1–3 Still, following the infection control measures and associated abrupt changes in healthcare delivery, children have not been spared from the health effects of the pandemic. Consequently, health professionals have expressed concern over children becoming second victims of the pandemic.4–6
Instructions on social distancing and self-quarantine resulted in a considerable decrease in paediatric emergency department (ED) visits.4 5 Also, the emergency healthcare itself changed: in EDs and prehospital emergency medical services (EMS), infection control measures, including the use of personal protective equipment have slowed patient flows and resulted in modified treatment protocols. On the other hand, the ubiquitous presence of COVID-19 in news and media may have created a bias in clinicians, who may be prone to diagnostic errors, suspecting COVID-19 over more common conditions.
Decreasing unnecessary paediatric ED visits and ambulance calls has been a priority in paediatric emergency care already before the pandemic.7–9 However, alarmed by reports stating risks associated with decreases in paediatric ED visits,4 5 we wanted to study if the pandemic and social distancing measures were reflected in the amount and features of the EMS contacts with children as well. If these contacts had indeed substantially decreased, it would be important to analyse whether this change has taken place at the cost of health risks for children.
Methods
Study area and population
The Helsinki University Hospital (HUH) area in Southern Finland has 1 263 000 inhabitants including 217 000 0–15 years-old children (2019)10 and consists of both urban and suburban regions covering 1 216 km2.
This study covers all prehospital ambulance responses for children (aged 0–15 years) in the HUH area during the study and control periods.
Organisation of EMSs and healthcare system
Finland has a publicly financed universal healthcare system for all residents. The public healthcare exclusively provides all prehospital EMSs. All emergency calls go to the governmental emergency response centre (ERC). A professional ERC operator categorises the leading problem to form a dispatch code and determines a priority class from A (highest risk) to D (lowest risk) according to a formal protocol.11 In HUH area, all prehospital emergencies are responded to by HUH EMS consisting of 36 ambulances and 3 medical supervisor units staffed by emergency medical technicians, paramedics and two physician-staffed units. An emergency physician can be consulted by phone, or, requested on scene. Not all patients encountered by EMS are transported to hospital by ambulance. After on-scene examination and treatment, the EMS personnel may conclude that patient does not need ambulance transport. In that case, they must inform the patient or the caregivers on how to observe and treat the condition and on whether or when to contact healthcare services again. The protocol on the treatment and transport of children for the EMS did not change during the pandemic. Nevertheless, preferring other treatment options over nebulised medication was advised.
There are two 24/7 paediatric ED units with inpatient care in the area. In addition, smaller units offer primary level healthcare during office hours.
Data collection
We retrieved all emergency responses concerning children (age 0–15 years) from the ambulance electronic patient record system (Merlot Medi, CGI Suomi Oy) in HUH area between 1 March 2020 and 31 May 2020 (study period) and equivalent periods for three previous years: 1 March 2017–31 May 2017; 1 March 2018–31 May 2018; 1 March 2019–31 May 2019 (control periods). We chose control periods to cover three previous years and the same months in order to be able to account for any potential seasonal variation. The pandemic declaration by WHO on 11 March, the Finnish Government announcement of the state of emergency in Finland on 16 March, and the reopening of schools on 14 May were included in the study period. We analysed the time of contact, reason for contact, dispatch priority, reason for transportation, priority of transportation, age, sex, native language, whether the patient received medications, oxygen, fluids or was intubated, whether a physician was consulted or requested on-scene or additional units required, and whether COVID-19 was suspected. We investigated eventual laboratory diagnostics for respiratory viruses (including SARS-CoV-2) from the HUH in-hospital patient record system (Uranus, CGI Suomi Oy and Apotti, Epic Systems Corporation). A flow chart of EMS contacts in 2020 and possible suspicion of COVID-19 infection is presented in online supplemental material 2.
Supplemental material
Statistical analysis
Because this is a retrospective study concerning a multidimensional and rapidly progressing medicosocietal phenomenon, the possible confounders are multiple and their effects difficult to predict. As we did not aim at establishing causalities between the control measures and EMS contacts, but at noticing possible indicators of the effects of the pandemic on the health and welfare of children, we chose univariate analysis for the primary statistical method, since it gives the clinically most relevant answers to our study questions. Estimates and proportions are shown using medians and IQRs and number of events are shown using counts and percentages. To compare the change in EMS contacts during the study period to that of control periods, we used the Mann-Whitney U test or Wilcoxon signed-rank test depending on whether comparisons were made between all the observations or between the weeks of 2020 and the previous years. The analyses were performed using R V.3.6.312 and the visualisations using ggplot2-package.13 We used 0.05 as the level of significance. As the infection control measures changed during the study period, we used line plots with date as the X-axis to evaluate the eventual changes in our parameters.
This study is reported in compliance with the Strengthening the Reporting of Observational Studies in Epidemiology checklist for cohort studies (online supplemental material 3).
Supplemental material
Patient and public involvement statement
No public involvement was planned for this study, as the COVID-19 pandemic advanced rapidly.
Results
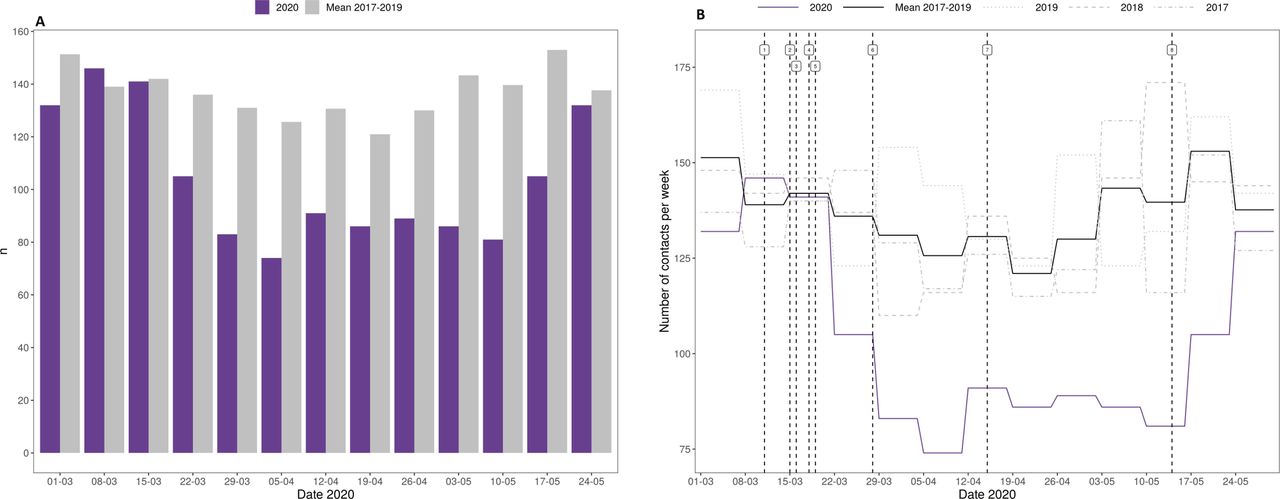
There were 28 680 prehospital EMS contacts during the study period, of which 1368 (4.8%) concerned children. This comprised a reduction of paediatric EMS contacts by 23.7% compared with the mean of 1794 contacts in control periods (figure 1). There was no statistically significant variation within the control periods (online supplemental material 1, online supplemental table 2). Patients were younger: 5.3 years compared with 6.3 years (p<0.001) and there were proportionally less children speaking one of the national languages (Finnish or Swedish) as native language: 7.8% (p=0.003). The number of EMS calls for children speaking another language, however, decreased with a delay. The sex distribution was equal in both periods (males 54.0% vs 55.1%).
Supplemental material

{kind=link}
Basic information on paediatric emergency medical services (EMS) contacts in 2020 compared with equivalent periods in 2017–2019. (A) A number of weekly EMS contacts. (B) A timeline of the course of the first pandemic wave and number of weekly EMS contacts. 1. WHO declared the pandemic, 11 March 2020. 2. Public social gatherings were limited to a maximum of 500 participants, 15 March 2020. 3. The government announced the state of emergency, 16 March 2020. 4. National restrictions and social distancing launched. Schools closed, 18 March 2020. 5. Launching strict national border control, 19 March 2020. 6. Isolation of Southern Finland started, 28, March 2020. 7. Isolation of Southern Finland ended, 15 April 2020. 8. Schools reopened, 14 May 2020.
The changes in the characteristics of EMS dispatch and transportation codes are described in table 1. The proportion of the highest priority A dispatch code rose by 139.9% (p=0.001). The absolute number of trauma patients decreased by 11.9% (p<0.02). However, their proportion increased by 23.7% (p<0.05). The proportion of non-transported patients increased by 21.1% (p<0.001; table 1).
Change in the dispatch and transportation codes
Additional help and the mobile intensive care unit were more frequently requested on-scene (+43.3%, p=0.040 and +46.3%, p=0.049, respectively). Less treatments were performed in 2020 compared with the control periods: establishing an intravenous access decreased in proportion by 32.5% (p=0.008) and administering medications by 35.3% (p<0.02; table 2).
Change in the additional units requested and interventions performed on scene
Four patients were dead on arrival of the EMS or died on scene during the study period, as compared with 0–2 during the control periods (table 3).
Mortality presented by year during equivalent periods of 1 March to 31 May
Of the 1368 children, COVID-19 infection was suspected in 103. Of these, four were previously known to be positive for SARS-CoV-2 and there were two new infections. However, 41 of the 1261 children not suspected as having COVID-19 by the EMS were tested for COVID-19 infection at the ED, with only 1 positive result.
Discussion
During a local epidemic peak of the COVID-19 pandemic, prehospital emergency care delivered to children decreased and its characteristics changed markedly. Emergency calls for children were more often categorised as urgent and an emergency medical physician or other additional help were more often needed. Concomitantly, the number of prehospital paediatric deaths during the pandemic was noteworthy. Therefore, our results suggest that the children encountered by the EMS during the pandemic were more seriously ill than before the pandemic. Paradoxically, the EMS contacts more likely led to not transporting the child to the ED (table 1).
Finland has not experienced high COVID-19 infection rates in the population so far. The highest demand for hospital beds and intensive care was experienced mid-April.14 Thus, the changes we noticed in the emergency healthcare to children were neither due to SARS CoV-2, nor to an overwhelming of the emergency healthcare system. Instead, they represent the changes in healthcare functionality, and in the behaviour of families with children.
We expected the decrease in the number of EMS contacts for children based on international reports about substantial decreases in the number of paediatric ED visits during the pandemic.15 16 Our figures were also congruent with those from the paediatric EDs in the area, which saw a 45% decrease in the number of visits after the beginning of the infection control measures, according to the hospital statistical data. The EMS contacts with children started to decrease immediately after the declaration of state of emergency, suggesting that the decrease was more societal than medical in nature.
The decrease in EMS contacts was probably due to several factors, which may represent both positive changes in the behaviour of caregivers, but also cause unnecessary risks to children. A successful public guidance during the state of emergency, encouraging parents to treat mild symptoms at home and avoid overcrowding EDs, could have eliminated some medically unjustifiable EMS contacts.9 17 In addition, infection control measures could have decreased the occurrence of acute infections in children and, hence, the occurrence of febrile seizures and dyspnoea, which are leading causes for paediatric EMS calls under normal circumstances.18 Still, especially the peak in the number of children who died on-scene warrants careful examination of the EMS contacts during the pandemic. Even if the increase in deaths is a preliminary finding and as such may be due to coincidence, we cannot confidently state that the decrease in EMS contacts was a positive proceeding. The ubiquitous presence of COVID-19 in media, reports about overcrowded EDs and a concomitant public guidance stating that all unnecessary contacts should be avoided, could have led to caregivers delaying ED visits and emergency calls even when medical attention would urgently have been needed. Noticeably, a recent report from adult EMS contacts in the UK states that the pandemic did not cause reluctance to call an ambulance in case of a real emergency, such as stroke or heart attack.19
Our results suggest that the children encountered by the EMS during the pandemic were more seriously ill than during the control periods. Although the total number of EMS contacts decreased, the number of the most urgent EMS calls with priority class A increased. Simultaneously, the proportions of contacts requiring an emergency medical physician or other additional help increased. There were no changes in the EMS protocols that could account for such finding. The high number of paediatric out-of-hospital deaths may also be related to this notice.
Even though children encountered by the EMS during the pandemic seem to have been more seriously ill than before, the contacts more often led to not transporting the child to the ED. The increase in the proportion of EMS calls in which the patient was not transported in an ambulance (‘non-transports’) is interesting, as in our system the non-transport rates were already high before pandemic.18 20 This finding is also paradoxical considering that non-urgent or non-medical problems did not seem overexpressed during the study period. The increased tendency not to transport a child by ambulance may reflect the practical difficulties imposed by the infection control measures during the pandemic, such as a time-consuming obligation to thoroughly clean the ambulance after any transport. Also, non-transport decisions are not solely based on medical decision-making, but social and logistic issues are considered as well. In our urban study area, other transport possibilities than ambulance are easily available. During the pandemic, caregivers for older children were not allowed to escort the child in an ambulance. Thus, it is likely that if the ambulance transport was medically not necessary and if the caregiver needed to use another means of transport anyway, the child may have preferred the ride with the caregiver. In addition, similarly to laypersons, the EMS personnel were also exposed to media warning about overcrowded EDs and reporting about overwhelmed healthcare systems. Even without changes in protocols, the EMS personnel may have felt a need to ascertain that a maximal number of units are available at all times for urgent cases, and, opted not to transport when there was no explicit need for ambulance transportation.
We observed a decrease in the absolute rate of traumas, but non-traumatic emergencies decreased even more. This is interesting, as we hypothesised that the decrease in EMS dispatches during the pandemic would have been most pronounced for traumas. After all, due to social distancing, children had less school and sport activities and transports in motor vehicles. Under normal circumstances, these factors are major contributors for paediatric traumas.21 On the other hand, even if schools and activities were closed, playgrounds and other public outdoor areas remained open; thus, offering more unsupervised outside playing time. These changes from normal routines may have contributed to unpredicted new risks for traumas in children.
We found that the number of EMS calls for children speaking other language than the national languages (Finnish or Swedish) decreased similarly to other contacts but with a delay. In Finland, native language can be used as a proxy for recent immigrant background. Interestingly, several reports have addressed the vulnerability of ethnic minority groups to COVID-19.22 23 Our results suggest that language and immigrant background may play a role: the information took more time to reach subpopulations with deficiencies in language skills and poor knowledge of the healthcare system. Consequently, in possible new pandemic waves, more attention should be paid to efficiently spreading accurate information in different languages and formats.
To evaluate if changes were specifically encountered by families with children, we also compared our findings to those in the total HUH population. In our area, EMS calls for adults also decreased by 11.1% (p=0.004) during the pandemic; but, in contrast to children, the absolute number of their most urgent contacts also decreased by 17.1% (p=0.004), and there was no increase in the on-scene mortality. In addition, the decrease in adult EMS contacts occurred already before the declaration of the state of emergency. The pattern for children is clearly different, which strengthens the concern raised by recent reports suggesting that children may have had to bear the burden of the restrictions of the COVID-19 pandemic differently to adults—even to the extent of becoming the ‘collateral damage’ of the pandemic.6 Taken together, these findings suggest that in adults, behavioural changes (ie, decrease in risk behaviours following social distancing, reluctance to contact medical care, etc) were responsible for most of the decrease in EMS contacts; and that, in contrast to children, the protective measures were truly protective for adults, decreasing the occurrence of severe acute illnesses and injuries. It remains to be solved how, in future pandemics, children could be protected from the negative impacts of measures designed to protect adults.
To protect the EMS and ED personnel from infections, and to optimise the use of critical resources, it would be crucial to be able to recognise children with probable or possible COVID-19. We found that calibration still needs to be done—in about half of the patients where EMS personnel suspected COVID-19, no COVID-19 tests were performed at the ED. On the other hand, only 41 of the 1261 patients in whom EMS personnel did not suspect COVID-19 infections were tested for COVID-19 with one positive result. This implies that more explicit instructions for EMS personnel are needed.24
Our study has several limitations. First, it is a single-centre study. Second, because of the rapid advance of the COVID-19 pandemic, this study is retrospective. We tried to address the lack of historic references and the question about possible pre-existing seasonal variation by comparing the data to equivalent periods of three previous years. Finally, mortality is such a rare event that no statistical conclusions can be drawn based on our data. However, we believe that this finding needs to be disclosed.
The pandemic created exceptional circumstances with rapid changes in the behaviour of families with children and the functionality of emergency healthcare. During recent pandemics, for example, the H1N1 influenza in 2009, school closure and social distancing measures were never extended to children in a similar way.25 In our area, the setting was particularly interesting, as the prevalence of COVID-19 in the population remained low throughout the epidemic.14 Thus, our results may be generalisable to other similar situations of unexpected quick changes in the healthcare.
Conclusions
The total number of contacts decreased rapidly during the COVID-19 pandemic. Also, the children encountered by the EMS were more seriously ill, and we registered a noteworthy number of prehospital deaths compared with the control periods. Our results highlight the need to consider secondary effects of the pandemic and the control measures also on other populations than those originally targeted.
References
Footnotes
Contributors JO, HS, MaK and HH-R conceptualised and designed the study, carried out the initial analyses, drafted the initial manuscript, and reviewed and revised the manuscript. JO, HS, HH-R and JP collected the data. JP and MiK participated in the design of the study, reviewed the initial data collection and initial analyses, and critically reviewed and revised the manuscript. ML designed the data analysis instruments, coordinated and supervised data analysis, and critically reviewed the manuscript. All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
Funding This study received a grant from The Finnish Medical Society Duodecim.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This is a register-based study approved by the Institutional Review Board of Helsinki University Hospital (§24/2020).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Deidentified participant data are available upon reasonable request from heini.harve-rytsala@hus.fi.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.