Article Text

Abstract
Introduction Excessive administration of antibiotics to preterm infants is associated with increased rates of complications. The purpose of the study was to evaluate the effect of an antimicrobial stewardship intervention on antibiotic use in extremely preterm infants.
Design, setting, patients and intervention A before and after study of infants born at ≤28 weeks’ gestational age was performed in the neonatal intensive care unit of Queen Silvia’s Children’s Hospital, Gothenburg, Sweden. Retrospective analysis of the baseline period (January–December 2014) guided the development of a limited antimicrobial stewardship intervention. The intervention consisted of updated local guidelines with a focus on shortened and standardised treatment duration plus increased access to infectious disease consultant advice. It was fully implemented during the intervention period (October 2017–September 2018).
Objective Primary aim was to compare antibiotic use, defined as antibiotic treatment days per 1000 patient-days, between the two periods, and the secondary aim was to evaluate the number of days with meropenem-based regimens before and after the intervention.
Results We included 145 infants with a median birth weight of 870 g and median gestational age of 26 weeks. The baseline period comprised 82 infants and 3478 patient-days, the intervention period comprised 63 infants and 2753 patient-days. Overall antibiotic use (treatment and prophylaxis) was 534 versus 466 days per 1000 patient-days during the baseline and intervention periods, respectively. Antibiotic treatment days decreased from 287 to 197 days per 1000 patient-days. The proportion of meropenem-based regimens was 69% versus 44%, respectively. No increases in mortality or reinitiation of antibiotics were seen.
Conclusions Implementation of a limited antimicrobial stewardship intervention anchored in analysis of previous prescription patterns can contribute to safe decreases in antibiotic use in extremely preterm infants.
- neonatology
- microbiology
- data collection
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Antibiotics are indispensable in the care of new-born infants, but excessive use is associated with increased complications. Antimicrobial stewardship interventions can reduce inappropriate antibiotic treatment.
What this study adds?
A limited antimicrobial stewardship intervention contributed to reduced use of meropenem-based therapy in extremely preterm infants with a very high risk of neonatal sepsis.
Introduction
Sepsis and other bacterial infections are frequent in neonatal intensive care of preterm infants. Babies that weigh <1500 g at birth (very low birth weight) have on average 1.2 episodes of suspected sepsis during their first months of life, and 15% suffer from confirmed late-onset sepsis.1 The prevalence of infections is even higher in extremely low birthweight infants (birth weight <1000 g), with confirmed bloodstream infections occurring in around 40%.2 Timely administration of antibiotics is important, but the symptoms and signs of infection in neonates are non-specific. This leads to high levels of antibiotic consumption in neonatal intensive care units,3 associated with increased rates of complications4–6 and a risk of emergence of multidrug-resistant organisms.7–9 Antimicrobial stewardship programmes in neonatal units have been introduced around the world,10–14 but published results of stewardship programmes for extremely preterm infants, where the complication and infection rates are highest, are scarce.
Objectives
The primary aim was to determine the extent of antibiotic use and compare the number of treatment days during two study periods before and after implementation of an antimicrobial stewardship intervention for extremely preterm infants, born at ≤28 weeks’ gestational age. The secondary aim was to evaluate the impact of the antimicrobial stewardship intervention on the use of meropenem, a carbapenem-class antibiotic.
Methods
Study design and participants
This was a before and after study of an antibiotic stewardship intervention for the treatment of systemic infections in extremely preterm infants, in a low-resistance setting. The antibiotic stewardship intervention was guided by a retrospective baseline surveillance of antibiotic use, which also served as historical control period. The outcome was evaluated by a repeated retrospective surveillance of antibiotic use in patients admitted during the first 12 months after the stewardship intervention was fully implemented. The retrospective baseline surveillance was conducted during 2016 with evaluation and guideline design during early 2017. The programme was implemented on 1 September 2017 after a due process of review and approval by neonatology staff and leadership. Retrospective surveillance of the intervention period was performed in the second half of 2018. During the time between the study periods, no systematical changes of clinical practice regarding treatment or infection control were performed.
The main outcome measure was total days with antibiotic treatment for infection. Secondary outcomes were adequate duration of treatment and number of days with meropenem-based antibiotic treatment.
Infants born at ≤28 weeks’ gestational age, admitted to the study unit, were included. Exclusion criteria were: immediate transition to palliative care following initial resuscitation (to avoid random effects on mortality not related to treatment) and incomplete electronic medical records. The neonatal unit at Queen Silvia’s Children’s Hospital, Sahlgrenska University Hospital, Gothenburg, Sweden is a level III, 38-bed ward including a 14-bed intensive care unit. The unit provides level III care for Region Västra Götaland (population 1.7 million). Pregnant women with preterm labour at less than 28 weeks of gestational age are transferred to the adjoining delivery room prior to delivery if possible. Patients return to regional units when the clinical situation is stabilised and they have reached a corrected gestational age of >28 weeks.
The background antibiotic resistance is low in Sweden. Nationally, methicillin-resistant Staphylococcus aureus made up 1% of invasive S. aureus isolates during the study period, while 3%–8% of invasive Escherichia coli and Klebsiella isolates produced extended-spectrum beta-lactamases (ESBL).15 Rates in paediatric patients were similar.16
Data collection
We did a retrospective baseline surveillance of all antibiotics (prophylactic and treatment) that were administered to all infants born at ≤28 weeks’ gestational age, who were admitted during 2014 (1 January–31 December), which constituted the control period. The retrospective surveillance process was then repeated after the antimicrobial stewardship intervention was fully implemented, including all infants born at ≤28 weeks’ gestational age admitted between 1 September 2017 and 31 August 2018, which constituted the intervention period.
Each infant’s electronic medical record was reviewed for details on intravenous antibiotic use; blood culture results; results of other relevant cultures; clinical symptoms at initiation and relevant blood chemistry results. At the time of the study, key parts of the medical records were recorded on paper and subsequently scanned to electronic format after patient discharge. Background information on infants was also registered. Respiratory distress syndrome (RDS) was defined as respiratory distress with typical radiological findings and bronchopulmonary dysplasia (BPD) as the need for supplemental oxygen at 36 weeks’ corrected gestational age. Patent ductus arteriosus was defined as having received medical or surgical treatment of ductus, and necrotising enterocolitis (NEC) as NEC stage ≥2A based on the modified Bell NEC staging criteria.17
Antibiotic treatment episodes were classified as: (1) culture-positive sepsis, bacteraemia with a recognised pathogen and clinical symptoms; (2) sepsis with coagulase-negative Staphylococcus spp (CoNS), bacteraemia with CoNS and fulfilled Yale-criteria for CoNS infection18; (3) culture-negative infections, negative or absent blood cultures but fulfilled criteria for clinical sepsis according to Lindquist et al (signs of infection (apnoea, bradycardia, gastric retention or hypothermia) with ≥1 of the following: interleukin (IL)-6 ≥1000 mg/L in infants less than 3 days of age, IL-6 ≥100 mg/L in infants ≥3 days of age, C reactive protein ≥20 mg/L, white cell count <5 x 109/L or >30 x 109/L),19 documented skin infection, thrombophlebitis, NEC or other confirmed diagnosis; (4) unconfirmed infection, not fulfilling any of the above criteria.
Early-onset infection was defined as treatment started <72 hours of birth and late-onset infection as treatment started >72 hours of birth.
Length of antibiotic treatment was counted in days. A date with any intravenous antibiotic was counted as 1 day, regardless of the number of different antibiotics used during that day. When the infant received only one dose of antibiotics on a specific date, it was counted as 1 day of antibiotic treatment. Any antibiotics provided after transfer out to a level II unit were not included in the study. Patient-days was calculated as the number of days from date of admission to the neonatal ward at the study unit, up to date of discharge or transfer to a level II unit. Total antibiotic exposure was then calculated as the total number of treatment days divided by the total number of patient-days for all included patients.
Baseline procedures
Recommended first-line treatment for early-onset sepsis was penicillin G plus an aminoglycoside. For late-onset sepsis, the recommended first-line treatment was cloxacillin plus an aminoglycoside, with vancomycin substituted for cloxacillin in extremely preterm infants. Escalation of therapy to meropenem-based regimens was performed at the discretion of the treating neonatologist. In cases with severe clinical presentation (hypotension with signs of insufficient organ perfusion or suspected NEC) and low gestational age (<28 weeks), first-line empirical treatment consisted of meropenem plus vancomycin. Fluconazole was added prophylactically to all patients born <27 weeks’ gestational age who had central catheters or were treated with antibiotics. Cloxacillin prophylaxis (50 mg/kg administered two times per day) was recommended to all included patients with central catheters.
Blood cultures were compulsory before initiation of intravenous antibiotics. Lumbar puncture was performed if meningitis was suspected. Catheter removal was recommended in infections with S. aureus, Candida spp or gram-negative rods.
The indication for empirical antibiotics was clinical sepsis and defined symptoms of infection and ≥1 of the following: IL-6 ≥1000 mg/L in infants less than 3 days of age, IL-6 ≥100 or rising in infants ≥3 days of age or C reactive protein ≥20 mg/L.
There were no site-specific treatment protocols for confirmed, culture-positive sepsis or other defined clinical infections during the baseline period. Decisions on adjustments of antibiotics and treatment length were made at the discretion of the attending neonatologists.
Antimicrobial stewardship intervention
The study team consisted of three of the authors, of whom one was a neonatologist (EH) and two were infectious disease specialists (MS, LG). Detailed guidelines outlining drug choice and duration of treatment were developed, informed by the retrospective surveillance data. We focused on key areas that we could align with national guidelines and evolving international management traditions.20 21 The intervention-specific updated guidelines are presented in tables 1 and 2. The updated guidelines were implemented following approval from the department head and the medical staff of the unit. The intervention commenced at a specific date after thorough information to the staff. During the study period, the study team met regularly with a focus on surveillance of the need of further education of the staff. The attending neonatologists retained the right to choose empirical therapy and to escalate therapy to more broad-spectrum regimens at their discretion, throughout the study period.
Clinical practice and recommendations for extremely preterm infants (<28 weeks’ gestational age)
Guidelines on antimicrobial choice and treatment duration for confirmed infections
Statistical analysis
Continuous variables were compared with the Mann-Whitney U test and proportions with Χ2 test (two-tailed). Univariate linear regression was used to analyse serial observations. We used a multivariable linear regression model to control for confounding. A p value of <0.05 was considered significant. IBM SPSS V.25 software and the OpenEpi online statistical calculator (www.OpenEpi.com) were used for the calculations.
Patient and public involvement
No patient or public involvement was part of this study, which was initiated and led by the clinical research team.
Results
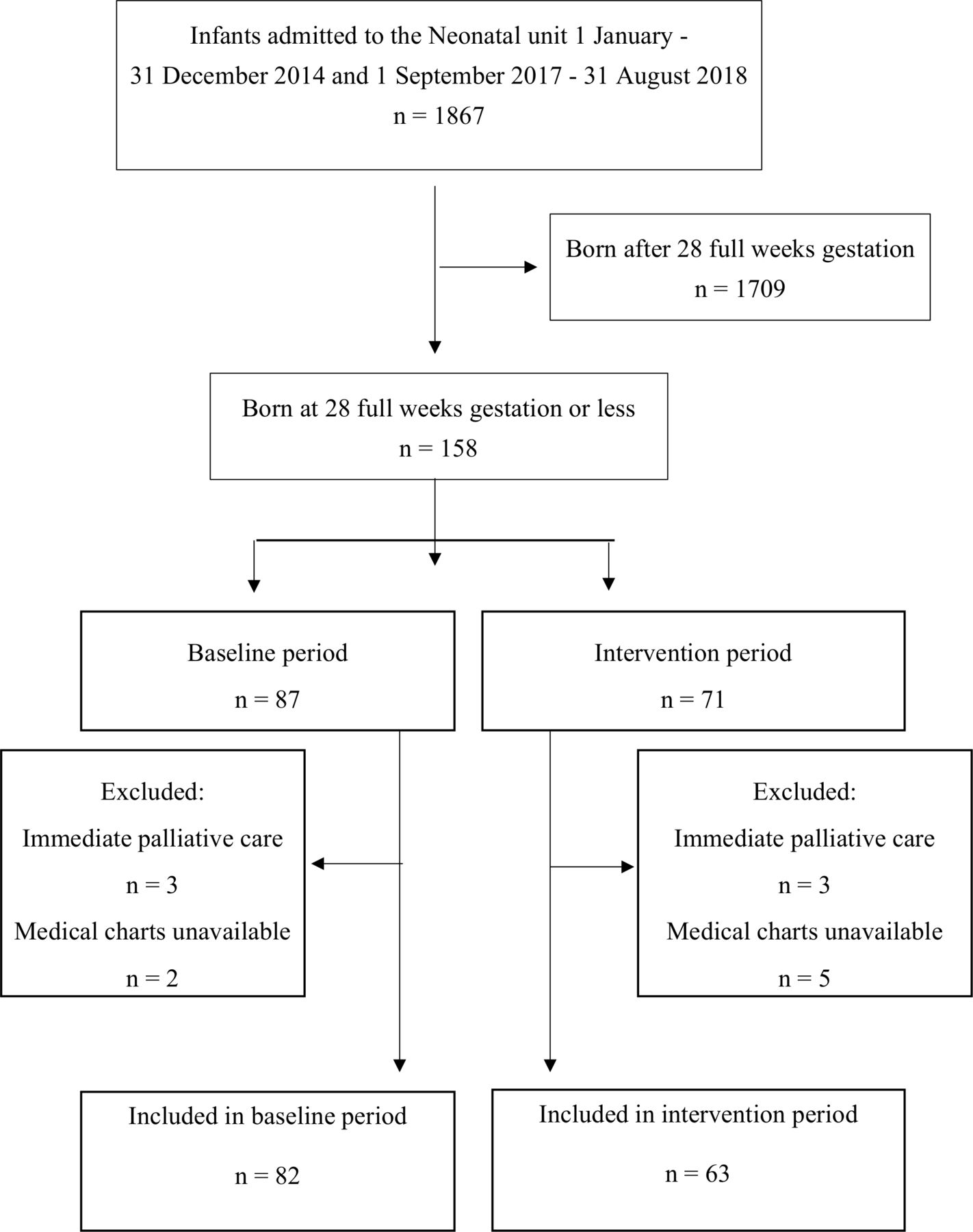
There were 1867 infants admitted to the neonatal unit during the two observation periods. Of these, 158 infants were born at 28 full weeks’ gestation or less (n=87 during the baseline period, n=71 during the intervention period) and constituted the sample population (figure 1). The majority of the patients were born at the study unit, but a few were born at other hospitals and transferred into the study unit after birth. A number of patients were transferred out to a level II regional unit before discharge home, 44/82 (54%) during the baseline period and 32/63 (51%) during the intervention period. Any antibiotics provided after transfer out to a level II unit were not included in this study. In the baseline period, five infants were excluded from analysis (three because of immediate palliative care after initial resuscitation; two because medical records were partially unavailable due to a lack of scanned paper charts). In the intervention period, eight infants were excluded (three because of immediate palliative care after initial resuscitation, five because medical records were partially unavailable due to a lack of scanned paper charts). We were able to include 145 infants in the analysis and their characteristics are presented in table 3. There was an observation of more early deaths (within 24 hours) during the baseline period that did not reach statistical significance. Fewer infants had RDS during the intervention period. Fewer infants developed BPD, among those who could be evaluated (n=122; 23 patients were moved to level II units without electronic records before BPD could be diagnosed). No outbreaks or infections with multiresistant bacteria were noted during the baseline and intervention periods.

Flow chart of included patients.
Characteristics of patients in baseline and intervention periods
The outcome data are presented in table 4. The total antibiotic use decreased from 534 to 466 antibiotic prophylaxis and treatment days per 1000 patient-days between the baseline and intervention periods. The intervention was targeted at antibiotic use for treatment, however, where we observed 90 treatment days less per 1000 patient-days, corresponding to a 31% decrease in antibiotic use. We found a statistically significant reduction in early reinitiations compared with the baseline period. The majority of treatment episodes were for late-onset neonatal infections (>72 hours after birth). Although the proportion of short treatments (<5 days) increased significantly, average treatment duration was similar in both periods for most infection types. Shorter treatment duration overall and for blood culture-negative infections were noted during the intervention period, but did not reach statistical significance (p=0.08 and 0.10, respectively). Antibiotic treatment days per patient-day fluctuated during the study periods, but without tendency to increase over time (figure 2). The number of lumbar punctures performed did not change between baseline and intervention periods (data not shown). Two infants had microbiologically confirmed meningitis, one during the baseline period (Enterobacter cloacae) and one during the intervention period (Ureaplasma spp).

Antibiotic use for treatment per month during the baseline period, January–December 2014 (left) and intervention period, October 2017–September 2018 (right). The slope is non-significant in both periods (p=0.56 and p=0.71, respectively).
Outcome data for baseline and intervention periods
To adjust for differences in severity of preterm complications, we performed a multivariable regression analysis that included variables with a univariate p value of <0.3 together with gestational age and duration of hospital stay (table 5). The intervention period remained independently associated with fewer days of antibiotic use in this model, with an adjusted estimate of 4.9 days less per infant. As expected, a higher gestational age at birth reduced the number of antibiotic days (around 3 days less per week) while a longer length of stay was associated with increases (1 more day with antibiotics per 4 days in hospital).
Multivariable model for the number of antibiotic treatment days per patient
The results for different antibiotic types are presented in figure 3. There were significant decreases in the number of treatment days per 1000 patient-days for meropenem and vancomycin (figure 3A). The distribution of antibiotic types used for treatment was altered, with a lower proportion of meropenem-based regimens and increased proportions of aminoglycosides and other more narrow-spectrum antibiotic types (figure 3B). The proportion of regimens that included vancomycin did not change.

{kind=link}
{kind=link}
{kind=link}
Total use of different antibiotic types for treatment, presented as treatment days per 1000 patient-days. (A) Distribution of antibiotic types used for treatment, presented as the proportion of total treatment days that included each antibiotic type. (B) Note that combination therapy was common and the sum of proportions will be over 100%. #One treatment outlier (prolonged treatment for Ureaplasma meningitis) in the intervention group excluded from figure. ****p<0.0001; ***p<0.001; **p<0.01; *p<0.05; ns, p>0.05.
Discussion
We found that a limited but tailored antimicrobial stewardship intervention with updated management guidelines contributed to a 31% decrease in antibiotic treatment among extremely preterm infants. Furthermore, the proportion of meropenem-based regimens decreased significantly, from almost 70% of treatments given to less than 45%. These changes were achieved without significantly increased use of prophylactic antibiotics or increases in mortality, and with a lower frequency of early reinitiations of antibiotic therapy.
Although our intervention was less comprehensive, the results are similar to previous reports of the effects of antimicrobial stewardship programmes based on updated management guidelines that are tailored to individual neonatal intensive care centres.10 12 Cantey et al reported a 27% overall decrease of antibiotic therapy following the introduction of treatment-duration guidelines.10 However, less than 5% of the study population in that study was born at ≤28 weeks’ gestational age. In another study from the USA, where the intervention was based on daily audits with feedback including treatment recommendations, overall antibiotic consumption was reduced moderately but the reductions in vancomycin and cephalosporins were in line with our figures.13 That study included more extremely preterm infants, although no subgroup analysis for these patients was presented. The present study, which included 145 extremely premature infants, confirms the feasibility of a tailored guideline-based stewardship approach in these high-risk patients. In contrast, Ting et al reported equal or increased inappropriate antibiotic use in very low birthweight infants following an intervention based on daily audits with feedback.22 The stewardship programme in their study used a different set-up and was aimed specifically at inappropriate antibiotic use, maybe explaining the contrasting results. There were still non-significant trends toward shorter average treatment duration and a decrease in the proportion of meropenem, in line with our findings.
The baseline number of treatment days per 1000 patient-days in our study was similar to post-intervention figures in published stewardship studies (245–417 days of therapy per 1000 patient-days),3 10 12 13 whereas we report a comparatively low figure for days of therapy after intervention, despite including only extremely preterm babies. The higher proportion of patients that avoided infection during the intervention period likely contributes to this observation. Other background factors such as antibiotic resistance or health system incentives can also influence antibiotic use, and the different point estimates should be compared cautiously.
There are several reports of vancomycin-reducing guidelines in extremely preterm infants.11 23 Although we did see a significant decrease in vancomycin treatment days (from 190 to 113 days per 1000 patient-days), our intervention was not directed specifically at vancomycin use. Swedish neonatal units have been spared of outbreaks with vancomycin-resistant bacteria, instead, there have been large outbreaks of ESBL-producing gram-negative rods.24 25 Although multi-resistant gram-negatives are a dominant cause of resistance outbreaks in neonatal units globally,26 27 there are still few reports of programmes aimed at reducing the use of antibiotics with gram-negative activity in neonates.14 22
The present study revealed a significant reduction of meropenem-based regimens following the intervention, partly explained by the lack of confirmed gram-negative bloodstream infections during the follow-up period. The proportion of meropenem-based treatment remained high after implementation of the updated guidelines, indicating a potential for further improvements in the rational use of antibiotics at our institution. In addition, the rate of lumbar punctures did not increase as expected and remains an obstacle to optimal treatment. To investigate this apparent lack of adherence to guidelines requires a qualitative approach that is beyond the scope of the present study.
The number of treatments was lower during the intervention period. A lower rate of early reinitiations of antibiotics contributed to this decrease. Although not a part of the stewardship intervention, this could still be related to the changes of management. Already during development, antibiotic stewardship programmes can affect the handling of infections.18 In the study by Nzegwu et al most of the reduction occurred before the programme was implemented.13 Clearly defined treatment duration may reduce the risk of unresolved infections.28 Increased adherence to infection control procedures may also contribute to a lower frequency of late-onset sepsis.29
The effects of antimicrobial stewardship programmes tend to wear off over time.30 To account for this, long observation periods are necessary. Zingg et al reported a yearly decrease of around 3% for a 7-year period.31 Other studies report sustained effects for at least 4 years.13 We did not have access to several years of data, but analysed monthly changes to identify trends. Although there were large fluctuations between months, they appeared to be random and there was no significant increase over time.
Fewer infants in the intervention group developed BPD. Even though this is consistent with earlier observations that prolonged use of antibiotics is associated with increased odds of BPD,6 many other factors could have influenced the reduction of BPD. We used a pragmatic definition of BPD without oxygen reduction tests, as proposed by Walsh et al.32 Less severe preterm complications might affect the threshold for antibiotic treatment,33 and the importance of adjusting for confounders in stewardship evaluation studies has recently been stressed.34 To adjust for differences in common complications and duration of stay, we included a multivariable regression model in the analysis. Admission during the intervention period remained independently associated with 5 days shorter total duration of antibiotic treatment. This estimate is not easily comparable to published reports that have not included such models.
There are limitations to the present study. The definitions of infection types and preterm complications were based on retrospective review of medical records and not on standardised prospective data collection. The limited sample size makes the data vulnerable to random changes in the incidence of infections. There were no confirmed gram-negative infections during the intervention period, which may affect the choice of therapy and treatment durations. The follow-up time was restricted to 1 year, which may be too short to evaluate the durability of the stewardship intervention. We used a metric (days with treatment) that does not account for changes in the spectrum of antimicrobial activity. The intervention was concentrated on a few key updates of management, and we did not include a standard-of-care neonatal unit as control. The overall results may represent a general effect of ongoing quality improvement rather than specific effects of the intervention. Improved diagnostics and reviewed indications for empirical antibiotics may be more effective approaches for reduced antibiotic use. Universally accepted definitions for culture-negative sepsis-like infections in neonates, especially for extremely preterm infants, are lacking.35 This makes it difficult to evaluate and compare guideline changes for this common clinical entity. Roughly half the antibiotic consumption in this patient group at our unit was for prophylaxis. The intervention did not target this use, potentially reducing the effectiveness of the present stewardship initiative. Finally, even though tailored antibiotic stewardship programmes may be specific for each institution, the process of developing and implementing local stewardship initiatives has beneficial effects that are likely to appear in many different settings.
Conclusion
We recorded a significant reduction of antibiotic treatment days following the implementation of a limited antimicrobial stewardship intervention for extremely preterm infants. The reduction was achieved without increases in adverse outcomes and appears safe, despite a majority of patients being very low birthweight infants with a high risk of prematurity complications. This study confirms the feasibility of antimicrobial stewardship interventions in high-risk populations. Further studies of targeted antimicrobial stewardship initiatives are needed to systematically address the practice of antibiotic prophylaxis, as well as high meropenem use in neonatal units.
References
Footnotes
Contributors LG collected and structured the data, performed initial analyses, drafted the initial manuscript, and reviewed and revised the manuscript. SL collected and supervised data, and reviewed the manuscript for important intellectual content. AE contributed to the study design, and critically reviewed and revised the manuscript for important intellectual content. EH and MS conceptualised and designed the study, supervised data collection and structure, and reviewed and revised the manuscript. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Funding All phases of the study were supported by The Region Västra Götaland research funds (grant number FoU-reg 551631). It was also financed by grants from the Swedish state under the agreement between the Swedish government and the county councils, the ALF-agreement (117 661).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the Regional Ethical Review Board in Gothenburg, Sweden (no. 869-15).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The datasets generated and/or analysed during the current study are not publicly available due to that the ethics committee specifically state that no data, which can identify a patient, can be publicly available.