Article Text

Abstract
Objective Young febrile infants represent a vulnerable population at risk for serious bacterial infections (SBI). We aimed to evaluate the diagnostic accuracy of components of the complete blood count in comparison with C-reactive protein (CRP) to predict SBI among febrile infants.
Design and setting Prospective cohort study conducted in a tertiary emergency department between December 2018 and November 2019.
Patients We included febrile infants ≤3 months old with complete blood count results. We analysed their white blood cell count (WBC), absolute neutrophil ratio (ANC), neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio, mean platelet volume to platelet count ratio, and compared these to the performance of CRP.
Main outcome measures SBIs were defined as urinary tract infection, bacteraemia, bacterial meningitis, sepsis, pneumonia, skin and soft tissue infection, bacterial enteritis, septic arthritis or osteomyelitis.
Results Of the 187 infants analysed, 54 (28.9%) were diagnosed with SBI. Median values of WBC, ANC, NLR and CRP were significantly higher in infants with SBI: WBC (13.8 vs 11.4×109/L, p=0.004), ANC (6.7 vs 4.1×109/L, p<0.001), NLR (1.3 vs 0.9, p=0.001) and CRP (21.0 vs 2.3 mg/L, p<0.001), compared with those without. CRP had the best discriminatory values for SBI, with area under the curve (AUC) of 0.815 (95% CI 0.747 to 0.883), compared with WBC, ANC and NLR. A predictive model consisting of WBC, ANC and NLR in combination with clinical parameters, had an AUC of 0.814 (95% CI 0.746 to 0.883). There was increased discriminative performance when this predictive model was combined with CRP, (AUC of 0.844, 95% CI 0.782 to 0.906).
Conclusion In young febrile infants, CRP was the best discriminatory biomarker for SBI. WBC, ANC and NLR when used in combination have potential diagnostic utility in this population.
- microbiology
- neonatology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Identifying young febrile infants at risk for serious bacterial infections is a significant diagnostic challenge.
Biomarkers including white blood cell count, absolute neutrophil count, C-reactive protein and procalcitonin are frequently evaluated in clinical prediction models.
Other aspects of the complete blood count including neutrophil to lymphocyte ratio, platelet to lymphocyte ratio and mean platelet volume to platelet count ratio have been described as promising predictive biomarkers of sepsis in adults, but have not been widely studied in the infant population.
What this study adds?
C-reactive protein (CRP) remains the most valuable discriminating biomarker for serious bacterial infections among young febrile infants.
In the absence of CRP, low cost and readily available biomarkers, including white blood cell count, absolute neutrophil ratio and neutrophil to lymphocyte ratio, when used in combination have potential diagnostic value in the evaluation of this population of febrile infants.
Introduction
Febrile infants under 3 months of age represent a significant proportion of annual emergency department (ED) attendances.1 An estimated 10% of febrile infants under 60 days will have serious bacterial infections (SBI), including urinary tract infection (UTI), bacteraemia and bacterial meningitis.1–3 Invasive bacterial infections (IBI) are commonly defined as the presence of bacteraemia and bacterial meningitis.4–6 SBIs and IBIs, if not promptly treated, can result in mortality, long-term cognitive deficits and hearing loss.7 8 While prompt identification and treatment of sepsis in this group is crucial, these young infants often present with vague symptoms without a clear focus of infection. Clinicians are faced with the diagnostic dilemma of whether the infant has an SBI or a self-resolving viral infection. They often end up routinely performing invasive investigations such as blood sampling and lumbar puncture, and have a low threshold to start empirical broad spectrum antibiotics.
Biomarkers that have been studied include white blood cell count (WBC), absolute neutrophil count (ANC), C-reactive protein (CRP) and procalcitonin (PCT). These markers have been evaluated in clinical prediction rules, used often in combination or together with clinical findings, to risk stratify febrile infants.9–12 However, PCT is not widely available in many settings owing to cost, and has been reported to have wide variations in its sensitivity and specificity.13 14
There has been increasing interest in different aspects of the complete blood count as an easily available and low-cost test. Neutrophil to lymphocyte ratio (NLR) was first reported by Zahorec to reflect the intensity of the immune response to systemic inflammation, surgical stress or sepsis in critically ill adult patients.15 In adult studies, it can predict the presence of bacteraemia and poor outcomes in patients with sepsis.16–18 A few studies have found NLR to be valuable in diagnosing paediatric and neonatal sepsis, alongside other widely used blood markers including ANC and CRP.4 19 20
Platelet and lymphocytes derangements are also measures of systemic inflammation. Mean platelet volume to platelet count ratio (MPV/PC) has been suggested in adult studies as an early prognostic marker of outcome in critically ill states secondary to sepsis or trauma.18 21 Platelet to lymphocyte ratio (PLR) is another novel biomarker, reflecting the balance between inflammation and thrombosis. It has been shown to be useful in adult studies to diagnose inflammatory conditions.18 22 However, these markers have not been as widely studied in the paediatric population.
The primary aim of our study was to investigate the diagnostic accuracy of these easily available biomarkers to predict SBI: WBC, ANC, NLR, PLR, MPV/PC and to compare them with CRP in febrile infants less than 3 months old. Our secondary aim was to determine cut-off values for these biomarkers that would be useful to risk stratify young febrile infants.
Methods
Study design and setting
We performed a prospective observational cohort study, between December 2018 and November 2019, at the ED of KK Women’s and Children’s Hospital (KKH) in Singapore. KKH is the larger of two tertiary paediatric centres in Singapore, with an annual ED attendance of approximately 150 000 children, aged between 0 to 17 years of age.
Study population
We recruited infants if they met the following inclusion criteria: (1) ≤90 days of age, and (2) presented with fever, defined as an axillary or rectal temperature of ≥38°C either at triage (measured by the triage nurse) or during consultation (measured by the doctor), when wrapped in a single layer. We excluded (1) infants without complete blood count results, (2) preterm infants <35 weeks gestation, (3) infants with perinatal asphyxia or significant neonatal complications requiring prolonged stay (>7 days) in the neonatal intensive care unit, (4) those who received antibiotics in the preceding 48 hours and (5) those with underlying haematological or immunological disease. In our hospital, all febrile infants younger than 3 months are hospitalised, forming a natural pool with complete outcomes documented. Subsequently, the type and extent of investigations are decided by the ward physicians. It is usual practice for neonates less than 28 days old with fever to undergo blood, urine and cerebrospinal fluid (CSF) cultures. However, older infants may undergo more limited investigations depending on clinical assessment. All infants are monitored in hospital and are reviewed by medical doctors twice a day or more depending on their clinical status, until the fever has resolved for at least 24 hours before they are discharged.
Definitions and outcome measures
We classified infants with serious bacterial infection as (1) UTI, defined by the growth of a single organism with (a) at least 50 000 colony-forming units (CFU)/mL from a catheterised urine specimen, (b) 10 000 to 50 000 CFU/mL from a catheterised specimen in association with an abnormal urinalysis (positive for leucocyte esterase, nitrite or pyuria with >5 white blood cells per high-power-field on urine microscopy) or (c) at least 100 000 CFU/mL from urine collected via a voided specimen,23 24 (2) bacteraemia, defined by the growth of a single bacterial pathogen in the blood, excluding growth of bacteria considered to be likely contaminants such as coagulase-negative staphylococcus,9 25 (3) bacterial meningitis, defined by the growth of bacteria in the CSF,26 27 (4) sepsis defined as documented or suspected infection and findings of inflammation such as haemodynamic instability, tissue perfusion alteration and/or indications of end-organ dysfunction,28 that demonstrated clinical improvement after fluid resuscitation and early antibiotic administration, (5) pneumonia defined on chest X-ray as reported by a trained radiologist, (6) bacterial enteritis confirmed by a positive stool culture, (7) infection of skin and soft tissues (cellulitis or similar), diagnosed by suggestive physical examination findings or (8) osteomyelitis or septic arthritis. In addition, we included in the definition of bacterial meningitis, infants with either (1) bacteraemia with an organism known to cause central nervous system infection and sterile CSF pleocytosis,26 27 or (2) sterile CSF pleocytosis with biochemical changes consistent with bacterial meningitis including CSF to plasma glucose ratio of less than 0.6, with no other attributable source of infection. For cases where chart review was unclear, a consensus was reached by consulting the infectious diseases specialist. CSF pleocytosis was defined as (1) CSF white blood cells ≥20 cells/uL for infants ≤28 days or ≥10 cells/uL for infants 29 to 90 days of age with (2) CSF red blood cells<100 cells/uL.26 27 IBI was defined by bacteraemia or bacterial meningitis.4–6 Infants were included in the non-SBI group if they had: (1) negative cultures or (2) demonstrated clinical improvement defined as resolution of fever and symptoms without a complete workup. The final diagnoses were determined after an independent review of the patients’ clinical course and investigations by a trained clinician.
We obtained demographic data, clinical history and physical examination, laboratory investigations including complete blood count, CRP, PCT, blood cultures, urine cultures and lumbar puncture investigation results from the electronic medical records. The complete blood count was determined using an automated haematology analyser (Sysmex XN-1000 and XN-3000, Kobe, Japan). Total white cell count with differential count was measured using flow cytometry method, while platelet count was determined using impedance method. CRP measurement was performed using a quantitative immunoturbidimetric assay (Alinity c analyser, Abbott Laboratories, Italy). From the complete blood count, we retrieved data including WBC and platelet count, ANC, absolute lymphocyte count and MPV. NLR was calculated as the ratio of neutrophils to lymphocytes, PLR as the ratio of platelets to lymphocytes and MPV/PC as the ratio of MPV to platelet count.
Statistical analysis
All data were entered into a Microsoft Excel database. Statistical analysis was performed using IBM SPSS Statistics, V.26 and SAS software, V.9.4 (SAS Institute Inc). At baseline, categorical variables were summarised as counts and percentages (%), and continuous variables as mean and SD or median and IQR. Continuous variables were assessed for normality using q-q plots and histograms. After applying a normalising log transformation on variables with right-skewed distributions, the normality assumption was found to be tenable. Statistical comparisons between groups on normal and normalised variables were performed using a two sample t-test. In addition, variables with right-skewed distributions were compared using a Wilcoxon rank-sum test. Categorical variables were compared using Fisher’s exact test.
We performed a univariate analysis for each potential predictor and presented these using unadjusted OR estimates, with 95% CIs. In the multivariable analyses, we studied the performance of the specific variables of interest that were statistically significant on univariate analysis (complete blood count indices WBC, ANC and NLR) and adjusted for age of the infant, gender and duration of fever before presentation. We derived predictive models with and without CRP to address the primary aim of the paper. Adjusted OR (aOR) were presented with their corresponding 95% CIs and statistical significance was taken at p<0.05. We presented discriminative ability using the area under the receiver operating characteristic (ROC) curve (AUC) analyses and optimal cut-off values were calculated using the Youden’s index (sensitivity+specificity −1). We compared the area under the ROC curves for significant differences, using DeLong’s method.29
Results
Among 203 febrile infants recruited, 187 were included in the final analysis (figure 1). There were no significant differences in baseline characteristics between the included and excluded patients in this study (online supplemental eTable 1).
Supplemental material
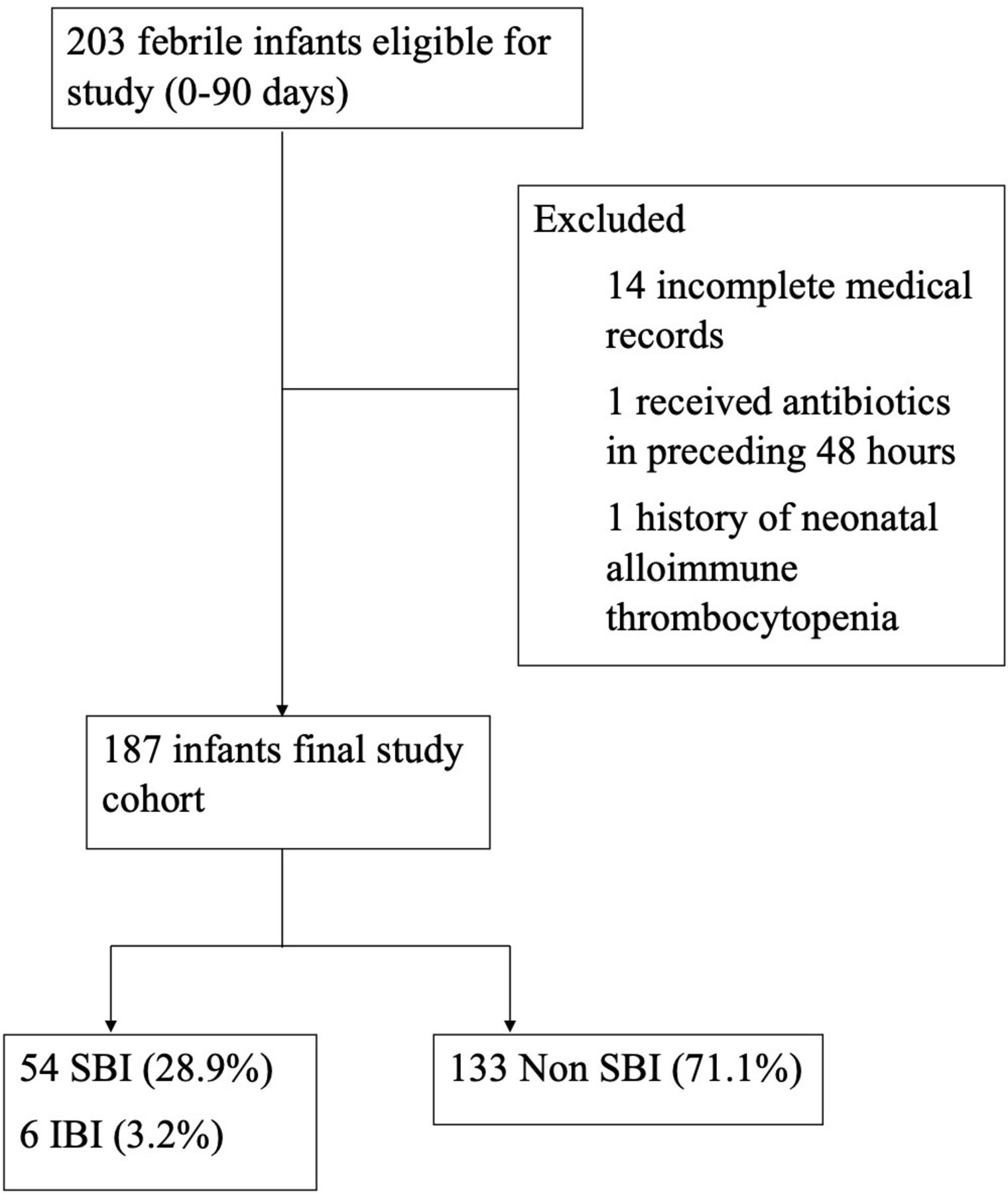
Patient flow diagram. IBI, invasive bacterial infections; SBI, serious bacterial infections.
Only one patient was discharged against medical advice and all other infants were hospitalised. Seventeen (9.1%) infants received intravenous fluid bolus in the ED, while 1 (0.5%) required intensive care. The majority had urine cultures (158, 84.4%), blood cultures (153, 81.8%) and lumbar punctures for CSF analysis (121, 64.7%). Most received intravenous antibiotics (153, 81.8%).
Table 1 describes the demographic and clinical characteristics of the SBI and non-SBI group. The overall median age at presentation was 35 days (IQR 9 to 61). Thirty-six (19.3%) infants were born to mothers with Group B Streptococcus (GBS) colonisation, among whom 35 (97.2%) received treatment for GBS.
Clinical and laboratory characteristics of infants with and without serious bacterial infections
Mean and median values of WBC, ANC, NLR and CRP were significantly higher in infants with SBI compared with those without (table 1). When comparing infants with IBI to those without IBI, only PLR was significantly higher: PLR (149.7, IQR 88.2 to 250.5, vs 86.0, IQR 68.6 to 114.4, p=0.038). The median value of MPV/PC did not differ significantly when comparing infants with SBI and IBI to those without (p=0.768 and p=0.065 for SBI and IBI, respectively).
Fifty-four infants (28.9%) were diagnosed with SBI, and 6 (3.2%) with IBI. UTI was the most common SBI (36, 66.7%), of which Escherichia coli (29, 80.6%) was the most common pathogen. The second most common SBI was sepsis (12, 22.2%). The main causative organism for bacteraemia was GBS, while cases of meningitis were largely secondary to Klebsiella pneumoniae, Escherichia coli and GBS. The prevalence of each SBI in various age groups is detailed in table 2.
Diagnoses of serious bacterial infections in each age group
WBC, ANC, NLR and CRP were significantly associated with SBI in the univariate analysis (table 3). In the multivariable analysis without CRP, WBC (aOR 0.730, 95% CI 0.540 to 0.986) and ANC (aOR 2.318, 95% CI 1.245 to 4.315) were significant. However, when CRP was added to the model, only ANC (aOR 1.934 (95% CI 1.007 to 3.714) and CRP (aOR 1.037, 95% CI 1.013 to 1.063) were statistically significant.
Univariate and multivariate analysis (with and without CRP) of clinical and laboratory predictors of infants with serious bacterial infections
CRP had the best discriminatory values for SBI, with AUC 0.815 (95% CI 0.747 to 0.883), followed by ANC and NLR, with AUC 0.681 (95% CI 0.587 to 0.775) and AUC 0.656 (95% CI 0.571 to 0.740), respectively (table 4). Sensitivities, specificities, likelihood ratios and positive and negative predictive values of the various biomarkers based on optimal cut-offs are also presented in table 4. At the cut-off of 7.2 mg/L, CRP had the highest sensitivity of 75.47% (95% CI 61.72 to 86.24) and negative predictive value of 88.29% (95% CI 68.27 to 92.44) for SBI. Using this optimal cut-off value of CRP, 13 (24.1%) infants with SBI and 2 (33.3%) of infants with IBI were not diagnosed accurately. These missed cases of SBI included 7 (53.8%) infants with urinary tract infection, 1 patient with bacterial meningitis and 1 patient with concomitant GBS bacteraemia and GBS meningitis.
Sensitivity, specificity and likelihood ratio values of biomarkers for discrimination of serious bacterial infection at optimal cut-offs
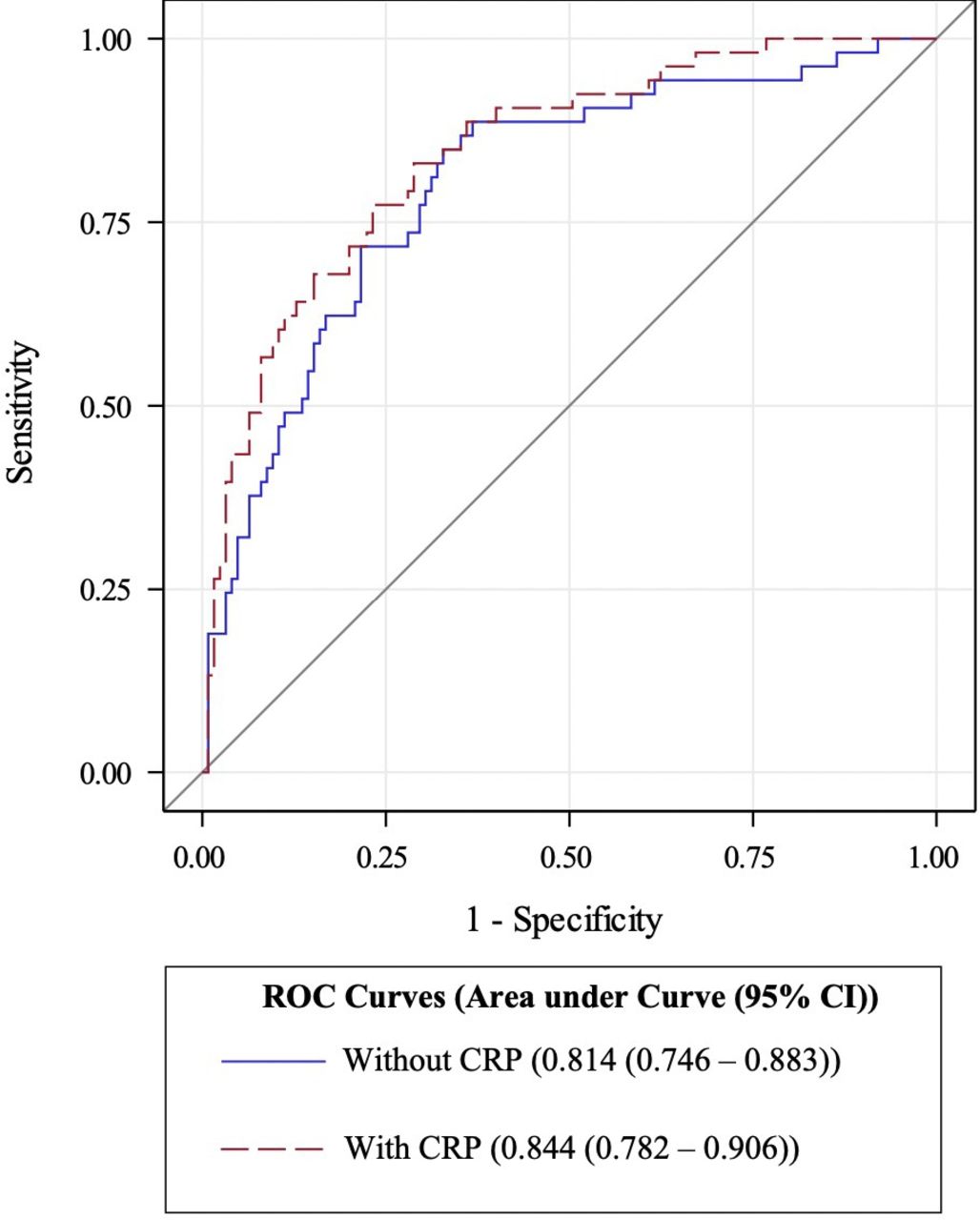
The optimal cut-off values based on Youden’s index for WBC, ANC and NLR are 13.83 x 109//L, 6.37×109/L and 1.24, respectively (table 4). Using clinical parameters with these complete blood count biomarkers (WBC, ANC and NLR) in a predictive model, we derived an AUC of 0.814 (95% CI 0.746 to 0.883). When CRP was added to this predictive model, there was significantly improved discriminative performance with an AUC of 0.844 (95% CI 0.782 to 0.906) (p=0.046) (figure 2).

{kind=link}
{kind=link}
Receiver operating characteristic (ROC) curves for demographic predictors and complete blood count biomarkers with and without C-reactive protein (CRP) for discrimination of serious bacterial infections.
Discussion
We described the predictive value of WBC, ANC, NLR, PLR and MPV/PC, and compared these to CRP in discriminating SBI in the young infant population. Our study shows that CRP had the best performance as a discriminatory biomarker for infants with SBI. Within the complete blood count, ANC performed better than NLR. We found no significant difference in platelet markers including PLR and MPV/PC between the two groups. We demonstrated that although WBC, ANC and NLR did not perform satisfactorily as independent predictors, when used in combination they could potentially value-add to the clinician’s armamentarium when predicting SBI. When these biomarkers were used together with CRP, there was improved discriminative performance.
The reported prevalence of SBI in literature varies widely, from 7.1% to 26%.3 4 9 11 12 30 Our study reports a relatively high prevalence of SBI of 28.9%. This is likely due to our broad case definition of SBI, including clinically significant cases of bacterial infection such as pneumonia, skin and soft tissue infection, bacterial enteritis and sepsis with associated haemodynamic instability that responded to fluid resuscitation and early antibiotic administration. Culture-negative sepsis, in particular in early onset sepsis, is well described in the neonatal population, possibly due to small volumes of blood obtained for culture, low levels of bacteraemia or fastidious bacteria.31–34 Our study found UTI to be the most common SBI, similar to reported literature.4 9 11 12 We did find that those with SBI tended to be older, with the highest prevalence reported in the 29 to 60 days age group, which differs from larger studies that report that infants with SBI were more likely to be 28 days or younger.2 9
Screening tools described in literature often use a combination of various blood biomarkers for risk stratification of febrile infants. Recent validated sequential algorithms and clinical prediction rules to aid in identification of young febrile infants at risk of serious bacterial infections often include PCT, which is not routinely available as a point of care test in many settings and is costly.9 12 Although PCT is known to have superior accuracy as a diagnostic marker for SBI, its reported sensitivity and specificity in literature is variable likely due to heterogeneous study populations and differing cut-off values.13 14 The use of PCT alone is reported to be inferior to available clinical prediction rules for identifying febrile infants at risk for SBI.13 We evaluated components of the complete blood count as fast, easily available and relatively low cost biomarkers. Out of these, only WBC, ANC, NLR had statistically significant higher median values for infants with SBI compared with those without. ANC had the best performance with AUC of 0.681 (95% CI 0.587 to 0.775). However, comparison with CRP showed that CRP had significantly better performance as a discriminatory biomarker, with AUC of 0.815 (95% CI 0.747 to 0.883). This finding concurs with previous studies which describes CRP as the most discriminatory biomarker for young infants with SBI, as compared with components of the complete blood count.4 5 35 The performance of WBC, ANC and NLR in our study, however, was poorer compared with previously reported studies.4 35
In our study, at the optimal cut-off level of 7.2 mg/L, CRP had a reasonably high sensitivity of 75.47% (95% CI 71.72 to 86.24) and negative predictive value 88.29% (95% CI 68.27 to 92.44). This cut-off value is much lower compared with values used in other predictive models for discrimination of SBI in young infants, which are in the range of 20 to 46.1 mg/L.4 10–12 This may be due to the majority of infants in our cohort presenting early with less than 24 hours of fever, as Singapore is highly urbanised with rapid hospital access. Our study suggests that a lower CRP cut-off might be necessary to distinguish infants with SBI during early onset of symptoms. CRP is known to rise 4 to 6 hours after the onset of symptoms and peak 24 to 48 hours later.36–38 This is similarly demonstrated in our study, where even at the optimal cut-off level, 13 (24.1%) infants with SBI and 2 (33.3%) of infants with IBI were incorrectly classified. Of note, a 77-day-old infant among these had GBS bacteraemia and GBS meningitis, who presented with an initial CRP of 1.8 mg/L. This further highlights the pitfall of relying on a single biomarker for identifying febrile infants at risk of SBI, especially early in the course of illness.
The value of CRP as a good discriminatory biomarker is demonstrated in our study by the improved performance of a predictive model with clinical parameters and complete blood count biomarkers after its inclusion, with an AUC of 0.844 (95% CI 0.782 to 0.906). Hamiel et al similarly found that in the assessment of SBI among young febrile infants, CRP combined with either ANC or NLR offered improved discriminative ability.4 However, in the absence of CRP, we found that the predictive model with clinical parameters, WBC, ANC and NLR performed with a reasonable AUC of 0.814 (95% CI 0.746 to 0.883). This suggests that there may be clinical utility in combining these indices in the discrimination of SBI, when CRP is not available.
Strengths and limitations
We performed a prospective study analysing a combination of these biomarkers including NLR, PLR and MPV/PC in this age group, thus adding value to previous retrospective reports.4 5 35 Unlike most studies looking at only SBIs such as UTI, bacterial meningitis and bacteraemia,4 9 25 35 we also included other important SBIs in our analysis, such as cases of sepsis, pneumonia, bacterial enteritis and skin infection which have clinical implications.
We recognise the limitations of our study. Not all infants underwent a full evaluation to look for bacteraemia, UTI and meningitis, which may have resulted in potential missed occult bacterial infections. However, we are confident that these numbers are small, since it is our hospital protocol that all young febrile infants undergo strict inpatient monitoring of their temperature and vital parameters for at least 24 hours before discharge. Infants are only allowed to be discharged if they remained well with no fever or clinical evidence of serious bacterial infection during this period of observation, and after repeated medical assessment. We did not document the timing of vaccinations (if at all) administered to these infants, which may have affected levels of CRP.39 40 While we tried to adjust for possible confounders through suitable exclusion criteria and with a multivariate analysis, we were not able to adjust for all possible confounders that would affect values of WBC, ANC, NLR and CRP, including maternal fever and causes of stressful delivery. We had small numbers of IBI, resulting in this subpopulation being underpowered for the analysis. Future larger prospective studies will be needed to validate these results, especially among infants with IBI.
Conclusion
In a population of febrile infants under 3 months of age, we found that CRP was the single best biomarker for distinguishing SBI. In the absence of CRP, we demonstrated that low cost and readily available biomarkers including WBC, ANC and NLR can add diagnostic utility when used in combination. There may be a role in the combination of these biomarkers with clinical findings to aid in risk stratification and subsequent management of young febrile infants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Conceptualisation: S-LC, GO, SSYC, RP. Data curation: SSYC, RP, AZL, S-LC. Formal analysis: S-LC, JCA, SSYC. Methodology: SSYC, S-LC, GO, JCA, KCN, IM. Supervision: S-LC, GO, JCA, KCN, IM. Writing – original draft: CSYS, AZL. Writing -review and editing: SSYC, AZL, S-LC, GO, JCA, KCN, IM. Approval of final manuscript: SSYC, AZL, S-LC, GO, JCA, RP, KCN, IM.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethics approval was given by the SingHealth Institutional Review Board E (2017/2680) and documented informed consent was obtained from parents or legal guardians for all patients recruited for the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Individual participant data that underlie the results reported in this article, after de-identification (text, tables, figures and appendices) can be shared with researchers who provide a methodologically sound proposal. Proposals should be directed to chong.shu-ling@kkh.com.sg.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.