Article Text

Abstract
Background In the UK setting, where neonatal jaundice treatment is required, it is largely carried out in hospitals. However, it is possible to safely administer home phototherapy (HPT).
Objective To report on our centre’s experience of HPT and its potential benefits.
Design Retrospective observational study performed as a service evaluation.
Patients Infants ≥35 weeks corrected gestational age with a weight of 2 kg and serum bilirubin ≤50 µmol/L above treatment thresholds. Controls were a matched group of infants who received inpatient phototherapy (IPT).
Setting The catchment area of two neonatal intensive care units, one special care unit and a birth centre at four different hospitals that is covered by a single neonatal community outreach nursing team in Birmingham, UK.
Intervention HPT was started either in the community or as a continuation of IPT. Controls received IPT.
Main outcome measures The rate of bilirubin reduction, hospital readmission rates and parental satisfaction.
Results 100 infants received HPT while 50 received IPT. No infant showed a progressive rise of serum bilirubin level while receiving HPT. The rate of bilirubin reduction was similar in both HPT and IPT groups (2.4±1.9 and 2.5±1.6 µmol/L/hour, respectively, MD=−0.1, 95% CI −0.74 to 0.53, p=0.74). Readmission rate was 3% in the HPT group. 97% of parents stated that the overall experience was good and 98% would choose HPT if they had their time all over again.
Conclusion Our programme suggests that HPT for neonatal jaundice can be carried out in a select group of infants. It helps in providing holistic family-centred care and is viewed positively by families.
- jaundice
- neonatology
Data availability statement
Data data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Inpatient phototherapy is routinely used to treat neonatal jaundice.
Although home phototherapy is commonly used in other countries such as the USA, it is rarely used in the UK.
No high-quality evidence is currently available to support or refute the practice of home phototherapy in the UK.
What this study adds?
Phototherapy can be delivered at home in a select group of infants and could be an ideal option during the COVID-19 pandemic.
It can be as effective as inpatient phototherapy, potentially prevent occupancy of acute beds and help in delivering family-centred care.
It is well received and positively viewed by parents.
Background
Jaundice is almost universal in newborn infants and, where treatment is required in the UK setting, it is generally undertaken in hospital. However, it is possible to safely administer home phototherapy (HPT) for jaundice in patients’ own homes.1 2 This practice has been accepted as an alternative to inpatient phototherapy (IPT) in several high-income countries such as the USA where it is accepted practice.3 4
HPT helps to prevent prolonged hospitalisation and re-admission. It can promote mother–infant bonding and lead to increased parental satisfaction.5 While the existing published studies have focused on the efficacy of HPT, they rarely commented on parents’ satisfaction. Patients’ experience is an important and commonly used indicator for measuring the quality of service in healthcare. There is increasing evidence that it is positively associated with clinical effectiveness and patient safety.6 7 It is also a measure of patient-centredness, one of the six healthcare quality aims proposed by the Institute of Medicine.8 Patient satisfaction affects clinical outcomes, patient retention and is linked to improved compliance with clinician’s instructions, timely care seeking, greater comprehension and retention of information.9
Our HPT service was set up in 2018 and is now supported by a 7-day neonatal community outreach nursing team (NCOT) and one consultant. We report on our centre’s experience of the HPT service and analyse the outcomes for infants treated at home.
Methods
Setting
The Birmingham Heartlands Hospital NCOT covers a large catchment area with around 18 000 deliveries per year. The area covers a tertiary neonatal intensive care unit (NICU), special care unit and birth centre in three different hospitals which are part of the University Hospitals Birmingham National Health Service (NHS) Foundation Trust and another NICU at Birmingham Women’s Hospital.
Population
We included all infants who received HPT. The eligibility criteria for HPT were infants with corrected gestational age (CGA) ≥35 weeks, weight ≥2 kg, ≥48 hours of age and serum bilirubin (SBR) ≤50 µmol/L above treatment thresholds according to The National Institute for Health and Care Excellence (NICE) guidelines.10 Infants in the control group were CGA matched, ≥48 hours old and received single phototherapy as per hospital policy. To be eligible for HPT, parents needed to be able to converse in English, follow instructions regarding the use of HPT equipment and have a satisfactory home environment. Infants with severe haemolytic jaundice, SBR level >50 µmol/L above treatment thresholds, age of <48 hours and infants whose parents were not conversant in English were ineligible for HPT.
Data were collected retrospectively from infants’ medical records over the period from April 2018 to September 2020 for HPT and from January 2019 to September 2020 for IPT. For consistency, the total duration of phototherapy was calculated using the timing of bilirubin level before HPT started to the timing of bilirubin level when HPT stopped.
Intervention
HPT was delivered using a NeoMedLight BiliCocoon Bag system device (figure 1). The irradiance of BiliCocoon was 35 μW/cm2/nm.11 IPT was delivered via Dräger Bililux with irradiance of >33.5 μW/cm2/nm at 50 cm.12 HPT could be a continuation of IPT or commenced in the community. Infants referred from the community needed initial clinical examination by a clinician in hospital, repeat SBR, conjugated bilirubin, full blood count and direct Coombs test (DCT).

BiliCocoon bag system used for home phototherapy.
Parents were taught to use the phototherapy equipment, signed written consent for HPT use and received a feedback sheet to complete at the end of treatment. The NCOT visited daily to review infants and perform serum SBR. Once SBR level was ≥50 µmol/L below the treatment threshold, HPT was stopped and a rebound level taken 12–24 hours later. If satisfactory, the device and feedback form were collected.
Parental feedback
The feedback form consisted of two types of questions. The initial part sought to determine parental experiences through a series of closed questions. These questions were structured to allow for a ‘yes’ or ‘no’ response, with a space provided for additional comments if needed. The second part of feedback sought to discover the personal experiences and opinions of parents about the HPT service through open questions (see online supplemental file 1).
Supplemental material
Outcomes
The primary outcome was to report on the effectiveness of HPT, represented by the rate of fall of bilirubin and hospital readmission rates. It was also defined as the avoidance of significant rise of SBR that puts infants at risk of kernicterus or readmission for intensive IPT. Secondary outcomes included parental satisfaction and duration of phototherapy.
Statistical analysis
Data were analysed using GraphPad Prism V.8.4.3 (471). Data were presented as mean±SD for normally distributed continuous data and median and IQR for skewed continuous data. Comparison was performed using the χ2 test for categorical data and Student’s t-test or Mann-Whitney U test for continuous data as appropriate.
Patient and public involvement
Patients or the public were not involved in the design, conduct or reporting of our study.
Results
We included 100 infants in the HPT group and 50 infants as controls. Their characteristics are included in table 1. HPT was initiated in the community in 52 (52%) infants, while 48 (48%) infants received it as a continuation of IPT (table 2). The rate of bilirubin fall was similar in both HPT and IPT groups (mean 2.4±1.9 and 2.5±1.6 µmol/L/hour, respectively, MD=−0.1, 95% CI −0.74 to 0.53, p=0.74) (table 1). No infant showed a progressive rise in SBR level in HPT group.
Characteristics, rate of bilirubin fall and duration of phototherapy for infants treated with home phototherapy and control group
Characteristics, rate of bilirubin fall and duration of phototherapy for infants received community-initiated and hospital initiated HPT
The total duration of phototherapy was longer in HPT compared with controls, (mean 43±28 and 26±9 hours respectively, MD=17, 95% CI 9.2 to 25.5, p=0.0001) (table 1). Data on the duration of phototherapy as per the device’s timer were available in 66 (66%) infants in HPT group. The total duration of HPT was significantly longer (mean 40±23 hours) than the durations recorded on the BiliCocoon timer (mean 24±10 hours, MD=15.4, 95% CI 9.2 to 21.6, p<0.0001). The mean duration of stay for IPT group was 51±19 hours. Two infants required more than one session of HPT and three (3%) required readmission. One infant among controls required two sessions of IPT.
Parental experience
Feedback received from 100 families was overwhelmingly positive with 95 (98%) stating that if they had their time all over again, they would still choose HPT rather than IPT, while 2 (2%) preferred IPT (figure 2). Detailed feedback is shown in tables 3 and 4 and figures 2–4).
Parents’ responses to ‘what would you say were the main advantages of letting your baby have phototherapy at home?’
Parents’ responses to ‘were there any disadvantages to having phototherapy at home?’

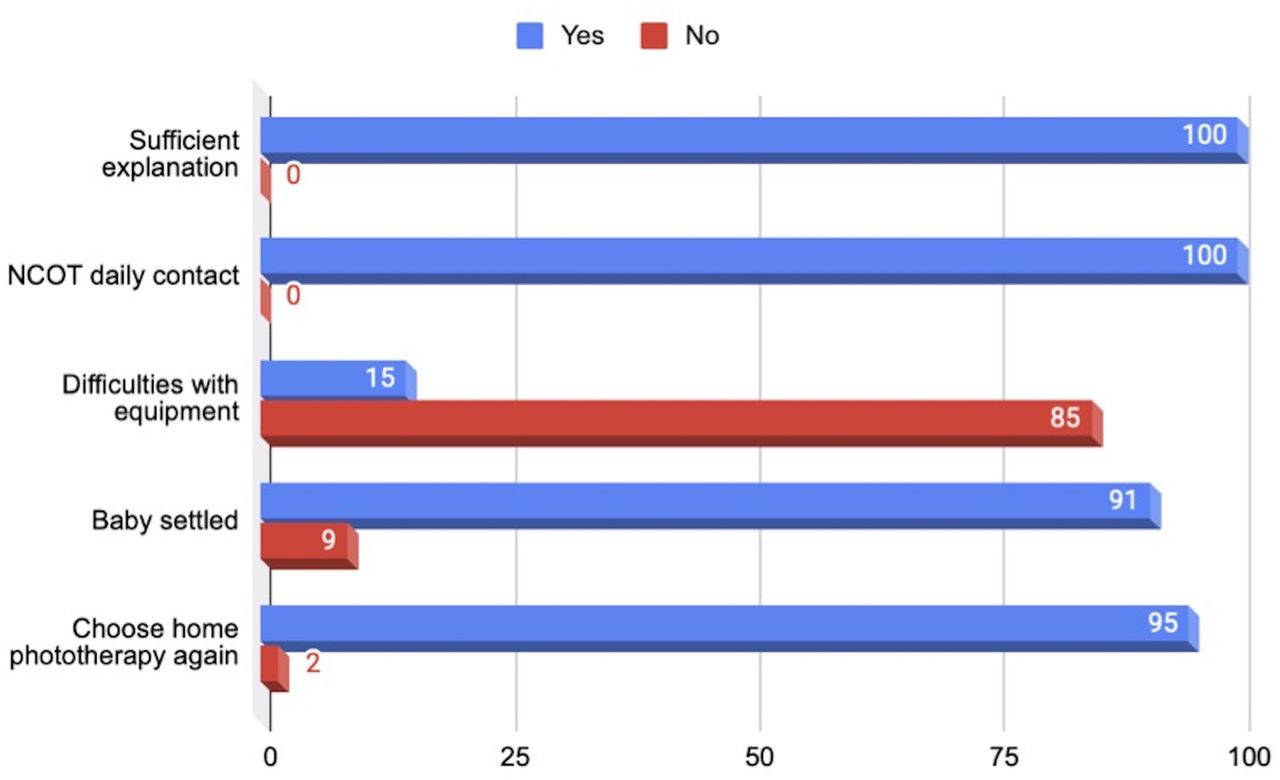
Parental opinions on home phototherapy service. NCOT, neonatal community outreach nursing team.

Overall parental experience of home phototherapy service.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Overall parental rating of home phototherapy service.
Discussion
Few studies have examined the use of HPT. Apart from Chang and Waite, most studies had small sample sizes. Our report adds to the increasing evidence on the effectiveness of HPT.3
The breastfeeding rate in both the HPT and IPT group was similar. In the study of Chang and Waite, breastfeeding rate was much higher at 90%, so breast milk jaundice may have been more prevalent in their population.3
In our HPT group, 8 (8%) were DCT positive; one required two sessions of HPT, none showed signs of haemolysis. Chang and Waite found that although 10% of their cohort were DCT positive, 5.7% required readmission or another session of HPT.3
The duration of HPT in our cohort was shorter (43 hours) when compared with the reports by Chang and Waite (53 hours) and Thakkar et al (57 hours).3 13 When compared with IPT, the duration of HPT was longer. This could be explained by greater parental adherence to treatment due to direct patient supervision and more frequent SBR checks in hospital. This was shown in the longer total duration of HPT compared with the phototherapy unit timer reading. However, IPT (mean 26±9 hours) was of similar duration to HPT as measured by the device timer (mean 24±10 hours). Our findings agree with Slater and Brewer who reported that the duration of IPT was shorter than HPT.14 However, Eggert et al found that duration of treatment was similar in both IPT and HPT.4 On the other hand, Zainab and Adlina reported the duration of HPT was shorter than IPT.15
Effectiveness and re-admissions
The rate of bilirubin reduction was similar in both HPT and IPT groups. No infant in HPT showed a progressive rise in SBR level. Similarly, the meta-analysis done by Chu et al showed that there was no difference in bilirubin reduction rate between HPT and IPT.1 On the other hand, Zainab and Adlina reported the rate of fall was higher in HPT group compared with controls. However, it is unclear whether the devices used for HPT and IPT delivered the same irradiance.15
In our cohort, HPT was successful in the majority of infants with three (3%) readmissions due to concerns over treatment failure and non-compliance. Two infants required more than one session of HPT; one had suspected Gilbert syndrome. Chang and Waite reported a readmission rate of 1.9%. However, they used different treatment thresholds.3 Reducing readmission rates help NICUs maintain available maternity beds for high-risk intrauterine transfers requiring delivery in tertiary perinatal centres. It also reduces bed occupancy on paediatric wards freeing beds for acutely unwell children.
Parental feedback on HPT
In our cohort, the responses to the initial questions in the questionnaire indicated high levels of satisfaction with the service. All parents agreed that staff had sufficiently explained how to use the equipment, and that the NCOT had contacted them daily until 1 day after phototherapy was stopped. Similarly, Jackson et al reported that all parents were highly satisfied that all information concerning the HPT had been supplied to them.16 However, they received feedback from only 28 parents.
A minority of parents in our HPT group did experience some difficulties with the equipment, such as struggling to put the eye masks on their infants and the eye masks slipping during treatment. Similarly, a few parents reported the mask causing discomfort to their baby who then needed frequent picking up in order to settle.
In the second part of the questionnaire, when asked about the main advantages of HPT, the two most common themes in the responses were being in the home environment and around their families. A number of parents expressed relief at not having to be in hospital in order to receive phototherapy. Additionally, having support from other family members and spending time with other children was cited as another advantage. Ease and convenience were also common themes, with several parents noting how simple the equipment was to use. A number of parents cited comfort, both for the baby and themselves, as the main advantage. Similarly, in the study by Jackson et al, 86% of parents reported that HPT always fitted with their family routine.16
For a balanced assessment, parents were also asked to list any disadvantages they had encountered. Eighty-five per cent found no disadvantages with HPT, however, some concerns were expressed. The two main disadvantages were equipment issues, with a few parents finding the equipment bulky and difficult to store, as well as the baby not settling in the HPT unit. A few parents found being responsible for their baby’s care without constant medical supervision anxiety-inducing, and thus did not feel entirely confident.
It is comforting that 95 (97%) parents stated the overall experience of HPT was good and 95 (98%) reported that they would choose HPT if they had to do it all over again and be advocates for the service to other families. Two parents (2%) stated a preference to IPT in future, having found HPT too stressful. Our team has used the few reported difficulties by some parents especially with the eye masks to forewarn future families along with suggestions as to how this could be overcome which could further reduce the parental anxiety this might produce.
Feasibility
Our results show that infants ≥2 kg and ≥35 weeks CGA can be treated with HPT. Zainab et al included infants ≥37 weeks while Chang and Waite only included infants with SBR levels 34-51 µmol/L below treatment thresholds as per the American Academy of Pediatrics (AAP) guidelines.3 15 The NICE treatment thresholds are quite different from the AAP thresholds. Whereas NICE guidelines offer gestation-specific thresholds at weekly intervals up to 38 weeks, the AAP guidelines offer a composite guideline for infants ≥35 weeks. Further, AAP guidelines advise against the use of HPT unless the bilirubin levels are 34-51 μmol/L below the treatment thresholds. In UK practice, phototherapy is commenced if SBR level is above NICE treatment thresholds. So, we included infants who met that criteria that is, infants who normally need admission to hospital for phototherapy, this means infants included in the Chang et al report would not have met the NICE criteria for treatment. It is also possible to treat carefully selected infants with mild haemolysis with HPT.
Infants in the control group could have been candidates for HPT. However, they were not offered HPT due to either (1) the lack of knowledge of junior doctors about HPT especially at the launch of the service and during change over period of new junior doctors, (2) the lack of availability of trained personnel during out of hours to teach parents how to use equipment, (3) parents did not feel confident to use HPT or (4) parents were not conversant in English.
Resource use
The average length of IPT was 51 hours which equates to 2.1 bed days per infant that could be saved. This potentially saves 204 bed days for 97 HPT infants as three (3%) required readmission. This could help in improving patient flow on maternity wards. While a comprehensive economic analysis was outside the scope of this observational study, baseline data from our hospital and the costing of HPT service demonstrated clearly the efficiency of delivering care in this manner. The one-off cost of machinery and ongoing costs of home visits have to be weighed against the costs of occupying acute beds and the difficulties mothers experience when away from their families.17 In light of the COVID-19 pandemic, we need to find different ways of providing care to keep families together and safe.
Considerations for healthcare professionals
Although HPT is a convenient alternative to IPT, it is not suitable for all infants and families. Infants with very high bilirubin levels may not be eligible for HPT due to the lack of direct supervision in the community and the need for intensive IPT. HPT relies on parental compliance and confidence to use the equipment without constant supervision. This requires clear and effective communication, which may be impeded by failure to employ translators where language differences exist.
We sought the feedback of our service users as user feedback is a powerful developmental tool for any service. Measurements of patient satisfaction using appropriately designed and delivered surveys provide robust measures of the quality of care and can help improve services and their delivery.18 On the contrary, dissatisfaction with healthcare leads to poor compliance and in extreme cases, patients resorting to negative word-of-mouth reports that discourage others from seeking healthcare from the system.19 The HPT service perfectly complements the recently launched NHS At Home, a drive to give people more personalised, supported and connected care in their own homes which reduces the need for hospital attendances or admissions.20
Strengths and limitations
To our knowledge, this is the largest cohort of HPT for neonatal jaundice in the UK. Our report not only demonstrates the feasibility of incorporating HPT in UK clinical practice but also is supported by overwhelmingly positive parental experiences.
However, our study is limited by the inherent limitations of retrospective studies. It was not possible to measure the exact duration of HPT. Although the NeoMedLight devices have a timer display which records treatment duration, the data were only available in 66 (66%) cases. The way in which we have measured the duration of HPT likely over-estimated the total duration of HPT. Selection bias may have been introduced in parental feedback because feedback was received from parents who agreed for their infants to received HPT in the first place. However, it is not possible to get feedback about a service from people who did not receive that service.
Conclusion
Our report demonstrates that HPT for neonatal jaundice can be administered in a select group of infants and is viewed very positively by families. It enables mothers and their infants to remain at home receiving family support and could reduce occupancy of acute beds. We would, however, recommend larger prospective studies before adopting the practice across the UK.
Supplemental material
Data availability statement
Data data are available on reasonable request.
Acknowledgments
The authors thank the postnatal wards nursery and neonatal nurses, midwives and the NCOT at Birmingham Heartlands Hospital for their great contribution to the study.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @MONANOURELDEIN
Contributors RM set up the home phototherapy service and conceived the idea of the study. MN and RM designed the study. MN, GM, HM and KP collected and analysed the data, and wrote the first draft of the manuscript. All authors contributed to editing the manuscript and approved it in its final form.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests No, there are no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.