Article Text

Abstract
Objective The aim of this study was to quantify the changes that occurred in the surgical services of children during the COVID-19 pandemic from the perspective of a low/middle-income country.
Design A case–control study was conducted at a large referral centre in Bangladesh among patients aged ≤12 years. Comparisons were made between cases admitted during a period of ‘April to September 2020’ (Pandemic period) and controls during a similar period in 2019 (Reference period). The number of admissions and outpatient department (OPD) attendances, age and sex distribution, diagnosis, number and types of surgeries performed (elective vs emergency), variations in treatment of acute appendicitis, types of anaesthesia and mortality were compared.
Results Admissions were only 41% of previous year (635 vs 1549), and OPD attendances were only 28% of previous year (603 vs 2152). Admission of children reduced by 65.8%, but neonatal admission reduced only by 7.6%. The median age of the admitted patients was significantly lower during the pandemic period (3 vs 4 years, p<0.01). Acute appendicitis (151, 9.8%) and trauma (61, 9.6%), respectively, were the the most common causes of admission during the reference and the pandemic period. Elective surgeries were only 17% and emergency surgeries were 64% of previous year (p<0.01). Appendectomy (88, 9.1%) and laparotomy (77, 17.6%), respectively, were the most common surgeries performed during the reference and the pandemic period. Conservative treatment of acute appendicitis was more during the pandemic period (47.5% vs 28.5%, p=0.01), but patients who underwent appendectomies had more complicated appendicitis (63.3% vs 42.1%, p=0.01). In all, 90.4% of surgeries were performed by resident doctors. There were no COVID-19- related deaths.
Conclusion Trauma became the most common cause of admission during the pandemic, and neonatal surgical conditions remained almost unchanged with high mortality rates. Elective procedures and laparoscopy remained low and resident doctors played a major role in providing surgical services.
- COVID-19
- health services research
- adolescent health
- neonatology
Data availability statement
Data are available upon reasonable request from the following ORCID ID: https://orcid.org/0000-0002-1661-2111.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
The COVID-19 pandemic has changed the management of care around the world. Different centres took different measures to prioritise their pattern of services and keep essential services moving. Surgical care of children was also compromised, but emergency surgery and surgery for malignant conditions did not stop. It was predicted that there would be a reduction in the volume of surgeries, but catastrophic loss of lives would occur in the low/middle-income countries.
What this study adds?
Neonatal admissions did not significantly reduce, and patients had a significantly less median age. Trauma was the most common cause of admission despite the limited movements and outdoor activities. There were more conservative treatments for acute appendicitis. Resident doctors were the key service providers.
Introduction
The COVID-19 pandemic has affected every aspect of life around the world, and children’s surgical condition is no exception.1–4 Many routine surgeries were cancelled, emergency surgical care was also very challenging and patients suffered from limited access to healthcare delivery systems.5–7 In Bangladesh, the first confirmed COVID-19 case was declared on 8 March 2020 and the first COVID-19-related death was reported on 18 March 2020.8 9 As of 1 February 2021, there were 535 139 confirmed cases in Bangladesh, of which 8127 (1.5%) died.10 Bangladesh is the third most affected country in South East Asia after India and Pakistan, and 31st in the world.11
Although it has been observed that children suffered less from COVID-19-related problems, access to surgical care was also restricted in children during this period.5 12 A global survey on children’s surgery providers from 30 low/middle-income countries (LMICs) reported that there was little consensus among respondents on which procedures should be limited or delayed during the pandemic.13 There is also scarcity of report from LMICs about the actual changes during the pandemic on the surgical services to children. The aim of the study was to assess the changes the COVID-19 pandemic brought about on children’s surgical services and to compare surgical activities in children during the COVID-19 pandemic with those during a reference period in a tertiary-level government hospital in Bangladesh.
Materials and methods
Study design and settings
This was a case–control study performed in the Department of Paediatric Surgery, Chittagong Medical College Hospital (CMCH) in Chattogram. Chattogram (former Chittagong) district has the second highest number of COVID-19 positive cases in Bangladesh.14 CMCH is the largest government referral centre for paediatric surgical conditions for about one-fifth of the population in the country. This department deals with patients of paediatric general surgery, paediatric casualty, paediatric urology, neonatal surgery and paediatric oncosurgery. It also provides outpatient and emergency services to surgical children aged ≤12 years. Children with orthopaedic, neurosurgical, cardiac surgical, and burn and plastic surgical problems are usually admitted in the respective adult departments, but some of them are also admitted in this department and transferred there if needed. In Bangladesh, the number of positive cases had increased from April until July 2020 when it began to reduce and reached a plateau at the beginning of October 2020. The number of cases increased again during December 2020.15 To answer the research question regarding changes in paediatric surgical services during the pandemic, we analysed all the children admitted in this department and attended in the outpatient department (OPD) during a period between 1 April and 30 September 2020 (Pandemic period) and compared them with the records of patients of similar period between 1 April and 30 September 2019 (Reference period). Patients of the pandemic period were considered as cases and those of the reference period were the controls. All patients aged ≤12 years who were admitted in the ward or attended in the OPD were included in the study. Patients aged more than 12 years (three during the pandemic period and eight during the reference period) were excluded. Children with surgical conditions who were admitted in other adult surgical departments were also excluded from the study. The specific objectives were to compare the number of admissions and OPD attendances, age and sex distribution, diagnosis, number and types of surgeries performed (elective vs emergency), expertise of surgeons, types of anaesthesia, and number and diseases of mortality between both periods. As a secondary objective, variations between the patterns of treatment of acute appendicitis (conservative vs surgical) and operative findings (uncomplicated vs complicated) were recorded as this remains the most common paediatric surgical condition.16 Complicated appendicitis was defined as operative finding of appendicular perforation, gangrene or abscess formation.
Data analysis
Comparisons were made between groups with regard to sex, age groups (neonates, infants and children), diagnoses among the admitted and OPD patients, types of surgery and anaesthesia. Age was compared using the Jonckheere-Terpstra test. Age group, sex, type of surgery, expertise of surgeon and type of anaesthesia, treatment pattern of acute appendicitis and per-operative findings were compared using χ2 or Fisher’s exact test. Average monthly surgeries between pandemic and control period were compared using Student’s t-test. P value of <0.05 was considered as significant. Statistical analyses were performed using SPSS V.22.
Patient and public involvement
No patient or public involvement was required for this study.
Results
During the pandemic period, a total of 635 patients were admitted in contrast to 1549 admissions during the reference period. Male to female ratios were 1.8 vs 1.9 during the pandemic versus reference period, respectively (p=0.63). The median age of the admitted patients was 3 years during the pandemic period and 4 years during the reference period (p<0.01). Admission of children reduced by 65.8%, but neonatal admission reduced only by 7.6% (table 1). OPD attendances reduced to 603 in the pandemic period from 2152 in the reference period.
Frequency of admission and OPD attendance during the pandemic and the reference period among different age groups
Acute appendicitis was the most common disease among admitted patients during the reference period (151, 9.8%). Trauma was the most common cause of admission during the pandemic period (61, 9.6%), which was followed by acute appendicitis (59, 9.3%) (table 2). The number of admissions for acute appendicitis reduced by 60.9% during the pandemic period. Although trauma cases reduced during the pandemic period (101 vs 61), their relative percentage increased (6.5% vs 9.6%). There was very low admission for inguinal hernia. Neonatal intestinal obstruction (20) became the 10th most common cause of admission during the pandemic period (not shown in table 2). Inguinal hernia was the the most common cause of OPD attendance during both periods (154, 7.2% vs 49, 8.2%) (table 2). OPD attendance for undescended testes and urinary tract infection reduced substantially (table 2). However, vascular anomaly (20) and pelvi-ureteric junction obstruction (12) were among the 10 most common causes of OPD attendance during the pandemic period (not shown in table 2).
Ten most common diseases admitted in the ward and attended in the OPD during the reference period (2019) and their changes during the pandemic period (2020)
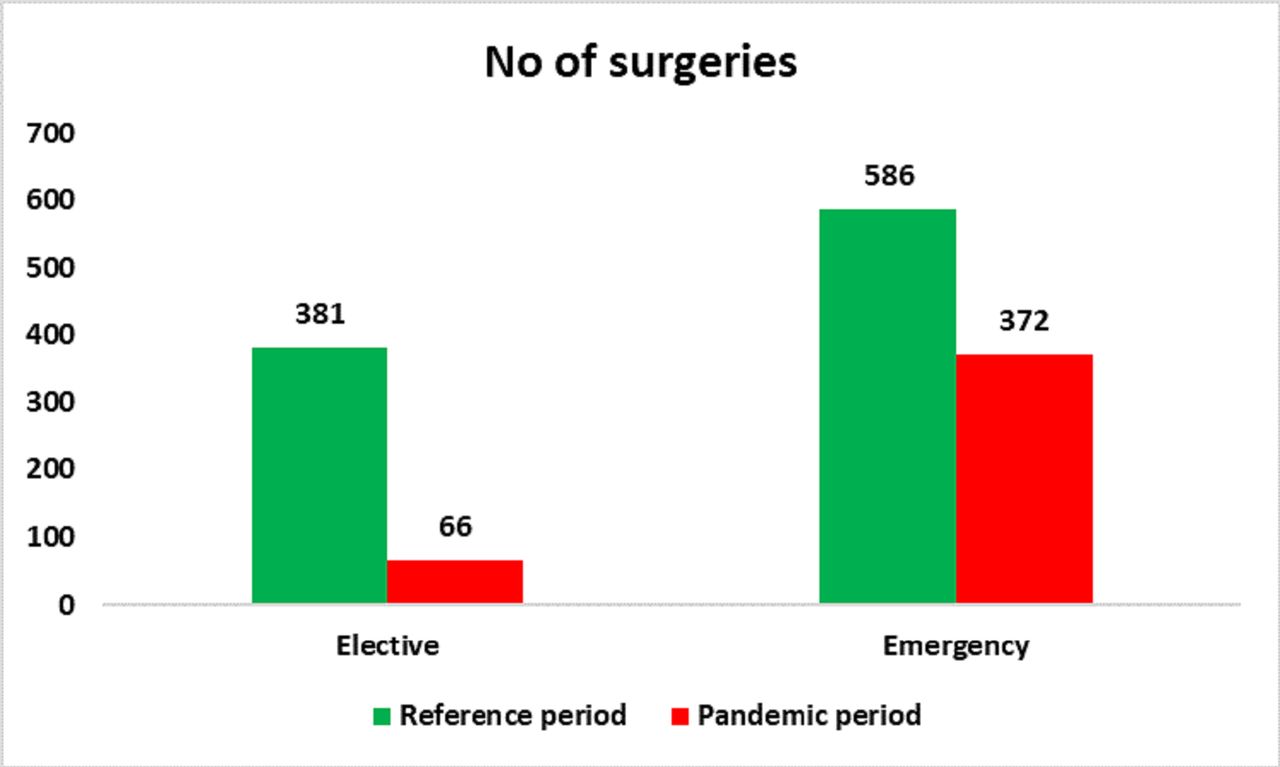
During the pandemic period, 438 surgeries were performed in contrast to 967 during the reference period, which means that there was a 54.7% reduction in surgeries during the pandemic period. However, among the admitted patients, 69.0% underwent surgery during the pandemic period in contrast to 62.4% during the reference period (p<0.01). Elective surgeries were only 17% and emergency surgeries were 64% of previous year (p<0.01) (figure 1). The number of surgeries gradually increased from June onwards during the pandemic period (figure 2). On average, 73 emergency surgeries were performed every month during the pandemic period versus 161 during the reference period (p<0.01). There were 26 laparoscopic procedures during the reference period in contrast to only 3 laparoscopic procedures during the 6-month span of the pandemic period (p=0.01). Cystoscopy procedures were 23 during the reference period and 11 during the pandemic period (p=0.51). Surgeries performed under general anaesthesia were 435 (45.0%) during the reference period in contrast to 179 (40.9%) during the pandemic period (p=0.15). During the pandemic period, 396 (90.4%) surgeries were performed by residents (supervised by consultants who did not scrub) in contrast to 669 (69.2%) during the reference period (p<0.01). Elective surgeries performed by residents were 35 (53.0%) vs 128 (33.6%) during the pandemic and the reference period, respectively (p<0.01).
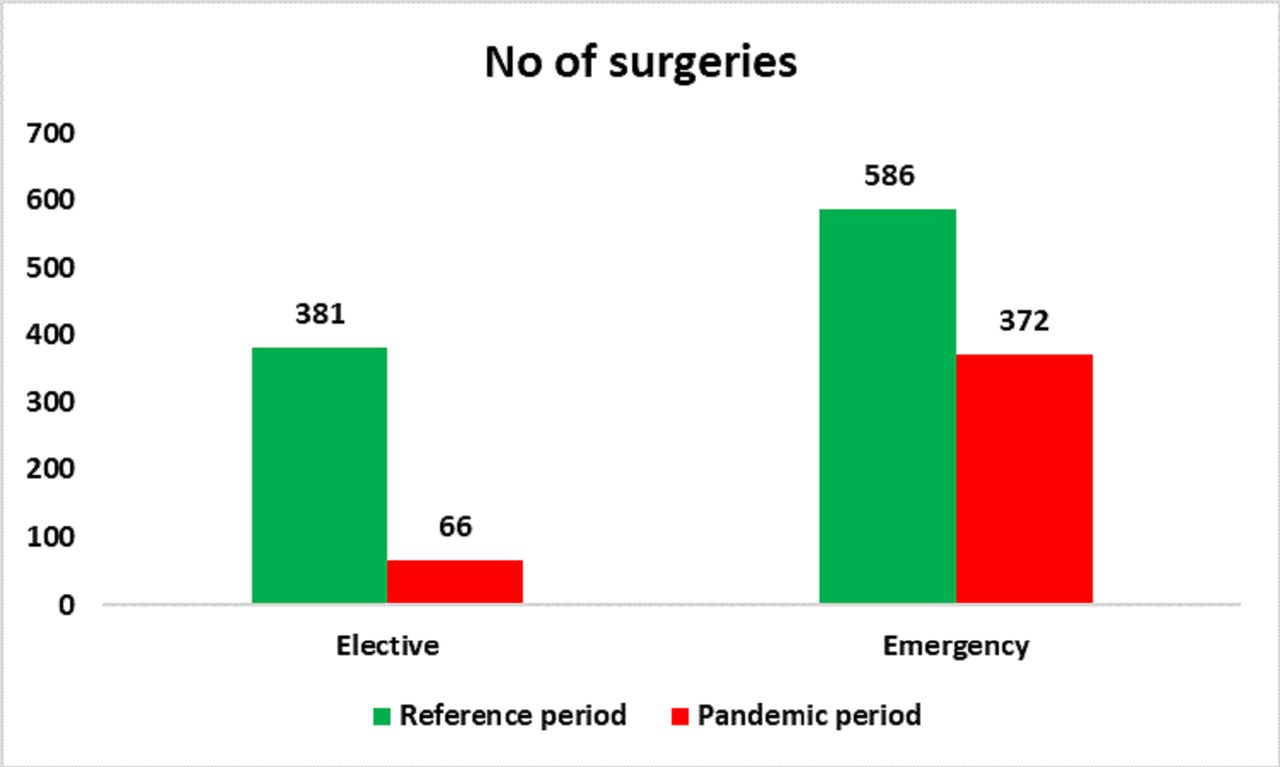
Comparison of number of surgeries performed during the reference and the pandemic period.
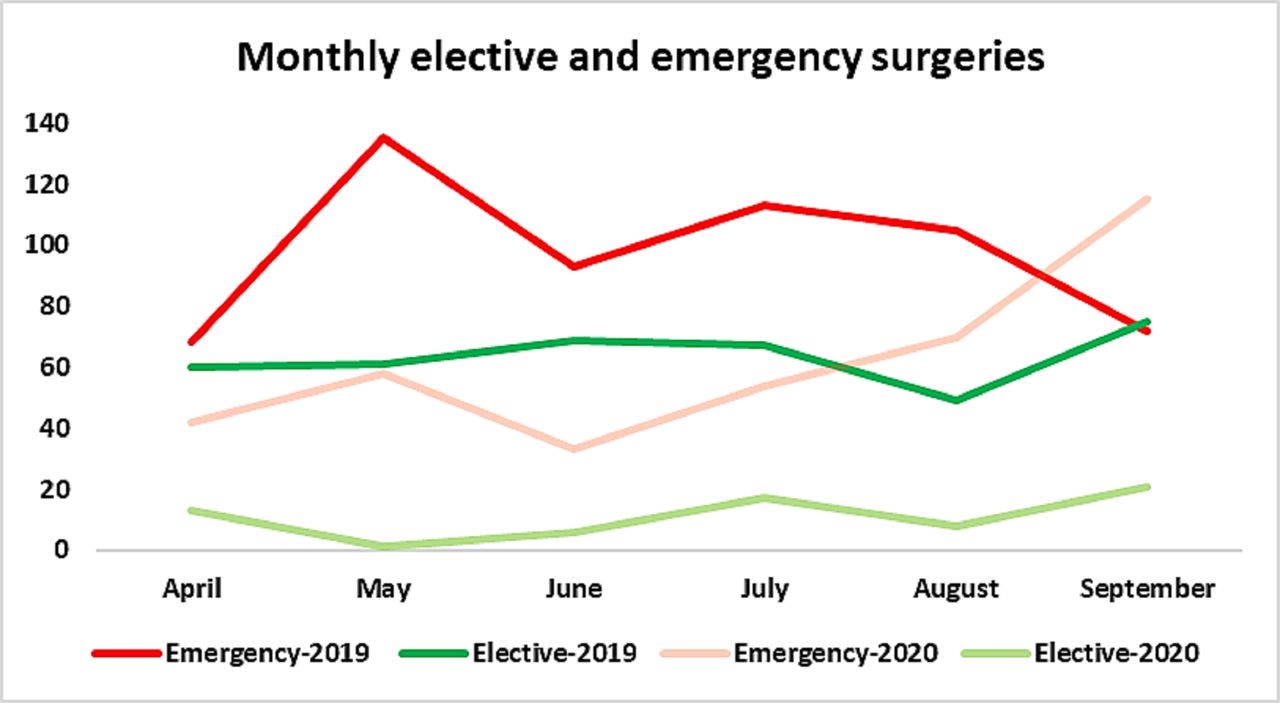
Comparison of monthly volume of elective and emergency surgeries during the reference (2019) and the pandemic (2020) period.
While appendectomy (88, 9.1%) was the most common surgery performed during the reference period, laparotomies for various other causes (77, 17.6%) were the most common during the pandemic period (table 3). In all, 47.5% of the admitted cases of acute appendicitis were treated conservatively during the pandemic period in contrast to 28.5% during the reference period (p=0.01). However, there were more cases of complicated appendicitis (63.3% vs 42.1%, p=0.01) during the pandemic period among patients who underwent surgeries. The number of laparoscopic appendectomies reduced by 85% during the pandemic period.
Major types of surgeries during the reference and the pandemic period
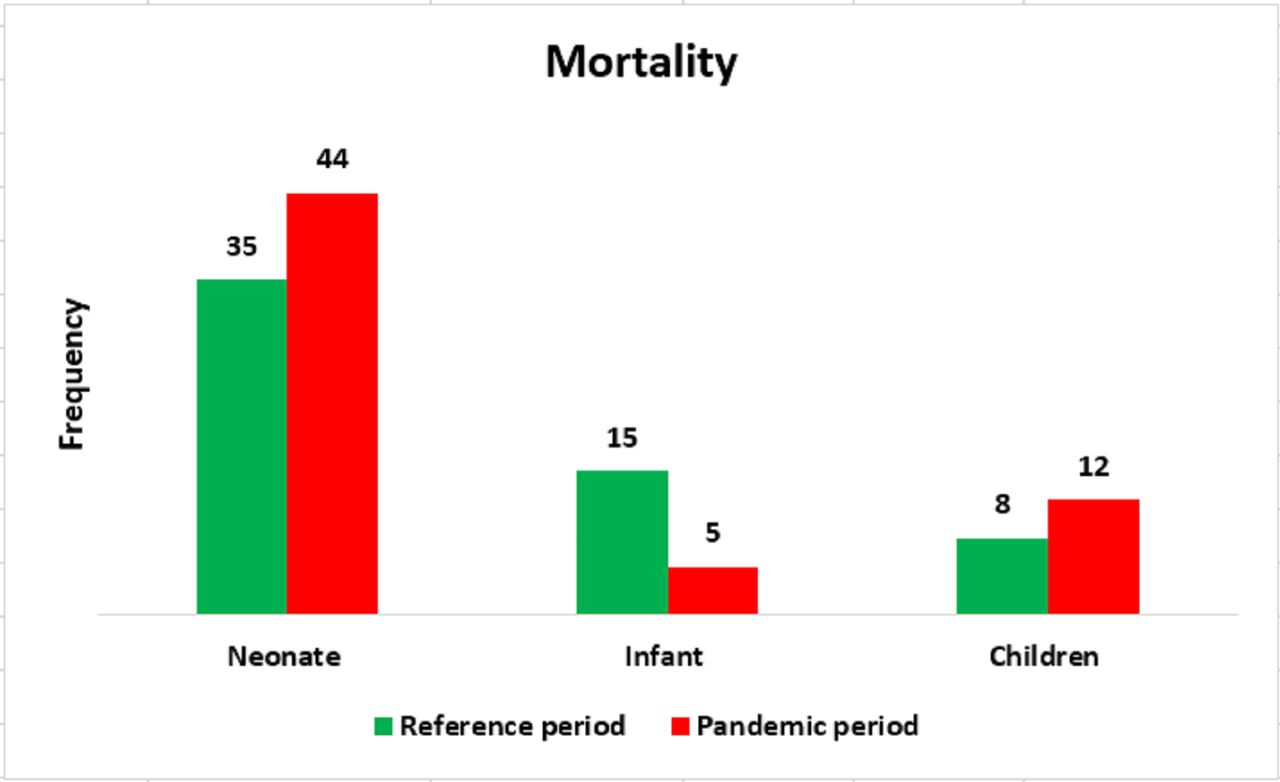
The number of mortalities remained almost similar (61 vs 58) during both periods. There were more neonatal and child deaths but fewer infant deaths during the pandemic period in contrast to the reference period (figure 3). The major causes of mortality during the reference period were intestinal obstructions (19), anorectal malformation (ARM) (5), gastroschisis (5), intestinal perforation (5), posterior urethral valve (5) and omphalocele (3). The major causes of mortality during the pandemic period were intestinal obstructions (29), ARM (8) and gastroschisis (7).
{kind=link}
{kind=link}
{kind=link}
Neonatal, infant and child mortality during the reference (2019) and the pandemic (2020) period.
Discussion
The COVID-19 pandemic affected LMICs later than high-income countries (HICs), and the consequences were less devastating than those of many HICs.17 However, it was predicted differently because of the inability of LMICs to respond aggressively.18 19 The changes in the surgical scenario in children during the pandemic in LMICs have not been adequately reported. This study reports a 59% reduction in admissions, 72% reduction in OPD attendances and 55% reduction in surgeries during the pandemic. These changes were predictable in the context of a pandemic. However, neonatal surgical admissions remained almost similar. Neonates constituted nearly one-fourth of the admitted patients and 72% of all mortalities during the pandemic period. In many LMICs, neonatal surgical care is not adequate and there is a lack of neonatal intensive care unit (NICU), provision of total parenteral nutrition and other necessary adjuncts.20 21 This hospital has an NICU, yet it observed a high neonatal surgical mortality. Birth defects are a major proportion of neonatal surgical conditions, and 94% of global birth defects occur in LMICs.22 23 The unchanged neonatal admission and more neonatal mortalities in a large centre from LMICs re-emphasise the need for improvement of neonatal surgical care in these countries.
Significantly younger babies were admitted during the pandemic period. This alludes to the fact that younger children are more prone to emergency surgical conditions than older children and are more in need of prompt surgical care. Children constitute a large part of the population in many LMICs, reaching about 60% in some.24 However, only 6.3% of all global surgical procedures occur in LMICs.25 This is in the perspective that about 19% of children in low-income countries have a surgical need and 62% of them have at least one unmet need.25 This study showed that although children suffered less from COVID-19, their surgical services had a major setback during the pandemic, making the scenario worse. This pandemic exposed many areas of concerns in provision of child health in LMICs but, at the same time, provided opportunity to improve the healthcare delivery system.24 26
There were changes in the disease pattern among the admitted patients during the pandemic. While acute appendicitis was the the most common disease for admission during the reference period, trauma was the the most common cause of admission during the pandemic period. About 95% of all trauma deaths in children occur in LMICs that have an underdeveloped trauma management system, especially in the emergency care of trauma patients.27 The emergency departments in the majority of the hospitals are not well-equipped and there are delays in acute trauma care. Trauma remained a major cause of morbidity in children during the pandemic despite the reduced number of vehicles in the roads and fewer outdoor activities.
There was an extreme reduction in laparoscopic surgeries during the pandemic period (26 vs 3), and there were no laparoscopies during May and June 2020. It was because of the earlier recommendations at the beginning of the COVID-19 pandemic by the surgical societies to avoid laparoscopy because of the fear of transmission of SARS-CoV-2 through surgical smoke or aerosol.28 29 Although this restriction was later relaxed, laparoscopic procedures remained very low.29 A significantly higher proportion of surgeries were performed by the residents during the pandemic period. Residents also performed a significantly higher proportion of elective surgeries during the pandemic period. However, consultants performed more difficult and time-consuming surgeries.
There was a significant increase in the percentage of conservative treatment for acute appendicitis during the pandemic period. On the contrary, among patients who underwent appendectomies, the majority had complicated appendicitis and it was significantly more than the previous year. There were contradicting findings in this regard around the world.16 30–34 Observations in this study passively suggest that an increase in the conservative treatment of acute appendicitis in LMICs might increase the rate of complicated appendicitis. Although this study did not analyse the reasons for conservative treatment of acute appendicitis, those were not always surgeons’ choice. The observed reasons were parents’ refusal to surgery; signs of resolution after delayed presentation despite ultrasonographic evidence of acute appendicitis; and disappearance of symptoms during the delay in arranging theatre, giving consent or waiting for the availability of anaesthetists.
This study has several limitations. It has the inherent limitations of a retrospective study and it was performed in a single centre. Patients with orthopaedic, neurosurgical, cardiac, burn and plastic surgical conditions were under-represented as a majority of these conditions were admitted in the respective adult surgical departments. However, it quantified some of the changes during the COVID-19 pandemic on the volume and patterns of surgical conditions in children from one of the largest paediatric surgical centres in Bangladesh. It depicts that healthcare workers continued their services even during the very peak hours of the pandemic.
Conclusion
The COVID-19 pandemic brought about major changes in the surgical services to children. Admission, OPD attendance and the volume of surgeries decreased. There were also changes in patterns of admissions, age distribution and types of major surgeries. There were major reductions in laparoscopic procedures. Resident doctors played a major role during the pandemic. There were no COVID-19-related deaths.
Data availability statement
Data are available upon reasonable request from the following ORCID ID: https://orcid.org/0000-0002-1661-2111.
Ethics statements
Ethics approval
Ethics approval was given by the Ethical Review Committee of Chittagong Medical College (Memo: CMC/PG/2020/125).
Acknowledgments
The authors acknowledge the contribution of the residents involved in the original record keeping of the patients.
References
Footnotes
Contributors MAAF was involved in conceptualisation. TKC, AS, MAA and TF were involved in data curation. TKC was involved in formal analysis, methodology, review and editing, and writing the original draft. SMHK was involved in supervision. MAAF and AS were involved in writing the article and review and editing. MAAF and SMHK approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.