Article Text

Abstract
Background Stimulation of non-crying neonates after birth can help transition to spontaneous breathing. In this study, we aim to assess the impact of intact versus clamped umbilical cord on spontaneous breathing after stimulation of non-crying neonates.
Methods This is an observational study among non-crying neonates (n=3073) born in hospitals of Nepal. Non-crying neonates born vaginally at gestational age ≥34 weeks were observed for their response to stimulation with the cord intact or clamped. Obstetric characteristics of the neonates were analysed. Association of spontaneous breathing with cord management was assessed using logistic regression.
Results Among non-crying neonates, 2563 received stimulation. Of these, a higher proportion of the neonates were breathing in the group with cord intact as compared with the group cord clamped (81.1% vs 68.9%, p<0.0001). The use of bag-and-mask ventilation was lower among those who were stimulated with the cord intact than those who were stimulated with cord clamped (18.0% vs 32.4%, p<0.0001). The proportion of neonates with Apgar Score ≤3 at 1 min was lower with the cord intact than with cord clamped (7.6% vs 11.5%, p=0.001). In multivariate analysis, neonates with intact cord had 84% increased odds of spontaneous breathing (adjusted OR, 1.84; 95% CI: 1.48 to 2.29) compared with those with cord clamped.
Conclusions Stimulation of non-crying neonates with intact cord was associated with more spontaneous breathing than among infants who were stimulated with cord clamped. Intact cord stimulation may help establish spontaneous breathing in apnoeic neonates, but residual confounding variables may be contributing to the findings. This study provides evidence for further controlled research to evaluate the effect of initial steps of resuscitation with cord intact.
- resuscitation
- epidemiology
- neonatology
Data availability statement
Data sharing not applicable as no datasets were generated and/or analysed for this study. Data are available upon reasonable request. The dataset generated and analysed is not publicly available as it is part of larger quality improvement projects but can be made available on reasonable request with a data-sharing agreement.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Stimulation is one of the key steps to neonatal resuscitation.
Breathing prior to umbilical cord clamping has been shown to result in smoother cardiovascular transition at birth in experimental studies.figure
What this study adds?
Intact cord stimulation to breathe with the cord intact may help deliver intervention more quickly than stimulation after cord clamping and may also avoid the reflex bradycardia that can occur when the cord is clamped before the lungs are aerated. Further research is needed to define if the results are confounded by factors such as provider experience or the baby’s tone and colour influencing management decisions.
Introduction
Globally, among the 140 million neonates who are born every year, 10–15 million do not cry or breathe at birth.1 These neonates may require resuscitation to transition from the intrauterine to the extrauterine environment.2 Neonates who do not receive timely and adequate resuscitation may die or suffer brain injuries and long-term disability.3 Every year, an estimated 1 million neonates die due to intrapartum-related complications or ‘birth asphyxia’,4 2 million experience hypoxic-ischaemic encephalopathy and 1.2 million go on to show developmental delay.3 Most of these mortalities and morbidities occur in low-income and middle-income countries.
Transitioning to an extrauterine environment depends on two major physiological events, the commencement of breathing and the transition of blood flow from the umbilical to the pulmonary circulation.2 5 The trigger of breathing at birth results in clearance of the liquid in the trachea and airways, aeration of the lungs, reduction in pulmonary vascular resistance and increase in pulmonary blood flow.6 7 This increase in pulmonary blood flow supplies left ventricular preload previously dependent on flow across the patent foramen ovale from the right atrium and the umbilical vein.2 Any intrapartum insult due to placental insufficiency (hypertension, infection or haemorrhage) can delay the spontaneous cardiopulmonary transition and may be compounded by umbilical cord clamping.8 9 As a result, blood flows continuously through the ductus arteriosus, bypassing the pulmonary circulation into the systemic circulation as right-to-left shunting.6 Resuscitation with cord intact may provide a smoother cardiopulmonary transition at birth.
The International Liaison Committee on Resuscitation (ILCOR) provides guidance on neonatal resuscitation.10 The ILCOR 2020 recommends that a neonate who is not crying or breathing with poor tone and heart rate less than 100 beats per minute should receive stimulation and clearing of airways (as needed) with intact cord.10 There is very little robust evidence on the impact of stimulation in neonates receiving resuscitation with the cord intact. The WHO recommends if there is experience in providing ventilation without cutting the umbilical cord, ventilation can be initiated before cord-cutting.11 WHO identifies resuscitation with the cord intact as a key research area to generate a stronger evidence base for care.11
Studies from low-income and middle-income countries have reported that neonates who are not crying or breathing at birth are immediately taken to a neonatal resuscitation area for stimulation, clearing of airways and positive-pressure ventilation.12 13 Despite educational programmes such as Helping Babies Breathe (HBB) from the American Academy of Pediatrics, which advocates stimulation to breathe before clamping the cord, health workers often clamp the cord before initiating resuscitation.14
This study aims to evaluate the impact of stimulation among neonates with the cord intact versus those with cord clamped on breathing and birth outcome.
Methods
Study design
This was a nested observational study within two quality improvement studies SUSTAIN15 and REFINE16 done in nine hospitals of Nepal.
Study sites
This study was conducted among nine hospitals in Nepal. The hospitals are tertiary care hospitals providing referral obstetric services through comprehensive and emergency obstetric and neonatal care services. These hospitals were chosen for quality improvement studies to implement a safer birth bundle. Health workers were trained on HBB 2nd edition to resuscitate neonates with intact cord when possible as part of the safer birth bundle. The cord management was at the discretion of the individual health worker.
Study dates
The study was conducted between 1 June 2019 and 2 May 2020.
Participants
Women in labour with gestational age ≥34 weeks and confirmed fetal heart rate during admission were approached for consent. Women who were admitted for vaginal birth were approached for consent. For this study, neonates who were crying at birth were not eligible for analysis. Non-crying neonates who received additional tactile stimulation constituted the study population. Babies who cried immediately after birth and those with birth defects were excluded from the analysis. Neonates who did not cry and were not stimulated also were excluded from the study.
Sample size
All non-crying neonates who received stimulation were considered for analysis.
Variables
The variables considered were defined as cord status: intact and clamped; parity: no previous birth, one previous birth and two or more previous births; obstetrical complication during admission: includes pre-eclampsia, eclampsia, premature rupture of membranes, preterm labour, polyhydramnios, oligohydramnios, breech/transverse lie, decreased fetal movements, antepartum haemorrhage, chorioamnionitis, cord prolapse, meconium-stained amniotic fluid and maternal medical complications such as diabetes mellitus and pre-existing cardiovascular and renal disease; induction of labour, augmentation labour; mode of delivery: instrumental (for forceps, vacuum application) or spontaneous; preterm birth (age of gestation less than 37 weeks); low birth weight (weight of baby less than 2500 g); immediate thorough drying after birth and breathing after stimulation (spontaneous breathing requiring no positive-pressure ventilation). Stimulation was defined as additional rubbing of the back of non-crying neonates after drying. Stillbirth was defined as no heart rate or breathing at any time after birth.
Data collection and management
The data collection was done through the existing data collection systems of the two studies REFINE and SUSTAIN. Observational data were collected by independent clinical researchers using a tablet-based application (online supplemental file 1). Observation was done on immediate newborn care, status of crying and when drying, clearing of the airway, stimulation and cord clamping were performed. Researchers also extracted information from patient notes on obstetric complications, progress of labour, mode of delivery, sex and weight of neonate. The data were then extracted into SPSS software for cleaning, coding and analysis.
Supplemental material
Data analysis
The non-crying babies included in the study were categorised as those who were stimulated with intact cord and those who were stimulated after cord clamping. Spontaneous breathing after stimulation was observed. Obstetrical and neonatal characteristics were compared between the two groups.
Multivariable analysis using logistic regression was done to assess the association of cord status during stimulation on breathing by adjusting for the variables which had a significance level difference of p<0.01. The variables which were significantly different by cord status during stimulation were complications during admission, mode of delivery and immediate drying.
Patients and public involvement
The main study aimed to improve the provision and experience of care of patients (mother and newborn) during childbirth. Information was provided to patients on their involvement in the main study. Results from this study will be disseminated to healthcare providers, paediatric associations and global neonatal guideline development organisations.
Results
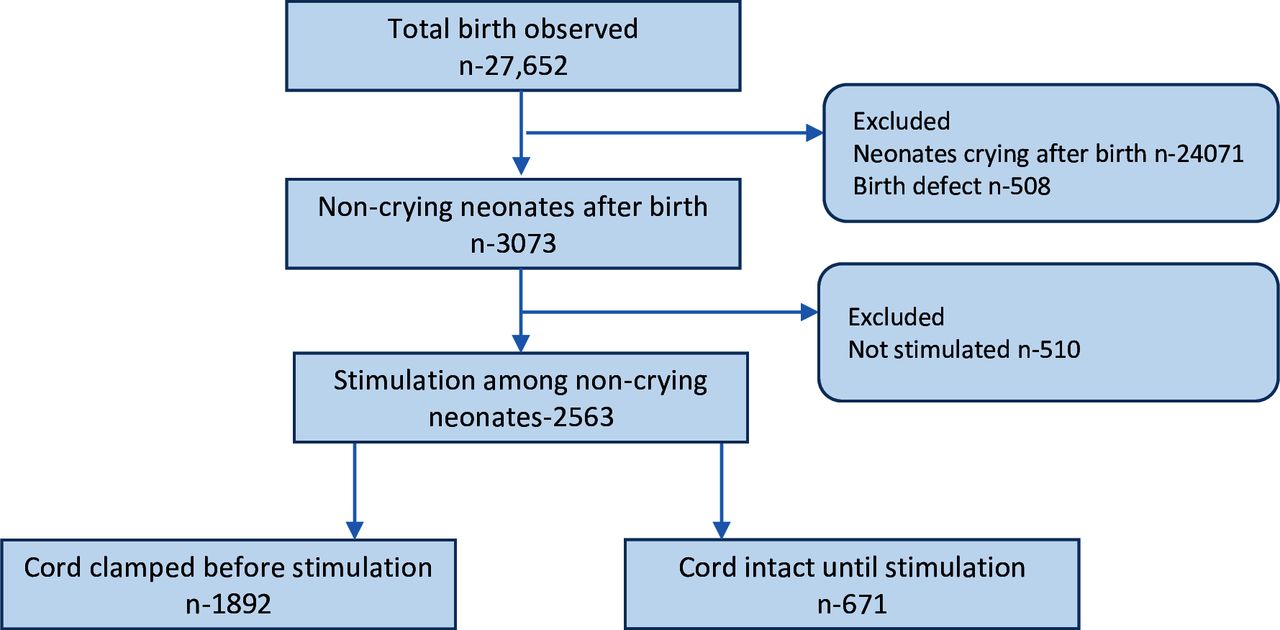
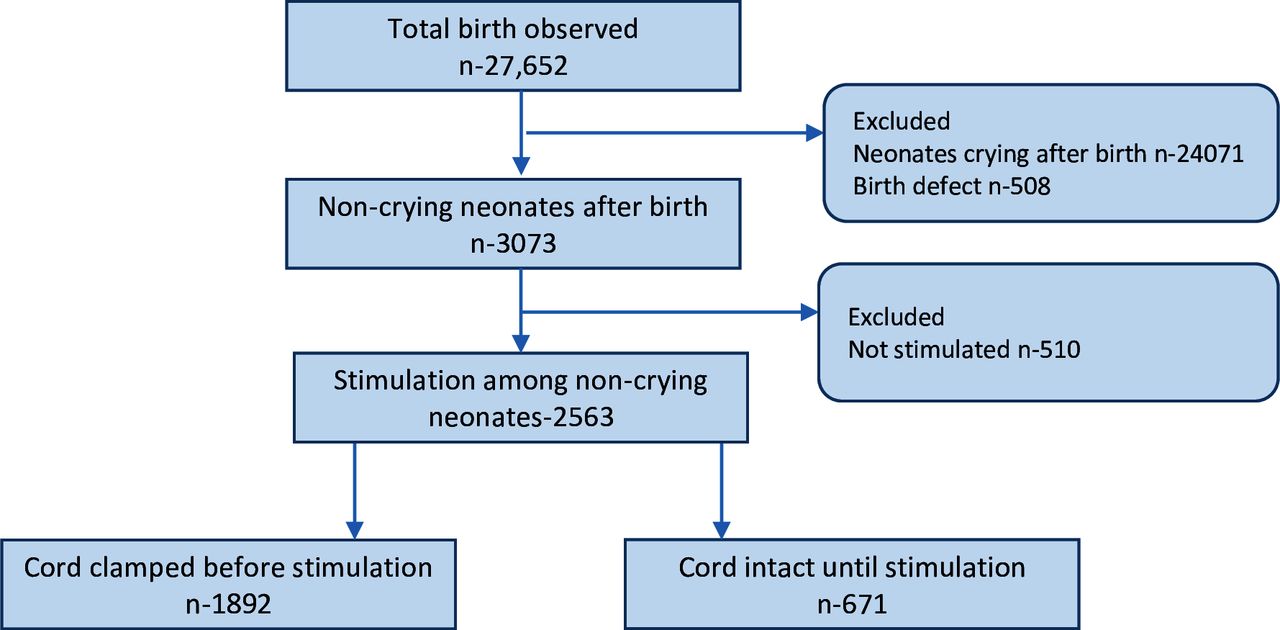
During the study period, 41 621 women delivered in the hospitals and 34 652 women consented to the study. Among the consented women, 27 652 births were observed in the study. Among the total births observed, 24 071 babies were excluded as they cried immediately after birth and 508 births were further excluded due to birth defects; 3073 non-crying neonates were included in the analysis. Among the non-crying neonates, 2563 were stimulated. Of the neonates stimulated, 671 (26.2%) of them had their cord intact, while 1892 (73.8%) had their cord clamped (figure 1).
{kind=link}
Study flow figure.
We compared the obstetric and neonatal characteristics of neonates who had cord intact versus cord clamped before stimulation. Obstetric complications during admission were lower among neonates who had cord intact than those who had the cord clamped (8.0% vs 11.2%, p=0.022).
Neonates who had cord intact had lower proportion of breech or transverse lie during labour than those who had the cord clamped (1.3% vs 3.5%, p=0.003). Among neonates with cord intact, a lower proportion had meconium-stained amniotic fluid during labour as compared with those with the cord clamped (22.2% vs 28.4%, p=0.002). Induction of labour was lower among neonates with cord intact than clamped (18.5% vs 25.5%, p<0.0001). The proportion of neonates born through instrumental delivery was lower among those with cord intact clamped (8.4% vs 12.3%, p=0.005) (table 1).
Obstetric and neonatal characteristics among non-crying neonates with intact cord versus cord clamped during stimulation
The clinical outcome differed among neonates stimulated with the cord intact versus with those cord clamped. Among neonates stimulated with the cord intact, 81.1% breathed, while 68.9% breathed after stimulation with cord clamped (p value<0.0001). The use of bag-and-mask ventilation was lower among those who were stimulated with the cord intact than those who were stimulated with cord clamped (18.0% vs 32.4%, p<0.0001). The proportion of neonates with Apgar Score 3 or less at 1 min was lower with the cord intact than clamped (7.6% vs 11.5% p=0.001). The proportion of neonates with Apgar Score 6 or less at 5 min was lower with the cord intact than clamped (7.9% vs 12. 7%, p<0.0001). The proportion of mortality was not significantly different between those with cord intact and clamped (0.7 vs 1.6%, p=0.123) (table 2).
Clinical outcome of non-crying neonates who were stimulated with cord intact versus cord clamped
We compared the obstetric and neonatal characteristics of non-crying neonates who breathed after stimulation. Overall, 58.3% of neonates with a maternal complication during admission breathed after stimulation, while 73.8% of neonates without maternal complication breathed after stimulation (p value<0.0001). Overall, 66.3% of neonates born through instrumental delivery breathed after stimulation, while 72.9% of neonates who were born through spontaneous delivery breathed after stimulation (p value=0.021). Among neonates who were not immediately dried after birth, 62.8% breathed after stimulation, while 72.7% of neonates who were immediately dried after birth breathed after additional stimulation (p value=0.01) (table 3).
The obstetric and neonatal characteristics of non-crying neonates who responded to stimulation
In bivariate analysis, there were 1.94 higher odds of breathing if the cord was intact during stimulation compared with neonates with cord clamped (crude odds ratio (cOR), 1.94; 95% CI: 1.56 to 2.40). If the neonate’s mother had complications during admission for delivery, the odds of breathing after stimulation were 0.50 lower than neonate’s whose mother had no complication during admission (cOR, 0.50; 95% CI: 0.38 to 0.64). Neonates who were dried immediately after birth had 1.57 higher odds of breathing after stimulation than those who were not dried after birth (cOR, 1.57; 95% CI: 1.12 to 2.19). In neonates with birth weight <2500 g, the odds of breathing after stimulation was 0.63 lower than neonate’s with low birth weight (cOR, 0.63; 95% CI: 0.51 to 0.78) (table 4).
Bivariate and multivariate analysis of association between obstetrics and neonatal characteristics with breathing after stimulation
In multivariate analysis, to assess the association of characteristics with breathing after stimulation, there was 1.84 higher odds of breathing if the cord was intact during stimulation when compared with neonates with cord clamped (adjusted OR (aOR), 1.85; 95% CI: 1.48 to 2.30) after adjusting for obstetrical complications during admission, mode of delivery, immediate drying after birth, low birth weight and preterm birth. Neonates who were dried immediately after birth had 1.49 higher odds of breathing after stimulation than those who were not dried after birth (aOR, 1.47; 95% CI: 1.04 to 2.07) (table 4).
Discussion
In this observational study, one-fourth of the non-crying neonates had stimulation performed with an intact cord. There were higher odds of spontaneous breathing if the cord was kept intact during stimulation than neonates who had their cord clamped during stimulation. The higher obstetrical complications during admission and Apgar Score less than 4 at 1 min among early cord clamped non-crying neonates indicates that these are more depressed neonates than neonates with cord intact. In line with this, a higher proportion of infants with early cord clamping received bag-and-mask ventilation. Even though there was no significant difference in mortality between the two groups, the mortality trended lower among the neonates who were stimulated with the cord intact.
An experimental animal study by Bhatt et al demonstrated a more stable cardiovascular adaptation if cord clamping was performed after initiation of ventilation.7 The results from this and other studies suggested that resuscitation of newborns should be performed with an uncut cord, facilitating the postnatal transition.17–19 However, in a single-centre observation study in Tanzania, there was no significant association between time to cord clamping and onset of breathing or initiation of positive-pressure ventilation following stimulation/suction.20
Similar to our results, a single-centre randomised controlled trial (RCT) in California, USA, to evaluate the effect of delayed cord clamping in premature infants (<32 weeks) who required ventilation demonstrated that provision of gentle tactile stimulation with the cord intact may hasten the establishment of spontaneous respirations and provide a similar placental transfusion compared with positive-pressure ventilation with delayed cord clamping.21 Another multicentric trial in the UK among premature infants (≤32 weeks) suggests that cord clamping after at least 2 min and providing neonatal care with the cord intact may improve outcome at discharge as compared with early clamping.22
A single-centre RCT in Nepal evaluated the effect on delayed versus early cord clamping in babies requiring resuscitation.23 In the trial, randomisation was performed while the baby was still in utero and resuscitation measures (stimulation and positive-pressure ventilation) performed according to the HBB algorithm with an unclamped cord in the mother’s bed were associated with early spontaneous breathing.
Our multicentric study conducted between 2017 and 2018 showed that 9.8% of neonates do not cry at birth.12 The study found that non-crying but breathing babies might not have the full respiratory capacity and require resuscitation.24 In this study, we hypothesise that the non-crying neonates who breathe spontaneously after stimulation might have been in primary apnea. There is increased oxygenation with intact cord due to several interacting mechanisms: persisting oxygenation by the placenta, avoidance of bradycardia often associated with clamping the cord before the onset of respirations and earlier initiation of breathing resulting in increased pulmonary blood flow.
A study in Tanzania showed that although the healthcare provider commonly practiced clamping the umbilical cord immediately after delivery, they were aware that delayed cord clamping has a potential benefit of oxygenation to the newborn in the event of the need for resuscitation.25 Our study also shows that despite the education of healthcare providers on keeping the cord intact during resuscitation, two-thirds of the non-crying babies received resuscitation after cord clamping. There is a need to implement a delay in clamping as a quality improvement intervention to improve initial steps of resuscitation—especially stimulation and if necessary bag-and-mask ventilation. Three recent systematic reviews and meta-analysis showed that there is a lack of evidence to recommend cord management among term and preterm infants who receive positive-pressure ventilation at birth.26 27
Methodological consideration
This study has several strengths including that observations were done by trained researchers in multiple hospitals in Nepal in a consistent way and with large sample size. Using observational methods limited recall bias. However, there are several limitations. First, this observation was only done for vaginal births and not for caesarean births. Second, cord management was at the discretion of the health workers, so there may have been a bias toward the previous practice of immediate cord clamping. The appearance of the baby at birth (degree of cyanosis, hypotonia) may have influenced decision-making on when to cut the cord.
In conclusion, our study found that non-crying neonates stimulated with the cord intact were more likely to breathe than those who were stimulated with the cord clamped. Stimulation with cord intact may help establish spontaneous breathing in apnoeic neonates, but residual confounding variables are likely contributing to the findings. Our study provides additional evidence consistent with the ILCOR recommendation on keeping the cord intact during the initial steps of resuscitation. This study highlights the importance of further controlled research to evaluate the effect of initial steps of resuscitation with cord intact.
Data availability statement
Data sharing not applicable as no datasets were generated and/or analysed for this study. Data are available upon reasonable request. The dataset generated and analysed is not publicly available as it is part of larger quality improvement projects but can be made available on reasonable request with a data-sharing agreement.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approval was granted by the Ethical Review Board of the Nepal Health Research Council for SUSTAIN (ref. 110/2019) and REFINE studies (ref. 87/2018). Written informed consent was obtained from the participants at the time of admission to the hospital before enrolling in the study.
Acknowledgments
The authors would like to thank all the data coordinators and surveillance officers, hospital manager, all the nurses and support staff working in the sick newborn care units. The authors thank all the mothers and caregivers of the sick newborns who consented to the study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @ShyamSuBu
Collaborators Nepal Neonatal Network: Omkar Basnet, Srijana Sharma, Pratikshya Bhattarai, Ankit Acharya, Professor Anjani Kumar Jha, Dr Yasho Vardhan Pradhan, Dr Sushil Nath Pyakurel, Professor Kiran Bajracharya, Dr Sheela Verma, Dr Amit Bhandari, Dr Anjana KC Thapa, Dr Krishna Prasad Bista, Jhalak Sharma Paudel, Sangita Khatri and Leela Paudel.
Contributors AKC and NS conceptualised the study. AKC, JT and SSB conducted the analysis. NS and RG provided feedback to the analysis. AKC, SSB, RG and JT wrote the first draft. NS and SN made the second and final revision to the draft. All authors reviewed and provided feedback on the revised version and agreed to the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.