Article Text

Abstract
Objective To determine the prevalence of reported ‘household stressor’ adverse childhood experiences (ACEs) in families of children presenting with neurodevelopmental, behavioural or emotional difficulties and to determine whether family vulnerabilities, individually or cumulatively, were associated with particular clinical symptomatology.
Design Retrospective chart review followed by statistical analysis of family stressors and clinical symptomatology.
Setting A community paediatric clinic in Australia.
Participants All 267 children who attended an initial paediatric appointment during 2018.
Results 162 (60.7%) children had been exposed to one or more household stressor ACEs, including 116 (43.4%) children exposed to parental mental illness. Behavioural disturbance occurred in 144 (53.9%) children and externalising behaviours (other than attention deficit hyperactivity disorder) were more frequent than internalising behaviours. Externalising and internalising behaviours were associated with individual and cumulative household stressor ACEs. Most other symptomatology apart from genetic/neurological conditions, autistic symptoms and some developmental delays appeared to be partially associated with ACEs.
Conclusion Household stressor ACEs were common, frequently occurred concurrently, and were associated with much of the symptomatology, in this cohort. Parental mental illness was the most prevalent stressor and behavioural disturbance the most prevalent symptomatology. These findings may have implications for clinical practice and service provision.
- child psychiatry
- health services research
- psychology
- social work
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
What is known about the subject?
Mental health disorders affect around one in seven children annually in Australia.
One in five children in Australia experience three or more combined adverse childhood experiences (ACEs).
ACEs, including child abuse and neglect, are associated with impaired developmental, behavioural and emotional outcomes in children and adolescents.
What this study adds?
Household stressor ACEs, in the absence of abuse or neglect, were common in children presenting to an Australian community paediatric clinic.
Household stressor ACEs were individually and cumulatively associated with specific symptomatology in children attending an Australian community paediatric clinic.
The most prevalent stressor was parental mental illness and the most prevalent symptomatology was behavioural disturbance.
Introduction
Adverse childhood experiences are common worldwide and are risk factors for most mental disorders including mood, anxiety, behaviour, substance use and personality disorders, as well as psychotic experiences and suicidal behaviour.1 Half of adult mental health problems originate in childhood and mental health disorders affect around one in seven children annually,2 now comprising the majority of general paediatric practice in Australia.3 The significance of ACEs became apparent in 1998 when Felitti et al published ground-breaking research demonstrating a frequency-dependent relationship between the number of adversities experienced in childhood, impaired physical and mental well-being in adulthood and reduced life expectancy.4 The relevance of ACEs to adult and child mental health is well-substantiated and there has been much recent debate about the need to address underlying contributing factors to childhood mental illness, especially parental mental illness and early attachment difficulties1 3 5–8 and to improve adverse parenting practices.9
ACEs were traditionally described in 3 main categories, with 10 subcategories: child abuse (physical, sexual and emotional), child neglect (physical and emotional) and ‘household dysfunction’ (domestic violence, parental mental illness, parental substance abuse, parental separation and parental incarceration).10 Subsequent research has described other ACEs such as community violence and many ACE screening tools have been developed11 but are used only in specific circumstances in Australia.12–14 Whereas research into ACEs and adult mental health has necessarily been largely retrospective, there is increasing interest in behavioural and emotional problems in children whose ACEs may be ongoing. Much research on ACEs in childhood has looked at the combined effects of abuse, neglect and household stressors1 10 11 15; instead, this paper focuses on possible associations between mental health symptomatology in childhood and household stressor ACEs in the absence of apparent abuse and neglect.
Among Australian children, one in five experience three or more combined ACEs16 and 64% children attending a community paediatric clinic in South Western Sydney had one or more combined ACEs17 but the community prevalence of household stressor ACEs in the absence of abuse and neglect is unknown, as is the degree to which these stressors themselves may contribute to child morbidity. Another Australian community paediatric clinic study had found a considerable incidence of reported domestic violence, parental mental health problems and parental substance abuse despite difficulties asking about these factors during paediatric consultation.12 This study seeks to determine the prevalence of disclosed household stressor ACEs in a cohort of community paediatric clinic patients and to explore whether some symptomatology in developmental, behavioural and emotional paediatrics might be related to household stressors.
Methods
The study was a retrospective chart review of all children who attended an initial paediatric appointment in an Australian community paediatric clinic during 2018 (n=267). All children were referred by general practitioners (GPs) for suspected developmental delays or disabilities, behavioural or emotional concerns. In this particular jurisdiction children with suspected abuse or neglect are referred elsewhere, to a specialised child protection unit, and not to the regular community paediatric clinic.
Charts were reviewed and information was obtained from the following sources: GP referral letter; paediatrician’s notes; paediatrician’s letter to GP following initial appointment with their working differential diagnoses. Child characteristics were noted. Family stressors (the original 5 ‘household dysfunction’ ACEs) were recorded if documented as disclosed (absent data were treated as negative). These were parental separation (child not living continuously with both biological parents), mother treated violently, parental substance abuse, parental mental illness and parental incarceration. Clinical symptomatology was grouped into descriptive categories. As symptoms were not mutually exclusive, two or more categories were usually relevant. To minimise bias, data regarding GPs’ presenting concerns, paediatricians’ differential diagnoses and family factors were reviewed and recorded separately. Clinical categories used were attention deficit hyperactivity disorder (ADHD) (inattention, hyperactivity, impulsivity), Externalising-other (externalising behaviours other than ADHD, such as oppositionality, defiance, aggression and violence), Internalising (internalising behaviours suggestive of anxiety or depression), ASD (autism spectrum disorder) (impairments in social communication and restricted repetitive interests or behaviours), Sensory (sensory processing difficulties), Speech/Language (speech or language delay), Developmental Delay-other (developmental delays other than Speech/Language), Learning difficulties (learning difficulties including specific learning disorders and intellectual disability), Genetic/Neurological (genetic or neurological conditions), Traumatised (developmental trauma) and Other.
Statistical analyses were performed in RStudio with R V.3.5.3. Associations between differential diagnoses and individual family factors, as well as associations between the family factors themselves, were measured as ORs using the epitools package (V.0.5–V.10). OR p values were estimated using median-unbiased method (mid-p) and adjusted for multiple comparisons using the Benjamini-Hochberg procedure. Both positive (OR >1.0) and negative (OR <1.0) associations were noted. The differences in differential diagnosis frequency between sexes were assessed using a two-proportions Z-test with Bonferroni adjustment for multiple comparisons. The differences in age distribution between diagnoses were represented in quartile plots and tested using a non-parametric Kruskal-Wallis rank test followed by Dunn’s multiple comparisons (dunn.test package, V.1.3.5). The difference in the number of ACEs (cumulative burden) between diagnoses was also assessed using this method. The association between age, sex and number of ACEs was assessed using Poisson regression. All tests were two-tailed and the significance level was set at α=0.05 for all tests. The 95% CIs are reported in brackets next to point estimates where appropriate.
Patient and public involvement
Neither patients nor the public contributed to study design, process or aims.
Results
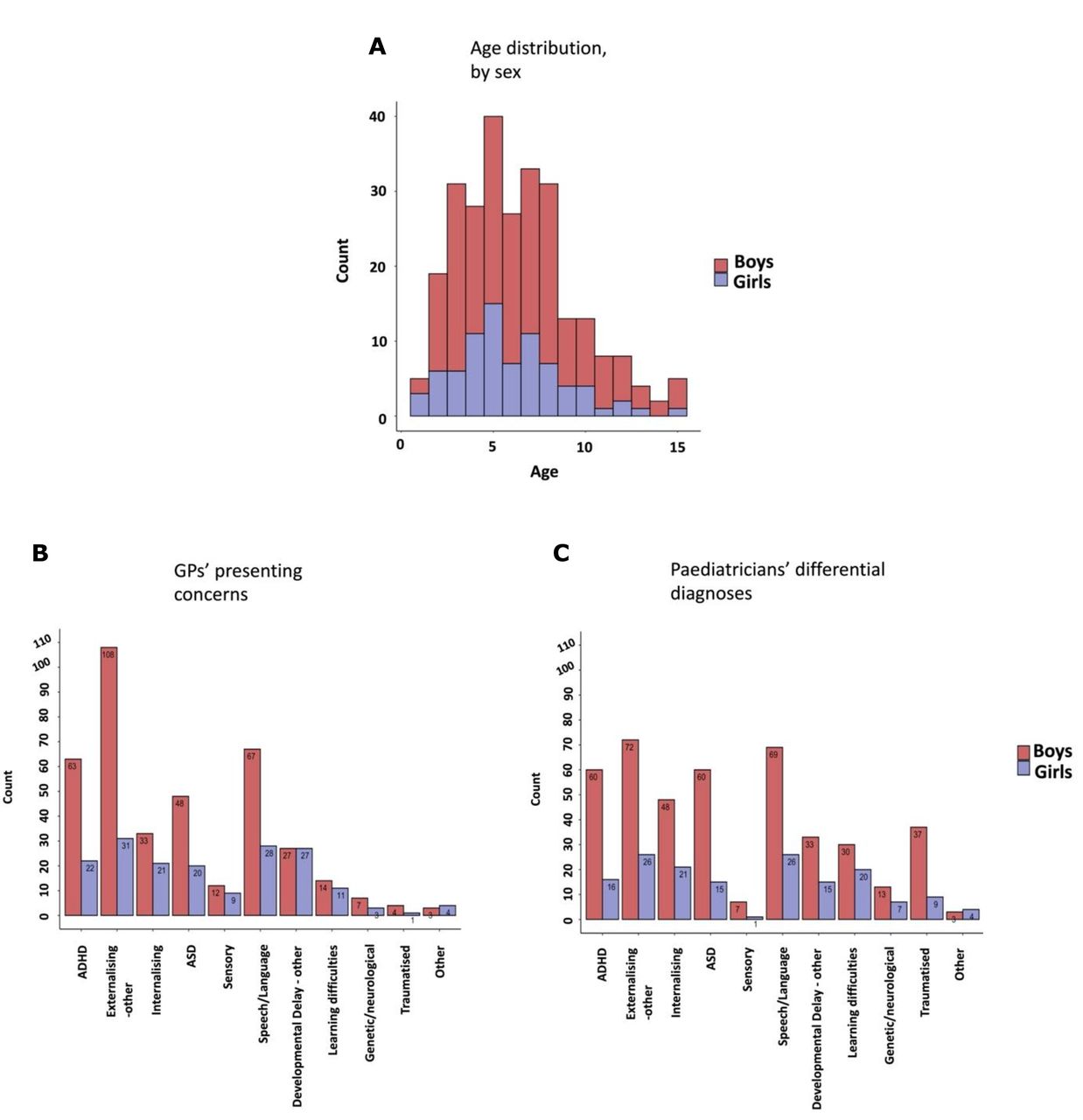
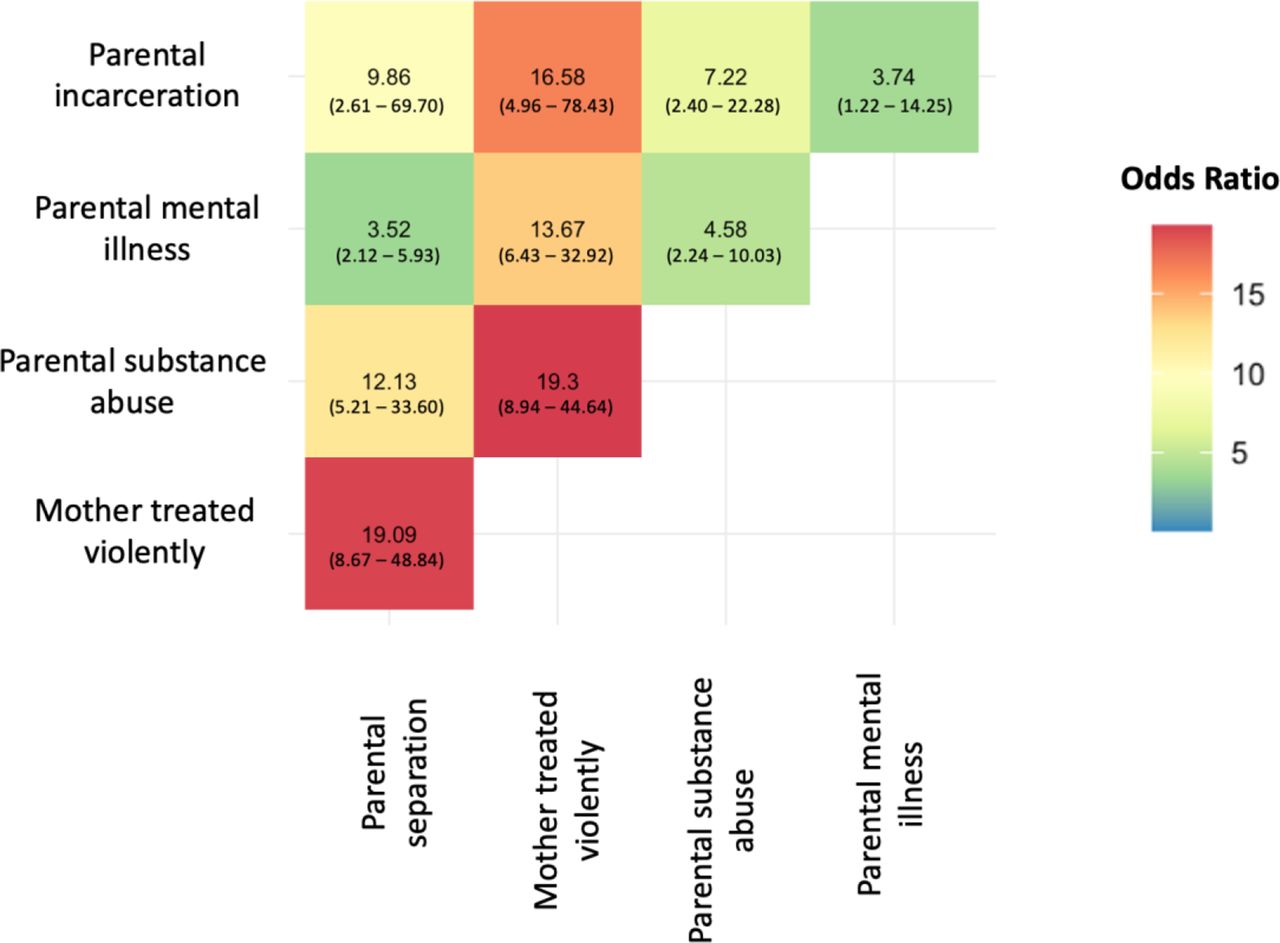
The children were largely physically healthy without obvious biological factors which might predispose to neurodevelopmental difficulties: only 10.5% were preterm and only 6.0% had recurrent hospital admissions. Seventy per cent were boys. Age and sex distribution are shown in figure 1A. One hundred and sixty-two children (60.7%) were reportedly exposed to one or more household stressor ACEs: parental mental illness (43.4%, n=116), parental separation (40.1%, n=109), mother treated violently (22.1%; n=59), parental substance abuse (15.7%, n=42), parental incarceration (5.6%, n=15). There were strong associations between all five household stressor ACEs as shown in figure 2 and online supplemental table S1.
Supplemental material
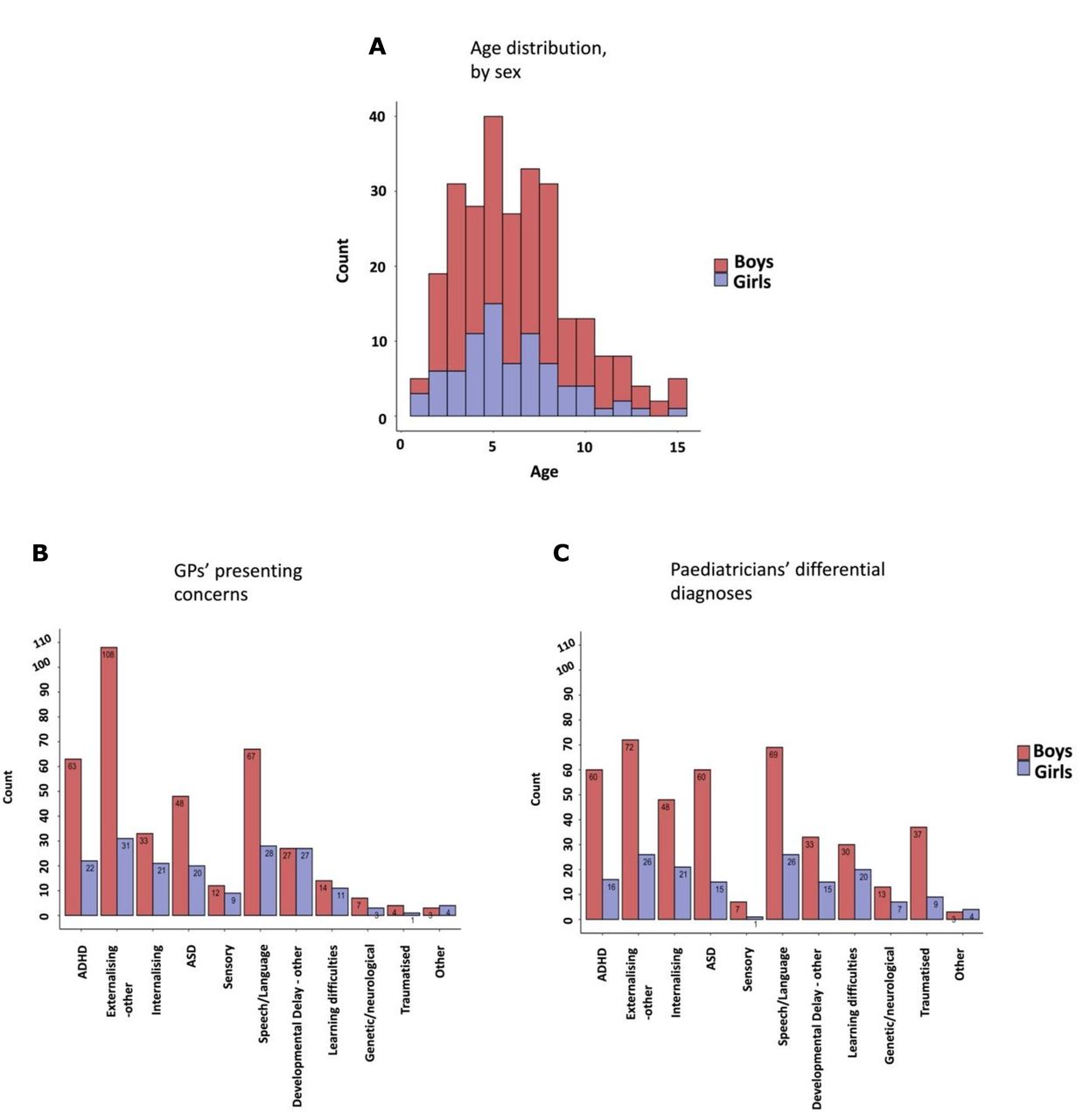
Sample demographics: age, sex and symptomatology frequency. Histogram showing age distribution of the sample by sex (A). Histogram showing number of children and their GPs’ presenting concerns (B). Histogram showing number of children and their paediatricians’ differential diagnoses (C). Children may have more than one presenting concern or differential diagnosis. ADHD (attention deficit hyperactivity disorder), Externalising-other (externalising disorders other than ADHD), Internalising (internalising behaviours suggestive of anxiety or depression), ASD (autism spectrum disorder), Sensory (sensory processing difficulties), Speech/Language (speech or language delay), Developmental Delay-other (developmental delays other than Speech/Language), Learning difficulties (learning difficulties including specific learning disorders and intellectual disability), Genetic/Neurological (genetic or neurological conditions), Traumatised (developmental trauma). GP, general practitioner.

Association between family factors, as measured by OR. Numbers represent OR and their 95% CI. The OR is calculated as (odds of adverse childhood experience (ACE)-1 co-occurring with ACE-2)/(odds of ACE-1 occurring without ACE-2), with ACE-1 and ACE-2 two different ACEs displayed in rows and columns, respectively. An OR greater than 1 (positive association) implies that the odds of ACE-1 and ACE-2 co-occurring are higher than the odds of ACE-1 not co-occurring with ACE-2. Statistically, all five household stressor ACEs were positively associated with each other (ie, they were more likely to co-occur than not). The raw count data can be found in online supplemental table S1.
Frequencies of GPs’ presenting concerns are shown in figure 1B and paediatricians’ differential diagnoses in figure 1C. In both GPs’ presenting concerns and paediatricians’ differential diagnoses, total externalising behaviours (Externalising-other and ADHD combined) were the predominant symptoms, followed by developmental concerns about Speech/Language and ASD. Internalising behaviours were less prevalent. The frequencies of GPs’ presenting concerns and paediatricians’ differential diagnoses were similar except for differences in Externalising-other and Traumatised, which might be explained by paediatricians ascribing externalising behaviours to disclosed trauma. GPs’ presenting concerns were not considered further.
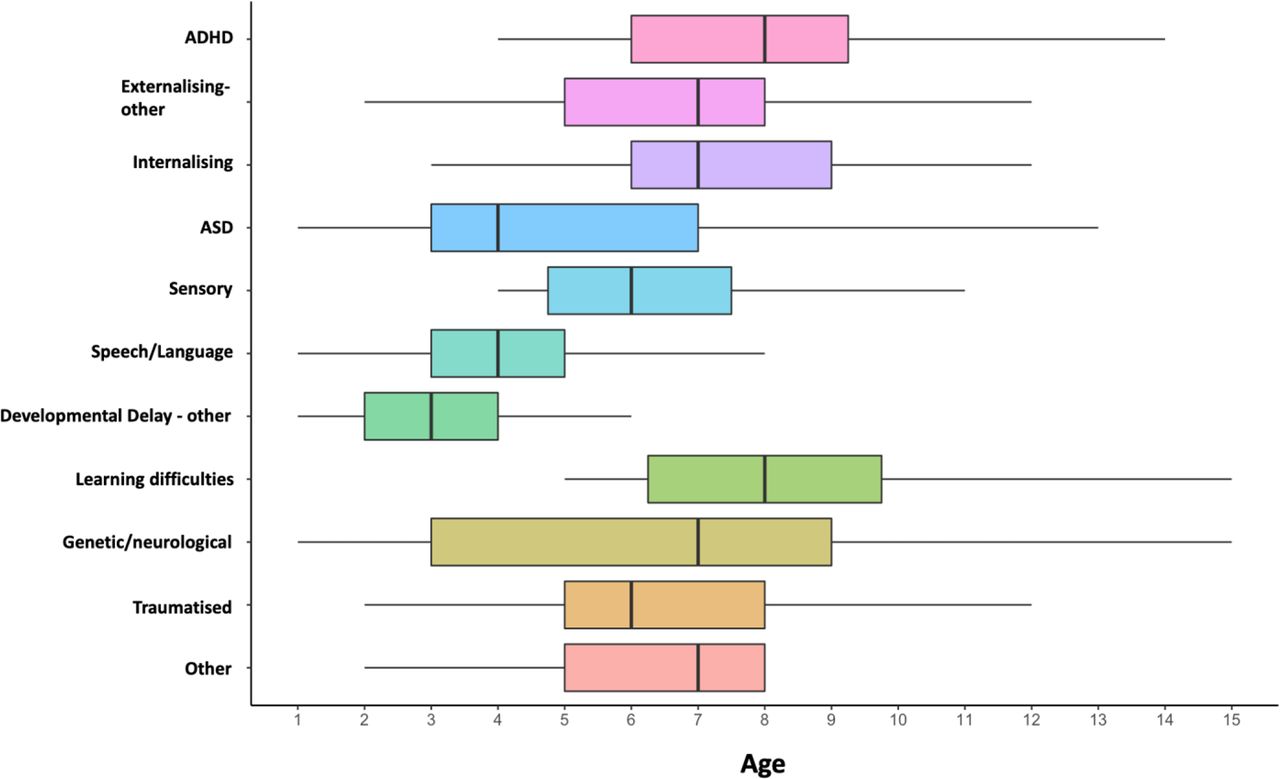
There were statistically significant differences in age distribution between differential diagnoses (χ2=118.71, df=10, p<0.001; figure 3 and online supplemental table S2). The most common differential diagnoses in young children were Developmental Delay-other, Speech/Language and ASD. Symptomatology was more varied in older children. Differences in symptomatology frequency between sexes were apparent (online supplemental table S3) although none met statistical significance. Notably, girls had a higher prevalence of learning difficulties than boys.
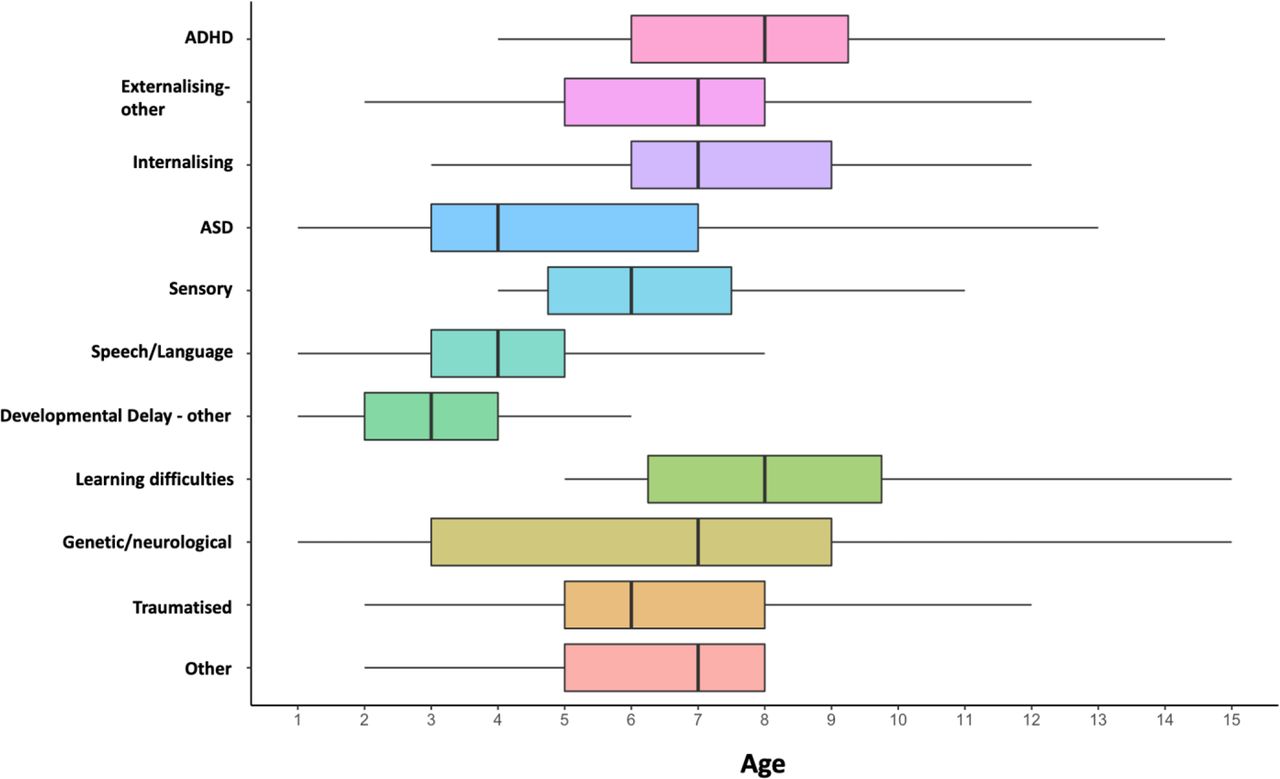
Boxplots showing age distribution across different differential diagnoses. There were statistically significant differences in age between differential diagnoses. For example, children with ADHD and internalising disorders were older than children with ASD. Refer to online supplemental table S2 for detailed results of Kruskal-Wallis and Dunn’s multiple comparisons statistical tests. Children may have more than one differential diagnosis. ADHD (attention deficit hyperactivity disorder), Externalising-other (externalising disorders other than ADHD), Internalising (internalising behaviours suggestive of anxiety or depression), ASD (autism spectrum disorder), Sensory (sensory processing difficulties), Speech/Language (speech or language delay), Developmental Delay-other (developmental delays other than Speech/Language), Learning difficulties (learning difficulties including specific learning disorders and intellectual disability), Genetic/Neurological (genetic or neurological conditions), Traumatised (developmental trauma).
Globally, Externalising-other, Internalising and Traumatised were independently associated with individual household stressor ACEs. Although associations less often reached significance in girls as compared with boys, the directionality of associations was the same. Significant associations between differential diagnoses and disclosed individual household stressors are shown as ORs in table 1 and non-significant associations are included in online supplemental tables S4–S6. Externalising-other occurred in 53% (44%–62%) of children with disclosed parental separation but only 25% (19%–33%) without, 58% (45%–70%) of children with disclosed violence to mother but only 31% (25%–37%) without, 60% (44%–74%) of children with disclosed parental substance abuse but only 32% (27%–39%) without, and 47% (37%–56%) children with disclosed parental mental illness but only 29% (22%–37%) without. Traumatised occurred in 39% (30%–48%) of children with disclosed parental separation but only 3% (1%–6%) without, 59% (46%–72%) children with disclosed violence to mother but only 5% (3%–9%) without, 60% (44%–74%) children with disclosed parental substance abuse but only 9% (6%–14%) without, 31% (23%–40%) of children with disclosed parental mental illness but only 7% (3%–12%) without and 60% (33%–81%) children with disclosed parental incarceration but only 15% (11%–20%) without. Internalising occurred in 38% (29%–47%) children with disclosed parental mental illness but only 17% (11%–23%) children without. There were no significant positive associations between: Externalising-other and parental incarceration; Internalising and parental separation, mother treated violently, parental substance abuse, parental incarceration; or between ASD, Sensory, Speech/Language, DD-other, Learning Difficulties, Genetic/Neurological and any of the five household stressor ACEs. Conversely, ASD occurred in only 17% (10%–25%) of children with disclosed parental separation but in 36% (29%–34%) without. Developmental Delay-other occurred in only 11% (6%–18%) of children with disclosed parental separation and in 10% (6%–17%) children with disclosed parental mental illness but in 23% (17%–30%) without disclosed parental separation and in 24% (17%–31%) children without disclosed parental mental illness. Genetic/Neurological occurred in only 2% (0%–6%) of children with disclosed parental mental illness but in 12% (7%–18%) without. There were no significant negative associations between ADHD, Externalising-other, Internalising, Sensory, Speech/Language, Learning Difficulties, Traumatisation and any of the five household stressor ACEs.
Relationship between differential diagnoses and ACEs, expressed as OR
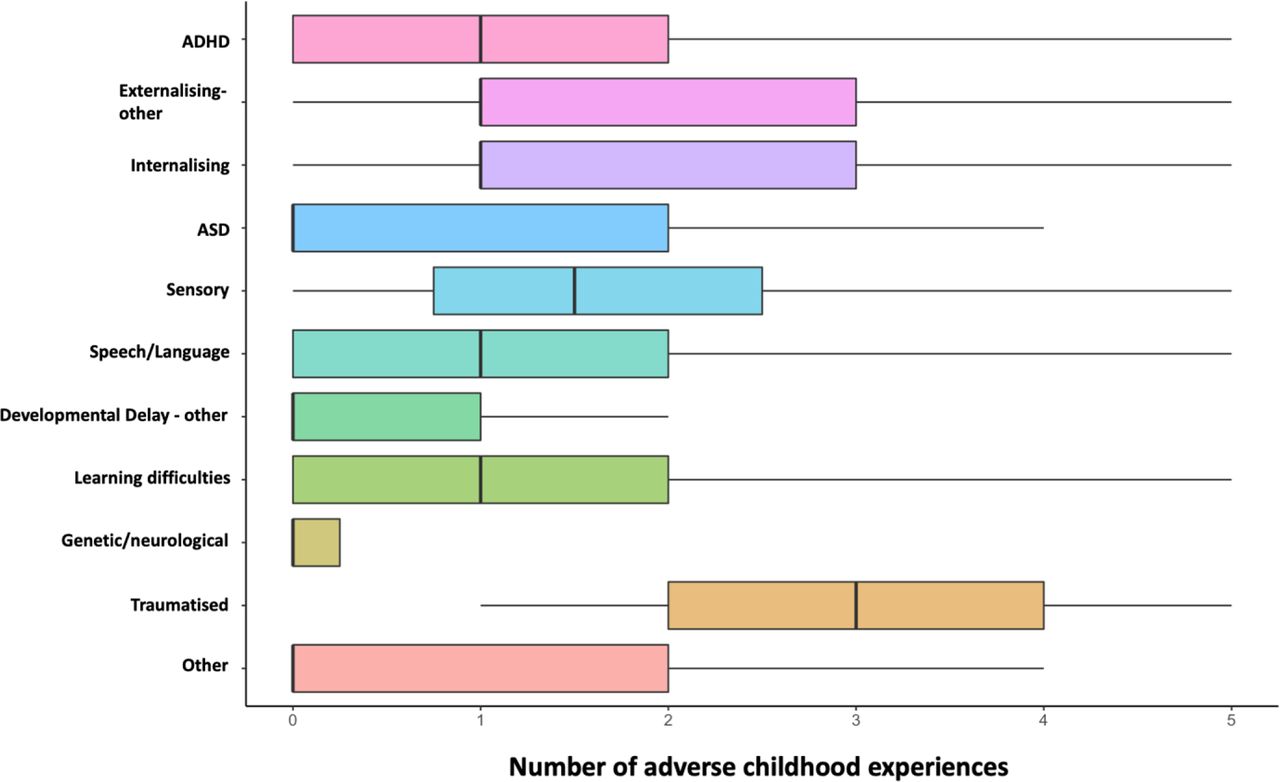
There were statistically significant differences in number of ACEs between differential diagnoses (χ2=106.78, df=10, p<0.001). Externalising-other, Traumatised and Internalising were associated with a higher cumulative burden of ACEs compared with ASD, Developmental Delay-other and Genetic/Neurological (figure 4 and online supplemental table S7). Figure 4 suggests that all differential diagnoses, except ASD, Developmental Delay-other and Genetic/Neurological, were partially related to ACEs. The median number of cumulative ACEs was zero in ASD, Developmental Delay-other, Genetic/Neurological; one in ADHD, Externalising-other, Internalising, Speech/Language, Learning Difficulties; one and a half in Sensory; three in Traumatised. There were no significant associations between age, sex and the number of ACEs.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Boxplots showing cumulative number of adverse childhood experiences (ACEs) across different differential diagnoses. There were statistically significant differences in the cumulative number of ACEs between differential diagnoses. For example, there were more ACEs in children with externalising and internalising disorders than in children with ASD. Refer to online supplemental table S7 for detailed results of the Kruskal-Wallis and Dunn’s multiple comparisons tests. Children may have more than one differential diagnosis. ADHD (attention deficit hyperactivity disorder), Externalising-other (externalising disorders other than ADHD), Internalising (internalising behaviours suggestive of anxiety or depression), ASD (autism spectrum disorder), Sensory (sensory processing difficulties), Speech/Language (speech or language delay), Developmental Delay-other (developmental delays other than Speech/Language), Learning difficulties (learning difficulties including specific learning disorders and intellectual disability), Genetic/Neurological (genetic or neurological conditions), Traumatised (developmental trauma).
Discussion
Our study demonstrated that household stressors, in the absence of abuse or neglect, occurred in 60% of children presenting to this paediatric clinic with developmental, behavioural or emotional symptoms. Both positive and negative relationships between household stressors and differential diagnoses were found (table 1) and stressors frequently coexisted (figure 2). We demonstrated that the more adversities the child was exposed to, the more likely they were to have externalising and internalising behaviours and even traumatisation (figure 4). The most common stressor was parental mental illness and the most common symptomatology was behavioural disturbance. The results suggest that common child mental health symptomatology in this cohort appeared to be related to household stressors. We suggest that these findings may have important implications for clinical practice.
Household stressor ACEs were common in this cohort, reflecting the combined ACE prevalence in the overall Australian child population16 and the combined ACE prevalence in a Sydney community paediatric clinic.17 In the absence of screening, the paediatrician’s discretion determined whether or not enquiry about household stressors occurred; household stressors were possibly under-reported rather than over-reported as many parents might not disclose certain personal details on their first encounter with a new clinician.12 The high concurrence with all household stressor ACEs accords with much previous evidence of clustering of adversities.1 5 6
Our findings of the most common differential diagnoses were similar to the categories described as the major and overlapping childhood mental health diagnoses of Disruptive Behaviour Disorders (our Externalising-other and Traumatised), Anxiety Disorders, ADHD and ASD.2 Our cohort differed by including many young children with speech/language problems. Notably, Externalising-other and Traumatised combined was the most prevalent clinical symptomatology in the cohort and boys predominated. This correlates with evidence from the Longitudinal Study of Australian Children (LSAC) showing that more boys attend services for mental health problems, as boys have more externalising problems which are more noticeable than internalising problems.18 Also, our cohort largely excluded adolescent girls with mood disorders, suggestive of emotional trauma,19 who may attend other services.
Statistical analysis showed positive associations between individual household stressors and specific symptomology. Overall parental mental illness was associated with the widest range of symptomatology, including internalising behaviours as well as externalising behaviours and traumatisation. Parental separation, violence towards mother and substance abuse were all associated with externalising behaviours and traumatisation but not with internalising behaviours. Having an incarcerated parent was associated with traumatisation. It is possible that the magnitude of any statistical associations might have been inflated or reduced by the paediatricians’ bias to ask about ACEs when suspected. However, our findings correspond with much evidence in the literature of associations of symptomatology with specific family factors: mental health and language problems at 10 years with recent exposure to intimate partner violence20; conduct problems with interpersonal violence21; adolescent anxiety disorders with separated parents and parental mental illness22; child and adolescent mental disorders with step-parent, blended-parent or one-parent families23; behaviour problems at 3 years with severe parental personality disorders.5 Statistical analysis also showed negative associations between household stressors and specific symptomatology. With parental mental illness there was reduced frequency of Developmental Delay-other and Genetic/Neurological and similarly with parental separation, reduced frequency of ASD and Developmental Delay-other. This might suggest that parental mental illness and parental separation limit parental ability in some cases to seek services for developmentally compromised young children (Developmental Delay-other and ASD tended to present in younger children, although the age range of presentation for Genetic/Neurological was wider), similarly to the difficulties that some disadvantaged families in LSAC may have in seeking services for children with certain conditions.18 It is also possible that clinician enquiry about ACEs was less frequent when children presented with these specific difficulties.
The cumulative burden of household stressors ACEs was higher in Externalising-other, Internalising and Traumatised than in ASD, Developmental Delay-other and Genetic/Neurological correlating with previous evidence of the cumulative impact of stressful child environments on externalising and internalising behaviours.1 22 24 25 Our findings—suggesting that all differential diagnoses other than ASD, Developmental Delay-other and Genetic/Neurological may be partially related to ACEs—align with evidence from larger studies showing that ADHD, language, academic competence and cognition may all be associated with family factors.1 10 11 24 26–29
The basic determinants of child health and development are now well understood26 and include genetic and environmental factors. Although our study was cross-sectional and therefore could not determine a temporal relationship between household stressors and children’s symptoms, there is considerable published evidence of adversity, trauma and toxic stress leading to compromised health and developmental outcomes10 11 26 as well as later consequences of deprivation of relational experience in infancy and early childhood.21 30 31 Some conditions in neurodevelopmental paediatrics have genetic aetiology and a specific genetic diagnosis may be possible in nearly half of children with intellectual disability (ID) although rarely in those in ASD unaccompanied by ID32; however, the majority of developmental, behavioural and emotional disorders are considered multifactorial.1 11 15 26 33 There is no longer debate about nature versus nurture but rather awareness of the complex interplay of genetics and environment26 32 33 and probable differential susceptibility to positive and negative environmental influences.34 Epigenetics suggests mechanisms for environmental trauma and deficit impinging on the foetus and child and for transgenerational transmission of trauma.16 26
Greater awareness of the likely contribution of psychosocial factors to the aetiology of childhood mental health disorders may lead to widening the scope of potential interventions for their prevention and management.35 Current strategies for prevention of childhood morbidity largely focus on promotion of maternal physical health in pregnancy.26 33 36 Psychosocial preventative strategies for childhood mental health disorders might include antenatal screening for family vulnerabilities, with particular emphasis on parental mental health disorders such as anxiety, mood and personality disorders as well as parental trauma history and history of compromised attachment, plus other family factors, notably interpersonal violence and parental substance abuse.5 6 In addition to addressing parental needs directly, evidence of family vulnerabilities could be followed by implementation of targeted supports such as mother–infant attachment interventions,5 6 intensive nurse home visiting for vulnerable new parents37 and whole family intervention for domestic abuse.38 The most effective parenting programmes to prevent child behaviour problems are found to be those which increase warmth and nurturing and to decrease harsh discipline and over-involved overprotective parenting.9 In terms of management, paediatric practice for childhood mental and developmental disorders currently includes psychotropic medication39 and referral for educational supports and therapies.40 A psychosocial approach could include ACE screening in paediatric clinics11 12 followed by targeted interventions such as parenting interventions, child–parent psychotherapies and childhood trauma therapies.1 3 5 6 41
In summary, this study supports the hypothesis that childhood mental health disorders, including developmental, behavioural and emotional problems, may be suggestive of family stressors rather than simply due to intrinsic factors in the child. The most prevalent disclosed stressor in this cohort was parental mental illness and the most prevalent symptomatology, behavioural disturbance. This awareness might broaden the scope of strategies for prevention and management of childhood mental health disorders in this population, which might eventually lead to reduction in chronic trajectories of mental health disorders.2
This study has several strengths. It includes the whole cohort of children attending initial appointments at this single regional public community paediatric clinic during 1 year and it describes actual clinical practice at the time. However, there are several limitations. The study has a relatively small sample size and did not differentiate between different groups within the cohort, such as indigenous or culturally and linguistically diverse families, nor did it record measures of socioeconomic status. Findings may therefore not generalise to certain populations. Additionally, there was no standardisation of paediatric enquiry about ACEs which could have biased statistical associations, although it seems likely that ACEs were probably under-reported rather than over-reported. Representativeness of the findings is unknown as there was no available direct comparison of prevalence of household stressor ACEs without suspected abuse or neglect in the wider community or in other clinical populations. Also, differential diagnoses were recorded rather than definitive diagnoses which might have only been established later. Despite these limitations, the preliminary findings of this exploratory study are interesting. Future larger and more comprehensive studies might include systematic screening for ACEs, standardised assessment tools to establish definitive diagnoses plus social and demographic factors to distinguish population groups.
Conclusion
This study showed that in a cohort of community paediatric clinic patients in Australia household stressor ACEs, in the absence of apparent child abuse or neglect, were common and were individually and cumulatively associated with specific clinical symptomatology. Parental mental illness was particularly common and associated with a range of childhood behavioural disturbances. The findings of this single centre retrospective review have potential implications for health services and paediatric practice. Further studies could determine how widely applicable these findings are for clinical practice throughout Australia and elsewhere.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Ethics approval
The study was approved by ACT Health Human Research Ethics Committee Low Risk Sub-Committee. ACT reference: 2021.LRE.00038. REGIS Reference: 2021/ETH00568. The study was performed in accordance with all ethical requirements.
Acknowledgments
The authors would like to thank Professor Lyndall Strazdins, Research School of Population Health, Australian National University, for her support and advice throughout this project.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Concept: HH and MG. Design: HH, MG, ND and KT. Literature review: HH, MG, ND and KT. Data collection: HH, ND and KT. Statistical analysis: ND and KT. Figures and tables: ND. Authorship, drafting and revision: HH, ND, KT and MG. All authors approved the final manuscript as submitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.